Article Text

Statistics from Altmetric.com
The first British Thoracic Society (BTS) statement on mesothelioma was published in 2001 by a Working Party of the Standards of Care Committee of the BTS1 in response to a request by the National Health Executive in England. In the last 5 years enough progress has been made to justify the preparation of a second statement. The most significant updates are in sections reviewing radiology and biopsy techniques and interpretation, the potential use of tumour markers, chemotherapy, radical treatment and the roles of the specialist nurse and multidisciplinary team approach in management. Recent major clinical trials are also reviewed.
As before, this updated statement was written by a Working Party of clinicians with an interest and experience in the disease with the aim of compiling a document to assist in the management of pleural and peritoneal malignant mesothelioma in the UK. We were again assisted by co-opted specialists, including radiologists, pathologists, nurses and oncologists, whose full details are given in Appendix 1. The draft was reviewed by the whole membership of the BTS and also sent to expert groups and patient representatives for whose comments we are grateful. Our statement is the result of this consultation process.
This statement is compiled primarily for clinicians who may be involved in caring for patients with mesothelioma and is based on literature searches and reviews by members of the Working Party responsible for particular sections. However, like its predecessor, it is not strictly evidence-based as we did not attempt a comprehensive review of all available literature. Moreover, in most aspects of this subject there are still no randomised trials on which to base guidelines. The management of mesothelioma remains subject to debate and variations in practice, so we have retained the term “statement” rather than “guidelines” in this revision.
This statement should be read in conjunction with the Mesothelioma Framework produced by the Department of Health’s Lung Cancer and Mesothelioma Advisory Group.2 The latter document is directed mainly at Strategic Health Authorities, cancer networks, primary care trusts and NHS trusts in England, and provides advice on how to organise mesothelioma services in order to improve standards of care to a uniformly high level.
Summary of key points
Malignant mesothelioma will increase in incidence over the next 5–10 years. It is inexorably progressive with a very poor 5-year survival and a median survival of 8–14 months.
Malignant mesothelioma should be considered in any patient with either pleural fluid or pleural thickening, especially if chest pain is present. Prompt referral to a respiratory physician for further assessment is indicated.
Where a chest radiograph is suggestive of malignant pleural disease, a copy report should ideally be sent to a designated member of the lung cancer multidisciplinary team, usually the chest physician, and preferably electronically or by fax.
The pathological diagnosis of a diffuse malignant mesothelioma is not always straightforward and interpretation should always be taken in context with full knowledge of the clinical history, examination findings and radiological appearance.
Where there is diagnostic uncertainty or where radical treatment is considered, cases should be referred to a specialist multidisciplinary team.
An appropriately trained specialist nurse should be involved from the outset to support the care of the patient and liaise between hospital services, primary care and specialist palliative care services.
The diagnosis should be communicated skilfully and sympathetically with a clear picture of the disease and the management plan. This information should be communicated to the general practitioner immediately.
Written information about the disease, its medicolegal aspects and relevant organisations should be available to the patient and family.
Early pleurodesis is a key aim for symptom control and prevention of the development of a trapped lung.
Palliative radiotherapy provides pain relief in about half of all patients.
All patients with mesothelioma and performance status 0–2 should have the opportunity to discuss the merits of chemotherapy with a specialist experienced in the use of chemotherapy for malignant mesothelioma.
Supportive and palliative care aims to provide relief from pain and other physical symptoms and to respond to emotional, psychological, social and spiritual needs.
Dyspnoea, cough and other symptoms should be managed according to palliative care guidelines.
Radical surgery should, for the foreseeable future, only be considered within randomised trials such as MARS and MesoVATS.
Peritoneal mesothelioma is related to asbestos exposure but is less common than pleural mesothelioma.
EPIDEMIOLOGY
The incidence of mesothelioma in Great Britain has been increasing rapidly since cases began to be systematically recorded in the late 1960s when the mesothelioma register was established.3 Latest available projections of the future burden of the disease in Britain suggest that the annual number of deaths will peak at between 1950 and 2450 deaths per year sometime between the years 2011 and 2015.4 The model suggests that for men in the highest risk birth cohorts—that is, those born in the late 1930s or early 1940s—mesothelioma may account for around 0.7% of all deaths. Although highly uncertain, long-range predictions suggest that around 65 000 deaths from mesothelioma may occur over the next 50 years. There is widespread variation in the incidence of malignant mesothelioma in England: two Strategic Health Authorities have <30 cases annually while two have >100 cases per year.2
Asbestos fibres are the cause of most cases of mesothelioma. Evidence from two British studies suggests that the proportion of men with mesothelioma directly attributable to occupational asbestos exposure may be about 85%,5 6 and this is consistent with evidence from studies in other countries.7 8 However, mesothelioma can also result from para-occupational exposures (for example, women who have laundered their husband’s overalls) and non-industrial environmental exposures.6 Furthermore, there is some evidence to suggest that the rate of “spontaneous” mesotheliomas each year—that is, deaths which would have occurred even if the industrial exploitation of asbestos had never taken place—is around one per million or about 30 men and a similar number of women per year in Britain.
