Article Text

Statistics from Altmetric.com
The epidemiological associations between illness and nitrogen dioxide may be the consequence of confounding by particle numbers
In 1996 the Expert Panel on Air Quality Standards (EPAQS) recommended an ambient air standard for nitrogen dioxide (NO2) in the UK of 150 ppb measured hourly.1 This recommendation, like those for carbon monoxide (CO) and sulphur dioxide (SO2) that had preceded it, was based on human toxicology rather than on epidemiology. The EPAQS was unable to find evidence that these gases were likely to be toxic to humans at the recommended concentrations. However, at the time of the NO2 recommendation there was already epidemiological evidence that effects on populations rather than individuals might be associated with much lower concentrations and the EPAQS recommended that steps be taken to reduce annual average concentrations, although without proposing a long term standard. The UK government has subsequently adopted, as targets to be achieved by 2005, World Health Organization NO2 guideline standards of 105 ppb (200 μg/m3) over 1 hour and 21 ppb (40 μg/m3) as an annual average, the latter having been based on possible relationships between exposure to the gas and respiratory illness in children.2 Achievement of a long term standard does, of course, have the desirable consequence of reducing peaks and therefore short term exccedences. However, compliance with a very low average concentration of NO2 implies a substantial reduction in the concentration of the primary pollutant released from vehicle exhausts—that is, nitric oxide (NO). Since NO reacts with ozone to form NO2, lower concentrations will result in raised urban ozone concentrations, a gas that also has known toxic effects on the lungs and that, until now, has been seen primarily as a rural pollutant in the UK.
Progressive reductions in pollution are welcomed by many because of a belief that human health and the ecology of the planet will benefit, but it must be remembered that they are attained at a cost to industry and thus to society. That cost may be offset by reductions in health expenditure, by increases in life expectancy and crop productivity, and by opportunities for the innovative in designing more efficient engines and fuels. The components of this equation can at present only be estimated very uncertainly, therefore setting tight standards tends to be an act of faith, typically driven by political balancing of the exhortations of pressure groups on both sides. This makes it particularly important to attempt to quantify the health effects of pollutants, a process that has traditionally been based on known toxicological effects but now increasingly relies on epidemiological relationships.
TOXIC EFFECTS OF NITROGEN DIOXIDE: EPIDEMIOLOGY OR TOXICOLOGY?
Scientific confusion arises from the different viewpoints of toxicologists and epidemiologists which may be illustrated by considering NO2. Human inhalation challenge studies have shown that normal healthy individuals do not show adverse effects to NO2 below concentrations of about 2000 ppb (about 4000 μg/m3). Asthmatic subjects may react to concentrations as low as 250 ppb (about 500 μg/m3), either by alterations in bronchial reactivity or by increased sensitivity to inhaled allergens. Such subclinical changes might reasonably be expected to be associated with occasional exacerbations of asthma in very susceptible individuals in an exposed population. However, it is difficult to imagine that concentrations less than half of this could be responsible for clinically measurable episodes of illness, or that concentrations around a fifth of this could cause chronic health problems. While epidemiological studies have sometimes been able to detect associations that suggest health benefits may accrue by adhering to standards set at such very low concentrations, the overall message from these studies is confusing. For example, the WHO review in 20003 concluded that “the most consistent general impression is of increased respiratory illness in older children”. The report goes on to speculate that such episodes may set the scene for chronic lung disease in later life. This conclusion was weighted by consideration of studies of children living in houses with and without gas cookers. However, such studies have shown equivocal results, one meta-analysis having shown a significant effect4 and another not.5,6 As we have shown, gas cooking may entail very high acute exposures to both NO2 and particles.7 In fact, the heterogeneity of epidemiological findings with respect to NO2 led the UK Department of Health’s Committee on the Medical Effects of Air Pollutants to conclude in 1998 that this pollutant should not be included in its quantitative estimates of the effects of pollutants on health.8 It is plain that the evidence on which the long term NO2 standard is based is insecure.
