Article Text

Statistics from Altmetric.com
- Bronchoscopy
- cough
- tracheobronchopathia osteochondroplastica
- confocal endomicroscopy
- airway epithelium
- rare lung diseases
A 65-year-old Filipino man presented with a cough productive of heavily bloodstained sputum for 1 month with slight weight loss. He had chronic obstructive pulmonary disease from a 60 pack-year smoking history, having quit 20 years previously, and his chronic mild dyspnoea was stable. He had been treated for pulmonary tuberculosis 9 years previously but had not travelled abroad for 3 years. He had no other medical or family history and was taking no medications.
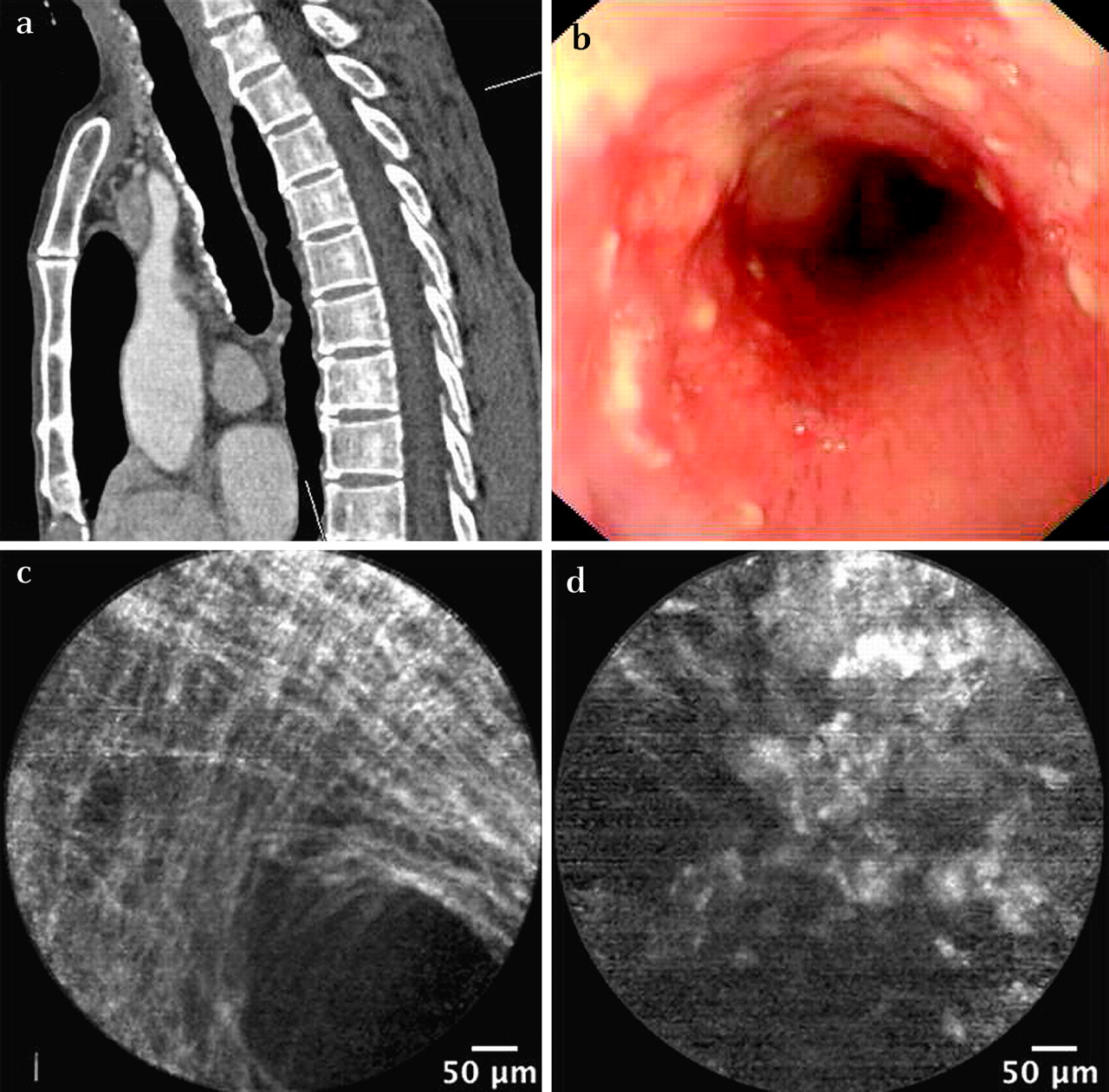
Investigations included a high-resolution CT scan (figure 1a) and fibreoptic bronchoscopy (figure 1b). Coliforms and a co-amoxiclav-resistant Proteus were cultured from purulent bronchoalveolar lavage (BAL) fluid from the left lower lobe. Both organisms were sensitive to ciprofloxacin. The BAL fluid was negative for mycobacteria, and cytology showed no malignancy. Endobronchial biopsy samples (EBBx) showed mucosa with active chronic inflammation including eosinophils and some dystrophic calcification. Bronchoscopic probe-based confocal laser endomicroscopy (pCLE) of a tracheal lesion is shown in figure 1d. pCLE is a new bronchoscopic technique which detects autofluorescence to obtain near histological quality real-time in situ images of the alveolus1 and bronchial basement membrane.2
{kind=link}
(a) Sagittal section of the CT scan of the thorax; (b) fibreoptic bronchoscopic view of the trachea with sparing of nodularity posteriorly; (c) typical probe-based confocal laser endomicroscopy (pCLE) reticular pattern of normal basement membrane of trachea compared with (d) pCLE appearance of this patient's anterior trachea.
Question
What are the abnormalities of the CT scan of the thorax, fibreoptic bronchoscopy image and the pCLE image? What are the possible diagnoses?
See page 353 for answer
Footnotes
Funding Imperial College's pCLE hardware was partially funded by its RT-ISIS grant from the EPSRC.
Competing interests None.
Patient consent Obtained.
Ethics approval This study was conducted with the approval of the regional ethics committee 09/H0708/18.
Provenance and peer review Not commissioned; externally peer reviewed.
Linked Articles
- Pulmonary puzzle
- Airwaves