Mesothelioma can be induced by other non-asbestos fibres such as erionite found in rock in certain areas of Turkey.9 The suggestion that Simian virus 40 (SV40),10 which was found to contaminate polio vaccines administered in the 1950s and early 1960s in Great Britain, is a contributory factor has been refuted by recent studies.11 12
The latency period between first exposure to asbestos and death from mesothelioma is typically very long. One review of over 20 epidemiological studies which documented latent periods reported a median latency of 32 years, very few cases with latency of <20 years and nearly one-third of cases with latency of >40 years.13 A more recent British study reported a mean latency of 41 years (range 15–67).5
Analyses of the British Mesothelioma Register by occupational group and geographical area support the conclusion that the continuing increase in deaths from mesothelioma in Great Britain is a consequence of past occupational asbestos exposure.3 These analyses show that occupations and geographical areas with the highest mesothelioma risks tend to be those clearly associated with heavy past asbestos exposures—for example, within industries such as shipbuilding, railway engineering, asbestos product manufacture and construction. However, analyses of trends in risk over time are consistent with the notion that deaths due to specific high-risk industries of the past are levelling off or falling more recently as other sources of exposure have developed over a wider range of occupations and geographical areas. Workers with the highest risks today are likely to be those subject to incidental exposures during the course of their work such as building maintenance workers; nevertheless, the lifetime risk for most individuals is extremely small.4
Measurements of airborne asbestos levels in buildings containing asbestos in good condition are typically several orders of magnitude below the lowest exposure levels seen in occupational cohorts of asbestos workers, and ambient asbestos levels in the general environment are likely to be even lower.6 Quantitative risk models derived from cohort studies may not be valid at these low levels, but they do indicate that substantial numbers of cases are unlikely to result from such exposures.13 14
The risk of mesothelioma varies considerably in relation to the type of asbestos fibre, and there is evidence that the risks in relation to amphibole asbestos are considerably higher than chrysotile.15 Chrysotile was by far the most widely used type of asbestos in the UK. However, amosite was also used in substantial quantities and crocidolite to a lesser extent, as reflected in the figures on UK imports of the different asbestos types.16 Thus, many historical exposures are likely to have involved a mixture of fibre types, and the widespread use of chrysotile together with amphiboles in many asbestos products suggests that current exposures are likely to continue to do so.
Many thousands of workers have been exposed to asbestos fibres and have heard about the potential dangers, although only a small proportion will develop life-threatening disease as a result. These workers have justifiable anxiety about their future and may seek reassurance from the medical profession with routine chest radiographs. Although often requested by patients, annual radiographs of previously exposed individuals cannot be recommended. The current responsibilities of employers of workers who might be exposed to asbestos during the course of their work are laid out in the Control of Asbestos Regulations 2006 (Statutory Instrument 2006 No 2739).17 These Regulations describe the requirements for record keeping and medical surveillance, together with the actions to be taken if an employee is found to have a relevant disease.
The information now available about the risk of mesothelioma according to occupation, geographical area, birth cohorts and type of asbestos and age first exposed may allow advice about potential future risks in individual cases to be given in general and qualitative terms. Unfortunately, there is currently no basis for providing more specific advice to individuals.
CLINICAL FEATURES
Typically, presentation is either with chest pain, dyspnoea or both.18 19 The pain is usually dull, diffuse, occasionally pleuritic and characteristically worsens during the course of the illness. The pain may be described as heaviness or aching in the shoulder, arm, chest wall and upper abdomen. It sometimes has neuropathic components because of entrapment of intercostal thoracic, autonomic or brachial plexus nerves. Occasional patients are encountered who present with persistent chest wall pain with clear chest radiographs who develop either pleural masses or effusions during follow-up in the subsequent months. Cough may occur, particularly in patients presenting with a pleural effusion, but this is not usually a prominent symptom.
In the early stages, dyspnoea is usually caused by a pleural effusion but later may be due to the restrictive effects of pleural thickening. A chest wall mass, weight loss, abdominal pain and ascites (due to peritoneal involvement) are less common presentations. Profuse sweating may occur.
Occasionally the diagnosis is suspected following a routine chest radiograph. Pleural thickening or a mass may be visible on the chest radiograph after drainage of a presenting effusion and may prompt consideration of the diagnosis, as may the finding of other manifestations of asbestos exposure such as pleural plaques. Bilateral disease occurs rarely at presentation but is not uncommon in the terminal phases. A further uncommon but well-recognised presentation is with a pneumothorax.
Unlike carcinoma of the bronchus, presentation with cervical adenopathy, haemoptysis, non-metastatic syndromes and symptoms due to distant metastases is unusual. The disease is more likely to progress by local extension than haematogenous spread. Direct involvement of mediastinal structures is common, but hoarseness and superior vena caval obstruction only rarely cause major symptoms. Dysphagia, if it occurs, tends to be a pre-terminal event.
Sometimes patients present with acute pleuritic chest pain and a small effusion but initial investigations may fail to give a diagnosis. The patient may then remain symptom-free for many months until recurrence of the fluid or the development of chest pain leads to further investigation and ultimate diagnosis of mesothelioma.