Epidemiological studies usually rely on the assumption that the exposures of all individuals in the population may be taken as those measured by one or a few city centre monitors. This method has the incidental effect of obscuring any threshold that may be present,9 leading to the possibly erroneous conclusion that there is no absolutely safe level of the gas in population terms. The epidemiologist may argue, with justification, that the toxicologist can only study relatively small numbers of subjects who are well enough to take part, and thus cannot comment on effects on the very vulnerable who comprise a small but critical proportion of any population studied. Faced with such conflicting evidence, what action should governments take?
CONFOUNDING AND EFFECT MODIFICATION
There are many problems in interpreting epidemiological studies of air pollution, but perhaps the most important are confounding and effect modification. There are relatively few important sources of pollution in cities—vehicles, industrial and domestic combustion processes outdoors, and cooking and smoking indoors. All produce a mixture of pollutants including particles, NO (oxidised by atmospheric ozone to NO2), and CO. Particles, with which adverse health effects have been associated most consistently, are usually measured as PM10 (the mass of those that are less than 10 μm in aerodynamic diameter), a metric that includes a varying contribution from non-combustion sources. There are plausible hypotheses to explain the association of exposure to low concentrations of particles with both respiratory and cardiovascular illness and death10–12; this cannot be said of any associations between NO2 and such illnesses.