Physical signs depend on the type of disease involvement and include signs of pleural thickening and effusion together with restriction of expansion of the hemithorax. Finger clubbing occurs more commonly in mesothelioma than in other forms of asbestos-related pleural disease.20 Pericardial involvement may result in signs of tamponade. Weight loss may be prominent as the disease progresses.
Progression of the disease may be variable. Some patients have periods of apparent stability while others have relentless rapid deterioration.
Key points
Malignant mesothelioma should be considered in any patient with either pleural fluid or pleural thickening, especially if chest pain is present.
It may occasionally present with persistent unexplained chest pain and a normal chest radiograph.
Symptomatic metastatic disease is unusual at presentation.
PROGNOSIS
Several studies have reported survival data, some measuring survival from date of onset of symptoms and others from date of definite diagnosis. A series reported from the UK showed an overall median survival from symptom onset of 14 months and confirmed a worse prognosis in those with sarcomatoid histology.5 A study of asbestos insulation workers in the USA showed that, among 141 cases of pleural mesothelioma, 36% died within 6 months, 64% within 12 months and 94% within 24 months of the onset of symptoms. Of 244 cases of peritoneal mesothelioma, 55% died within 6 months, 88% within 12 months and 98% within 24 months of onset of symptoms. In this series the median survival for pleural mesothelioma from onset of symptoms was 10 months and from diagnosis 5 months.21 The high number of patients with peritoneal mesothelioma is thought to reflect very heavy asbestos exposure in this group of workers. Survival data are difficult to interpret and compare because they vary in starting point. Future studies should be based on date of acceptance of diagnosis by a multidisciplinary team.
There are prognostic factors that allow some refinement of prediction of life expectancy. Apart from non-epithelioid histology, the most important poor prognostic factors are male gender, advanced stage disease,22 23 poor performance status, leucocytosis and thrombocytosis. Several scoring systems such as the European Organisation for Research and Treatment of Cancer (EORTC) and Cancer and Leukaemia Group B (CALGB) have been used extensively in chemotherapy trials and have been validated as useful in estimating survival.
The few patients who survive >3 years are almost exclusively from the epithelioid group. Distant metastases occur commonly, although they are usually late and seldom cause problems. Yates et al5 reported their presence in >50% of cases at autopsy and with similar frequency in all histological types, although Law et al23 found them more commonly in the sarcomatoid variety.
Key points
Median survival varies from 8 to 14 months in different studies.
Survival should be measured from the date of acceptance of the diagnosis by a multidisciplinary team.
The disease is inexorably progressive with a very poor 5-year survival.
Epithelioid tumours have a better prognosis than other cell types.
DIAGNOSIS
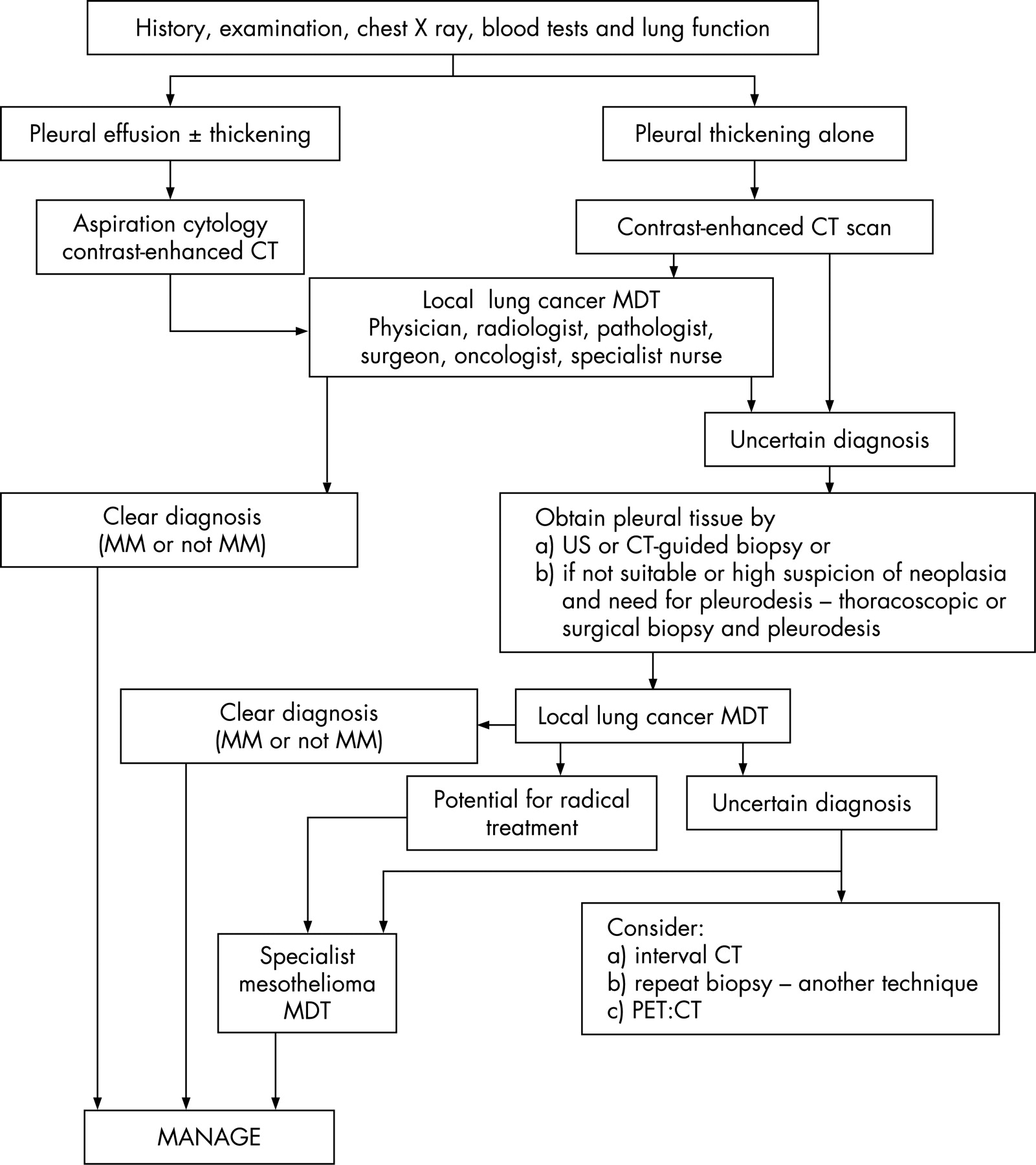
Diagnostic strategy
It is essential to use the combination of history, examination, radiology and pathology to reach a diagnosis of malignant mesothelioma. All the above elements are needed, and the overall strategy for diagnosis in a case of suspected mesothelioma is therefore to ensure that the patient has the relevant investigations rapidly and efficiently. In a clear-cut case it is possible to inform a patient of the diagnosis immediately a biopsy result is available, but in many cases it is usually wiser to defer this until the case has been discussed in detail at the local multidisciplinary team meeting and a diagnosis agreed. This also enables a preliminary view about management strategy to be given.
History
The history of asbestos exposure is very important but is often not recalled by the patient at presentation. An occupation may strongly suggest that exposure has occurred, although it is important to recognise less obvious occupations such as teacher, decorator and assembly worker. The possibility of neighbourhood or para-occupational exposure needs to be considered.
Further history at other stages of the patient’s pathway is often much more informative after the patient has been able to think over his or her employment history. It has to be borne in mind that many patients will be attempting to recall working conditions up to 50 years earlier.
Physical examination
Physical examination does not usually aid the differential diagnosis. Occasionally tumour tissue may be felt between the ribs.
Investigations
Plain chest radiographic abnormalities may strongly suggest a malignant process. The key investigations subsequently are a pleural tap if an effusion is present and a contrast-enhanced CT scan, together with an appropriate biopsy procedure24 (see later sections).
A pleural tap can be performed in the outpatient clinic and the fluid should be sent for cytology and immunocytochemistry on a cell block. The risk of seeding from a pleural tap site is thought to be low, but the site of a puncture should be recorded.
If the clinical, radiological and cytological results subsequently support a diagnosis of mesothelioma, then this can be accepted. However, although immunocytochemistry can reliably show that cells are mesothelial in origin, it may be difficult to distinguish malignant from highly reactive cells. A biopsy is recommended if there is doubt about the diagnosis on radiological or clinical grounds as cytology may be unreliable.
In general medical practice it is not uncommon for a patient to have an undiagnosed pleural effusion despite a pleural tap and a CT scan. A potential diagnosis of mesothelioma may not have been considered by the managing team. For this reason, institutions are recommended to have a policy of prompt referral of such cases for a respiratory opinion.
A biopsy is required if the diagnosis is not clear after the pleural tap and a CT scan. The choices of technique are an ultrasound or CT-guided percutaneous pleural biopsy, or a thoracoscopic biopsy. Blind biopsy techniques are quick to perform and inexpensive, and are thus still used in some centres. However, a recent study has shown that a blind Abrams’ punch biopsy is less effective at reaching a diagnosis for pleural thickening than a CT-guided biopsy, and the latter is therefore preferable.25
Thoracoscopy is appropriate where there is pleural fluid and the technique facilitates not only complete drainage of the fluid and biopsy, but also immediate talc pleurodesis where appearances are clearly malignant. Where there is doubt about the macroscopic appearance, pleurodesis should be deferred. Biopsies are essential even if the appearances seem to be those of normal pleura.
The multidisciplinary team and the uncertain diagnosis
Sometimes, even after cytology, biopsy and a detailed multidisciplinary team discussion, there is uncertainty about the diagnosis of malignant mesothelioma. This may be strongly suspected but not diagnosable with certainty, and this uncertainty should be communicated to the patient even if he or she has to be managed with mesothelioma in mind. Occasionally, as indicated above, a diagnosis of malignant mesothelioma only emerges after time and repeated CT scans and/or biopsies. This strategy needs to be carefully explained to patients and their families. Most equivocal cases eventually turn out to have mesothelioma when indolent disease is accompanied by negative biopsies. Persistent effusions are unusual in the presence of benign pleural thickening. Difficult cases should be reviewed by a regional specialist multidisciplinary team as recommended in the Department of Health Framework document.2
The points made in this section are summarised in the diagnostic algorithm shown in fig 1.