It is apparent that, in urban pollution episodes, particles and NO2 rise and fall together, making it difficult or impossible to separate their effects. Some studies have been particularly interesting in this regard. One observed an association between the triggering of implanted defibrillators and ambient concentrations of both particles and NO2, the latter effect appearing to be somewhat stronger.13 If NO2 was indeed responsible, individuals with such devices would be well advised to avoid entering kitchens containing gas cookers where NO2 concentrations may rise to 1000 ppb (approximately 2000 µg/m3).7 Another study in eight European cities showed that the association between particle concentrations (as PM10) and acute cardiac episodes was eliminated by controlling for NO2, strongly suggesting confounding.14 Effect modification is suggested by a study in which greater effects of NO2 on mortality occurred in cities with higher PM10 concentrations,15 and by another that has shown a stronger effect of particles (measured as black smoke, a metric roughly equivalent to PM4.5) on respiratory admissions when NO2 concentrations were simultaneously raised.16
This issue of confounding and/or effect modification is important. If a demonstrated association is a consequence of confounding by some other toxic substance, the effect of one may be ignored in terms of standard setting, whereas if the association is explained by effect modification, both toxic substances require regulation. Of course, if both come from a common source, regulation of one may regulate the other, but this cannot be guaranteed as changes in technology may increase one by reducing the other. Is it conceivable that these confusing associations are the consequence of confounding of all the above mentioned apparently toxic substances by one as yet unmeasured substance? We think that they may be, the confounder being the number of particles and thus the surface area presented to the lung.
PARTICLE NUMBERS AND NITROGEN DIOXIDE
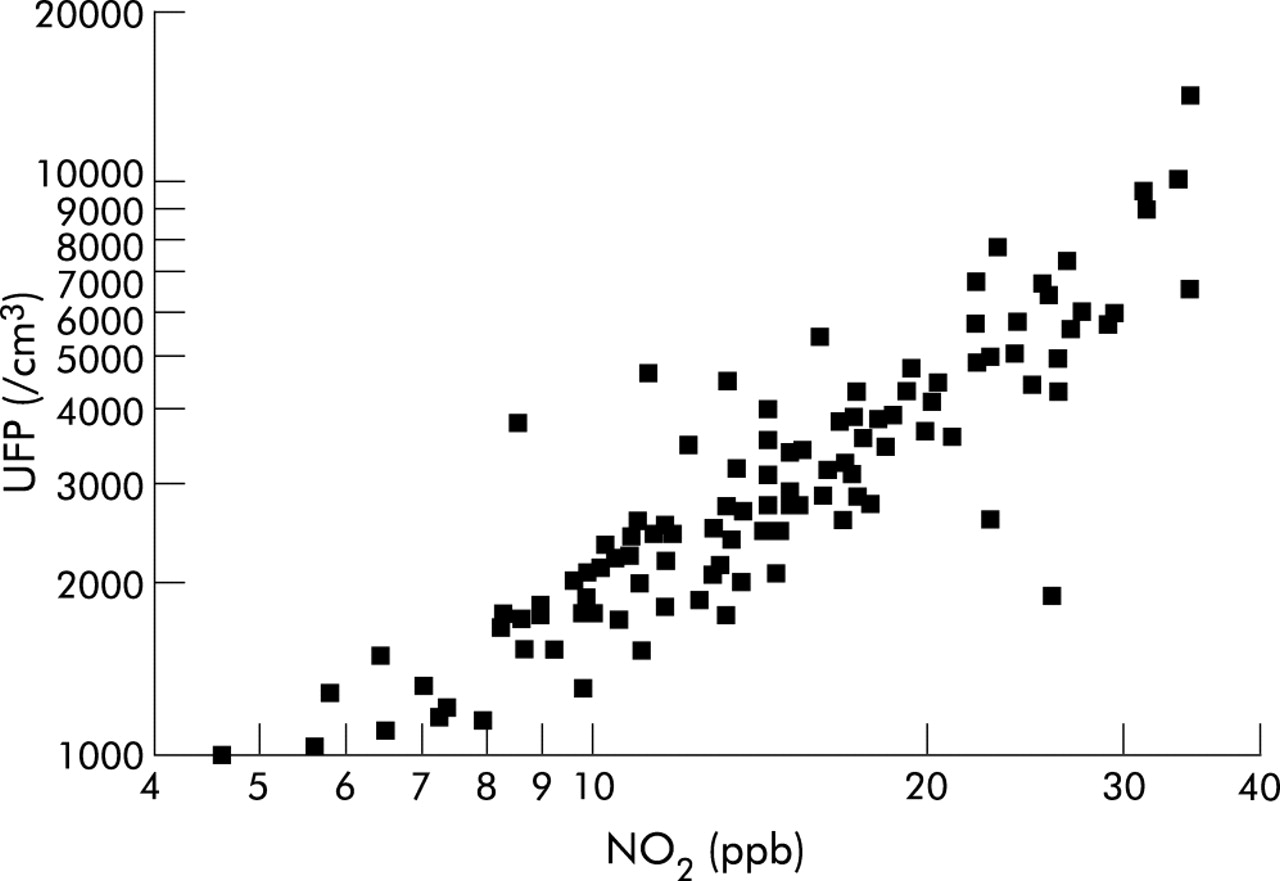
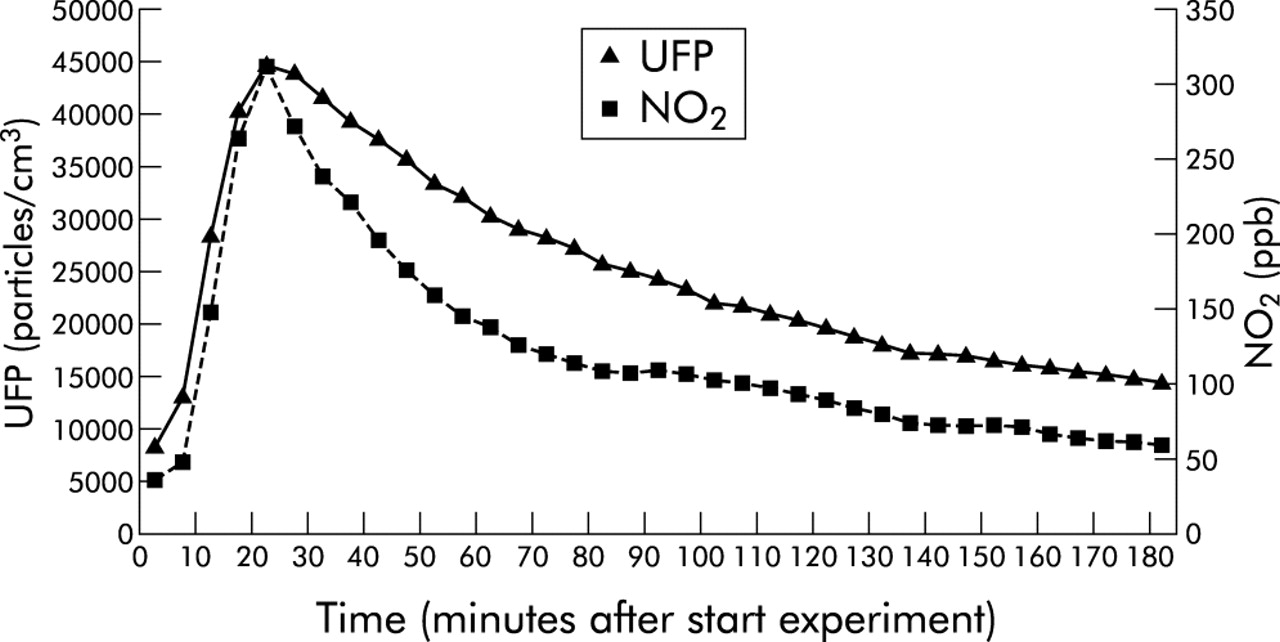
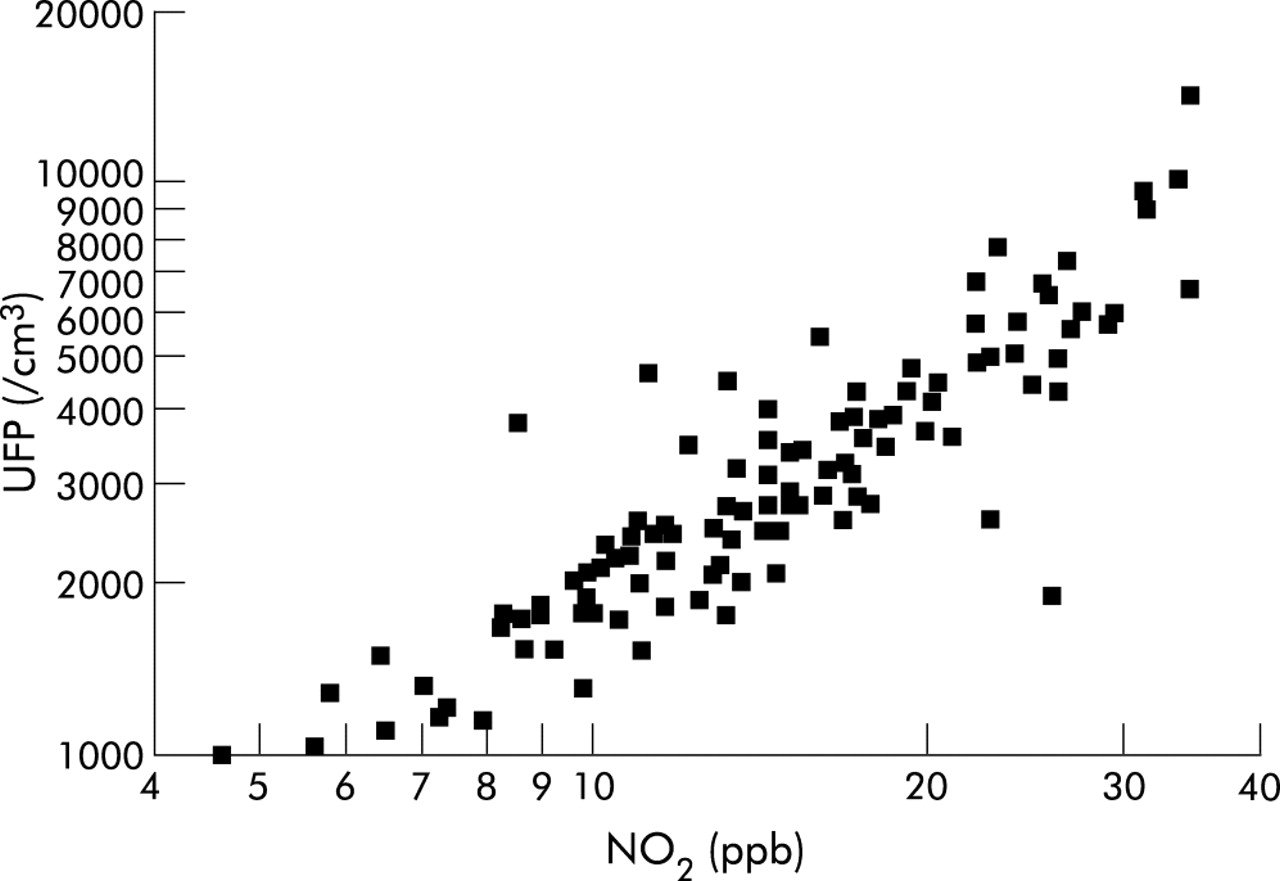
The particulate aerosol we inhale comprises particles of all sizes ranging from organic matter like pollen grains some 10 μm or more in diameter to primary combustion particles of 10 nm diameter. The smallest tend to aggregate rapidly into what are still submicron particles. When we measure particles as mass—for example, PM10, PM2.5 or black smoke—the greatest contribution comes from the largest particles, but the greatest number of particles by far are the submicron ones. These ultrafine particles are generated, as is NO, by the combustion process, and therefore the two pollutants (and NO2) are likely to correlate closely. We have carried out two separate investigations during which we have measured simultaneously particle number counts (by TSI 3934 