Key points
A detailed occupational history is essential.
Any patient in whom mesothelioma is suspected should be promptly referred to a respiratory physician for further assessment.
Pathological confirmation of the diagnosis is recommended unless the patient is frail or has extremely advanced disease.
Negative pleural biopsy and cytological results do not exclude mesothelioma and should lead to further investigation or follow-up.
CT scanning plays a key role in the diagnosis of mesothelioma.
CT scanning, ultrasound and thoracoscopic biopsy are the preferred techniques for obtaining tissue.
DIAGNOSTIC IMAGING
Imaging at presentation
The initial chest radiographic appearances of malignant mesothelioma may range from normal in early disease to complete opacification of a hemithorax, depending on the amount of pleural thickening and fluid present. The pleural thickening may manifest itself as discrete pleural nodules or may progressively encase the lung. The mediastinum may be either central or displaced. There should be a clear rapid referral mechanism in place if either a chest radiograph or a CT scan suggests malignant pleural disease.2 A second copy of the radiologist’s report should ideally be sent electronically or by facsimile to a designated member of the lung cancer multidisciplinary team, usually the chest physician.
Ultrasound can be very useful in identifying pleural abnormalities. The presence of a pleural effusion acts as an acoustic window, enabling the detection of intrapleural and intrapulmonary processes. Pleural effusions and thickening can be readily appreciated by ultrasound and discrete malignant nodules may be seen.26 Ultrasound-guided biopsy of pleural thickening and drainage of effusions are well-established safe techniques.
Computed tomography (CT)
Contrast-enhanced CT is the primary imaging modality used for the evaluation of suspected malignant pleural disease. Malignant or inflammatory pleural disease enhances strongly, and the contrast allows differentiation between thickened pleura, effusion and underlying aerated or collapsed lung. Multi-detector CT allows a scan of the entire chest to be performed in <10 s. A scan delay of 60 s allows optimal visualisation of pleural disease while still allowing assessment of the mediastinal nodes and liver in the portal venous phase of enhancement. A standard protocol includes the liver and adrenal glands but should also include the lower abdomen and pelvis if there is a past history of malignancy in the abdomen or pelvis or clinical evidence of pelvic disease.
Leung et al studied 74 consecutive patients with diffuse pleural disease.27 CT features used to distinguish malignant from benign pleural disease were (1) circumferential pleural thickening, (2) nodular pleural thickening, (3) parietal pleural thickening >1 cm, and (4) mediastinal pleural involvement. The specificities of these findings were 100%, 94%, 94% and 88%, respectively. The sensitivities were 41%, 51%, 36% and 56%, respectively. While the positive predictive value of these signs is high, their absence does not exclude a diagnosis of pleural malignancy and CT cannot reliably differentiate malignant mesothelioma from other malignancy. Others have confirmed that the commonest features of malignant mesothelioma are circumferential nodular lung encasement, pleural thickening with irregular pleuropulmonary margins and pleural thickening with superimposed nodules.28 These CT findings may be important for a working diagnosis in patients with poor performance status who do not want, or are unfit for, invasive biopsy procedures. Coincidental pleural plaques are found on the CT scan in approximately 20% of patients with malignant mesothelioma and there may be other features of asbestos exposure. Conversely, in many patients there may be no other radiological evidence of asbestos exposure. CT evidence of distant metastases is rare at presentation in malignant mesothelioma.
Magnetic resonance imaging (MRI)
MRI has a limited role in the evaluation of malignant mesothelioma. Pleural malignancy enhances avidly with use of gadolinium-based contrast material. Anatomical and morphological MRI features similar to those seen at CT are used to differentiate between benign and malignant disease and to establish local invasion.29 30 MRI, with its ability to scan in any plane, has been used to accurately assess resectability prior to radical surgery.31 Multi-detector CT scanning is able to provide detailed reconstructions, thus giving MRI only a limited role in evaluating patients with questionable areas of local tumour extension at CT or in whom intravenous administration of iodinated contrast material is contraindicated.
18F-fluorodeoxyglucose positron emission tomography (FDG PET)
In a limited number of patients where conventional imaging and biopsy have been either unhelpful or equivocal, FDG PET may be useful in differentiating benign from malignant pleural disease and might guide choice of biopsy site. Duysinx et al studied 63 patients with FDG PET and found this to have a sensitivity for detecting malignancy of 96.8% and a specificity of 88.5%.32 False positive results may be seen in cases of parapneumonic effusion and both tuberculous and uraemic pleural disease.33 Care should be taken with patients who have previously undergone talc pleurodesis, as the inflammatory process caused by this procedure can also cause a false positive result.34 It is not known how long the scan remains positive after pleurodesis.
The standardised uptake value (SUV) is used as a semi-quantitative measure of the metabolic activity of a lesion. The SUV is significantly higher in malignant mesothelioma than in benign pleural diseases such as inflammatory pleuritis and asbestos-related pleural plaques.35 However, some cases of malignant mesothelioma are low-grade tumours and may not be avid on FDG PET. SUV can be taken at any time following injection of the tracer. There is neither an accepted time at which SUV should be measured in patients with malignant mesothelioma nor a particular threshold able to differentiate between benign and malignant disease. Volume measurements can be taken using SUV, and this offers the potential for assessing disease response following either chemotherapy or other novel treatment.
Imaging and staging
The TNM staging system proposed by the International Mesothelioma Interest Group (IMIG) is used for assessing patients with potentially resectable disease (see Appendix 2 available online at http://thorax.bmj.com/supplemental).36 This staging system was designed as a surgical tool and may not be completely applicable to imaging. CT and MRI overall have fairly similar accuracies for staging malignant mesothelioma, but both techniques may underestimate the stage of the disease.37 Although both techniques have been shown to be sensitive in predicting resectability,38 CT is routinely used in view of its speed of examination and availability. Radiological staging may be required for entry into a clinical trial.
Mediastinal nodes are commonly involved by mesothelioma and, as with the staging of lung cancer, CT has limited accuracy for detecting mediastinal node involvement. FDG PET also appears to be relatively poor at distinguishing mediastinal nodal metastases from adjacent mediastinal pleural involvement, although a high SUV seems to correlate with the presence of N2 disease.39 Co-registration of CT with PET images, “CT-PET”, may have a role in assessing these patients but studies are limited at present.40 Currently, mediastinoscopy is normally performed before radical surgery to exclude patients with N2 disease. CT-PET may have a complementary role aiming to detect occult metastatic or N3 disease.
Imaging and assessment of disease response
The assessment of disease response is important in evaluating treatment in both everyday clinical practice and clinical trials. Solid organ tumours are normally measured with either bidimensional41 or unidimensional measurements. Response Evaluation Criteria in Solid Tumours (RECIST)42 is based on the assumption that tumours are generally spherical, and that a maximal unidimensional measurement correlates well with an overall reduction in tumour size. Malignant mesothelioma tends to grow as a rind around the chest wall, and changes in tumour bulk tend to manifest as changes in tumour thickness perpendicular to the chest wall rather than the maximal tumour dimension. Studies have shown discrepancies between tumour measurement in malignant mesothelioma using the World Health Organisation (WHO) and RECIST criteria.43 The RECIST criteria have now been modified and validated with particular reference to malignant mesothelioma.44 Semi-automated three-dimensional measurements have been described but are not routinely used.45 Difficulties arise in patients who have undergone pleurodesis as this causes an inflammatory response and subsequent pleural thickening. If the patient is to undergo chemotherapy following pleurodesis or surgical decortication, a baseline scan should be performed immediately before this.
Key points
Where a chest radiograph is suggestive of malignant pleural disease, a copy report should ideally be sent to a designated member of the lung cancer multidisciplinary team, usually the chest physician, and preferably electronically or by fax.
The multidisciplinary team should have a mechanism in place to follow up these reports.
In patients with suspected malignant pleural disease, a chest CT scan should be performed before pleural biopsy or thoracoscopy.
CT scanning cannot reliably differentiate malignant mesothelioma from other causes of malignant pleural disease.
Ultrasound-guided pleural aspiration should be used as a safe and accurate method of obtaining fluid if the effusion is small or loculated.
MRI has a limited role in patients with malignant mesothelioma (over and above multi-detector CT).
PET scanning may be useful in differentiating benign from malignant disease but further studies are needed.
Radiological staging of patients with malignant mesothelioma should occur before radical surgery and before clinical trial entry.
PATHOLOGY
Pathological diagnosis may be obtained from cytology or histology. Cytological diagnosis is based either on sampling of effusion fluid or by percutaneous fine needle aspiration cytology of a region of pleural thickening. In specialist centres the sensitivity of the former technique can be up to 76% and the latter 78%.46 Immunocytochemistry can be applied to the cytological material (including cell blocks), which can fairly reliably identify that the cellular content is mesothelial. However, where there is poor clinical and radiological correlation, the pathological diagnosis should be based on tissue biopsy due to difficulties in distinguishing malignant mesothelioma cells from reactive mesothelial cells and other pleural malignancies in fluid.47 48
Percutaneous core biopsy may provide sufficient material on which to confirm a diagnosis of malignant mesothelioma and to perform ancillary studies. This is reported to have a higher yield (86% sensitivity and 100% specificity) than closed Abrams’ or Cope needle biopsy which only offers a sensitivity of 21–43%.49 Others have shown a sensitivity for needle biopsy of 60% with a single attempt and 85% with repeat biopsies.50 Thoracoscopy has a sensitivity of over 90% with a low complication rate (10%).51
Separation of benign from malignant mesothelial proliferations
Establishing the nature of the mesothelial proliferation present in a sample is one of the most challenging aspects of diagnosis. The US-Canadian Mesothelioma Reference Panel have produced guidance in this area.52 It recommends a conservative approach, with equivocal cases being labelled “atypical mesothelial hyperplasia” or similar and, if appropriate, further tissue sampled.