scanning mobility particle sizer) and nitrogen oxides (by ML9841A chemoluminescent analyser). The first of these was in an unventilated laboratory during a study of the effects of electric and gas cooking on indoor pollution, the pollution source being a gas cooker.7 Figure 1 shows the close relationship between the two pollutants when derived from a common source. The second was a study of the effects of exposures to particles on the health of individuals with chronic lung disease over the course of 6 months, the measurements being made at a background site in Aberdeen city. Here we found a very striking association between concentrations of nitrogen oxides and the number of particles of <100 nm aerodynamic diameter measured simultaneously (fig 2); this association was stronger than the corresponding associations with particles measured as mass (table 1). These associations are so close that it would be impossible to distinguish their effects in epidemiological studies. Thus, if NO2 in these environments is measured as an index of pollution and is shown to be associated with health effects, these effects could equally be due to the numbers of particles.
Pearson correlation coefficients for the logged daily outdoor concentrations of NO2, NO, particle numbers, PM2.5 and PM10 in Aberdeen
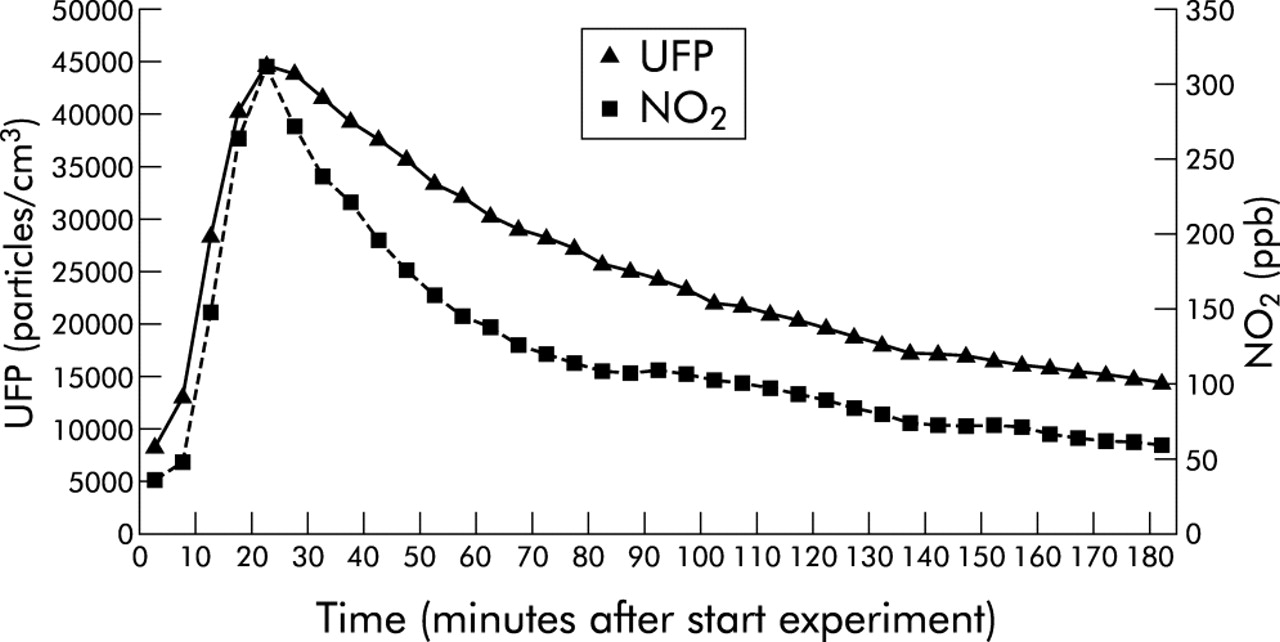
Indoor ultrafine particle number (UFP) and nitrogen dioxide (NO2) concentrations in an unventilated laboratory over 3 hours during and after burning of one gas ring for 15 minutes (r = 0.97).