Pathologists should be prepared to submit samples for expert review in cases of diagnostic difficulty.
Histopathological classification
The precise cell of origin of malignant mesothelioma is unclear, but it is now suggested that tumours arise from submesothelial cells that have the ability to differentiate along diverse lines. Numerous histopathological subtypes of diffuse malignant mesothelioma have been described (table 1). It is important for the pathologist to be aware of these alternative forms but the WHO classification advises that, as these various subtypes have no particular prognostic significance, tumours should be classified into one of three main types: epithelioid, sarcomatoid (with desmoplastic mesothelioma being a particularly aggressive form of the latter) and biphasic. Classification into these three main groups is important as it may alter management.
Ancillary tests
Despite the numerous publications describing the usual morphological features of mesothelioma, confirmation requires support from additional studies which may include histochemical, immunohistochemical and electron microscopic analysis. Unfortunately, no single stain or test can unequivocally confirm or exclude a diagnosis of mesothelioma and a panel of tests are performed, particularly when trying to differentiate mesothelioma from adenocarcinoma.
Epithelioid mesotheliomas can mimic (and be mimicked by) several other tumours, most frequently metastatic adenocarcinoma. The most useful differentiating histochemical stains are those for mucins (table 2). Two recent publications have reviewed the immunohistochemical profile of mesotheliomas compared with metastatic adenocarcinoma, which most commonly spreads from the lung.53 54 These confirm that a panel of antibodies is required and the most useful are listed in table 2. Most pathologists employ a limited combination of these markers with a mixture of positive and negative results indicating the diagnosis.
Immunohistochemistry is useful in differentiating between reactive and neoplastic mesothelial proliferations, particularly in cytological preparations or superficial biopsies. EMA is more likely to be positive in a neoplastic process, with more extensive p53 expression, while desmin decorates reactive mesothelial cells preferentially.55 The usual markers, however, are of much less value when trying to confirm the diagnosis of sarcomatoid malignant mesothelioma, where the sensitivity and specificity is much lower.56
Immunohistochemistry is useful in differentiating mesotheliomas from tumours other than adenocarcinoma (whether primary or metastasic). Table 3 lists most of the important differential diagnoses of diffuse malignant mesothelioma with antibodies that may aid diagnosis.
Electron microscopy can play a role in the diagnosis by demonstrating the long slender microvilli of mesotheliomas that contrast with the broader, blunt microvilli of adenocarcinomas.
Specific types of mesothelial tumour
Well-differentiated papillary mesothelioma
This is a rare tumour (fewer than 50 cases in the world literature) that deserves mention because of its confusing name and more indolent course and prolonged survival. Asbestos exposure has been reported in some cases of this tumour, but a genuine epidemiological association has not been established. It can be either localised or diffuse, and is more commonly found in the peritoneum of women. However, cases in the pleura are recognised (where the sex bias is less obvious).57
The typical microscopic appearance is of broad fibrovascular cores covered by a single layer of bland mesothelial cells. There are no mitoses and invasion of the underlying stroma is not seen. If this diagnosis is made pathologically but the disease proves to be rapidly progressive, then the correct diagnosis is probably a diffuse epithelioid malignant mesothelioma and further tissue sampling is indicated.
Multicystic mesothelial proliferation
This is a multicystic proliferation of mesothelial cells which has previously been considered by some to be a reactive process and by others a benign neoplasm. It is most frequently seen in the abdomen of premenopausal women and is sometimes associated with previous surgery or endometriosis. It is characterised by multiple fluid-filled cysts lined by flattened mesothelial cells. It is now clear that the condition can also be found both in the pleura and in men. It invariably has a benign clinical course.
Solitary fibrous tumour (localised fibrous tumour/mesothelioma)
This is an uncommon spindle cell neoplasm that occurs most frequently in the chest but which can occur in virtually any site in the body; it should not be confused with localised malignant mesothelioma58 which is a localised form of the diffuse tumour described above. Solitary fibrous tumour characteristically arises from the visceral pleura, is well circumscribed and may be pedunculated. The microscopic hallmark is a bland spindle cell proliferation arranged in a “patternless pattern”. The cellularity is variable with cellular areas interspersed with hypocellular collagenised regions. Vessels are usually prominent. Tumour can be infiltrative and cells are usually positive for CD34 and bcl-2 while cytokeratin antibodies are almost always negative. These tumours generally are benign, although occasionally malignant behaviour is recognised. The malignant varieties tend to cellularity, cellular atypia and high mitotic activity (>4 per 10 high paver fields). Approximately 15% of cases have hypertrophic pulmonary osteoarthropathy and 15% have recurrent hypoglycaemia.
Key points
The pathological diagnosis of a diffuse malignant mesothelioma is not always straightforward and interpretation should always be taken in context with full knowledge of the clinical history, examination findings and radiological appearance.
Pleural fluid cytology and histology of blind biopsy specimens have a low diagnostic yield for mesothelioma but are important initial steps in differential diagnosis.