{kind=link}
{kind=link}
Relationship between mean outdoor air 24 hour counts of particles <100 nm in diameter (UFP) and nitrogen dioxide (NO2) concentrations in parts per billion. Data represent 6 months of continuous side by side measurement.
IS PARTICLE NUMBER THE VILLAIN?
The number of particles is an important and usually unmeasured confounder in studies in which both particle mass and NO2 are associated with health effects. We are left to argue, from toxicological considerations, which of these is likely—at the known concentrations to which individuals are exposed—to cause the observed effects. At the moment there is evidence for toxic effects of ultrafine particles at quite low concentrations in animals.17 Relatively few studies have related particle numbers to cardiorespiratory illness, the most detailed being those of Wichmann’s group in Erfurt, Germany. They have shown a somewhat weaker correlation between gases and particle numbers than us, but they have shown associations between numbers, NO2, SO2, CO and cardiorespiratory deaths.18,19 It should be noted that, in contrast to most UK cities, domestic heating in Erfurt makes an important contribution to particulate pollution in the winter and SO2 concentrations are higher. Wichmann and colleagues concluded that the apparent effects of the gases were likely to be a result of confounding.
PARTICLES AS MICROBES – AN HYPOTHESIS
A plausible explanation for this toxicity is as follows. We hypothesise that the lung reacts to particle numbers rather than mass, since its primary defensive role is to counter invasion by microorganisms which may be inhaled in large numbers but never in high mass. The first requirement of the lung is to kill organisms in situ and/or to transfer them to lymph nodes where immune responses may be concentrated, and ingestion by macrophages is central to this mechanism. Ultrafine particles, however, may evade this and pass directly through the alveolar wall, thus being able directly to influence endothelial cell structures. Both macrophages and endothelium release mediators that have local and more general influences, one of which is to signal that bloodstream invasion may be imminent; a systemic reaction—the acute phase response—is a consequence. If we assume that the lung treats small particles as microorganisms, it is reasonable to propose that its response relates to numbers rather than mass. By altering blood coagulability and possibly by destabilising atheromatous plaques, this systemic response may be responsible for the acute cardiac effects seen in vulnerable individuals. It seems far more plausible that these effects are a response to the number of particles rather than to NO2, for which no comparable hypothetical explanation of effects at such low concentrations has yet been proposed.
The toxicity of microorganisms does not, of course, depend entirely on the numbers inhaled; their inherent ability to initiate cell damaging reactions or to resist defences is critically important. Similarly, not all inhaled particles would be expected to be equally toxic—for example, quartz and titanium dioxide. Thus, something other than particle numbers needs to be invoked to explain their effects, and this is likely to be the nature of the surfaces they present to the lung’s defences.12,17 A further step in explaining toxicity therefore requires consideration of surface properties. However, in urban air the very smallest particles make an overwhelming contribution to the total surface area, so measurement of one represents the other.
We propose that the observed associations between ill health and NO2 at low concentrations in the ambient air are the result of confounding by particle numbers. We have earlier hypothesised that a systemic response to particle inhalation is responsible for the acute cardiorespiratory effects,10 a suggestion for which there is now considerable support.20 This hypothesis also explains the association between air pollution and long term risk of heart disease,21 since it proposes that particles cause inflammation and thus an increase in the blood of markers such as C reactive protein and fibrinogen that have been associated with increased cardiac risk. Here we propose that this is a consequence of the lung’s evolutionary system of defence against microorganisms. From a practical point of view, we now need to explore relations between particle numbers and illness in order to obtain evidence upon which a number standard might be considered. For the moment, however, it seems likely that in situations such as those in most UK cities where motor vehicles are the main source of pollution, measurement of NO2 is the simplest means of assessing exposures to particle numbers and, conveniently for epidemiologists, this can be done on a personal basis.
The epidemiological associations between illness and nitrogen dioxide may be the consequence of confounding by particle numbers