Pathologists should attempt to specify the histological type of mesothelioma.
A selection of special stains must be used to confirm mesothelial origin of a tumour and aid differentiation from other pleural neoplasia.
Pathologists should be prepared to submit samples for expert opinion in cases of diagnostic difficulty.
Role of serum markers in diagnosis
Two recent studies have described the use of serum markers in the diagnosis of malignant mesothelioma. Osteopontin is a bone-derived glycoprotein that is overexpressed in a number of malignancies including lung, breast, gastrointestinal tract and ovarian tumours. In patients with malignant mesothelioma, serum levels were raised in comparison with both healthy subjects and asbestos-exposed controls. The levels in exposed individuals with pleural plaques with pulmonary fibrosis were raised, but not to the same extent as those measured in patients with malignant mesothelioma. Using a cut-off value of 48 ng/ml, the assay had a sensitivity of 78% and a specificity of 85%.59 Soluble mesothelin-related proteins (SMRP) are thought to be involved in cell adhesion and its monoclonal antibody binds to normal mesothelial cells, mesotheliomas and some ovarian cancers. Raised SMRP levels were found in 37 of 44 individuals with malignant mesothelioma (sensitivity 84%) and only 3 of 160 patients with fibrosis, benign pleural disease and non-mesothelioma cancers. Seven of 40 individuals with asbestos exposure had raised SMRP levels, and 3 of these apparently disease-free individuals subsequently developed malignant mesothelioma.60 Epithelioid tumours were more likely to be associated with raised SMRP levels, and the levels appeared to correlate with tumour size and fell following surgical debulking. A recent larger prospective multicentre study61 confirmed higher levels of SMRP in malignant mesothelioma in comparison with both other malignancies with pleural involvement and benign asbestos pleural disease; however, the test was less sensitive than initially reported when distinguishing pleural metastasis from malignant mesothelioma (58%). There was a clearer distinction when SMRP was measured in pleural fluid and the levels tended to be considerably higher.
Diagnosis at an early stage of the disease should, in theory, improve prognosis and identify patients for whom radical treatment might be indicated. The rate of false positives in exposed healthy individuals must cause concern and would engender considerable anxiety in a cohort of exposed men who, in all likelihood, will never develop malignant mesothelioma. Before large-scale screening with tumour markers can be recommended, prospective studies will be required to confirm sensitivity and specificity of the test, the natural history of an individual with an increased level of the marker and, ideally, demonstrate an impact of the measurement on mortality. Meanwhile, data on SMRP might be studied prospectively as part of treatment trials. As yet, SMRP is not widely available commercially; however, a markedly increased level in an appropriate clinical context might increase diagnostic confidence in cases where tissue diagnosis is equivocal.
Cytogenetics may play a part in diagnosis in the future but at present is not routinely used as no single alteration or pattern of alterations is diagnostic.
MANAGEMENT
General management
Patients with mesothelioma should be discussed by a lung cancer and mesothelioma multidisciplinary team, be under the care of a specialist (usually a respiratory physician) and have a specialist nurse allocated to them. The multidisciplinary team should include core professionals as defined in the National Institute for Health and Clinical Excellence (NICE) guidelines and Department of Health Framework document. Where there is diagnostic difficulty or a possibility of radical treatment, the patient should be discussed at a specialist multidisciplinary team meeting.
The specialist nurse (usually a lung cancer or mesothelioma specialist nurse) should facilitate the pathway of care for the patient and the family throughout the illness, ensure good liaison between hospital services and primary care, and ensure access to specialist palliative care services as required. Patients should be advised who to contact in case of need. Further details are provided in a later section.
The diagnosis should be communicated skilfully and sympathetically. A clear picture of the disease and what to expect, including a realistic prognosis, should be given to the patient and, if appropriate, to families and carers. It is important to avoid a nihilistic approach. A copy record of the consultation could be offered to the patient. Immediate communication with the general practitioner should include the known extent of the disease, what was said to the patient and the management plan.62
Ongoing follow-up by a member of the multidisciplinary team (usually the respiratory physician) is recommended, even if there is no change in treatment, as it provides an opportunity for further discussion including issues of compensation and benefits, symptom control and provision of support. There should be continuing close liaison with the general practitioner and primary health care team. The patient should have access to a specialist nurse, usually the nominated key worker.
The relatives or carers and the general practitioner should be warned, at an appropriate stage, that a Coroner’s post mortem examination will nearly always be required after the death of a patient with mesothelioma, and all deaths have to be reported to the Coroner (in Scotland the Procurator Fiscal).
Key points
A patient with mesothelioma should be discussed at a multidisciplinary team meeting and be under the care of a specialist.
Where there is diagnostic uncertainty or where radical treatment is considered, cases should be referred to a specialist multidisciplinary team.
An appropriately trained specialist nurse should be involved from the outset to support the care of the patient and liaise between hospital services, primary care and specialist palliative care services.
The diagnosis should be communicated skilfully and sympathetically with a clear picture of the disease and the management plan. This information should be communicated immediately to the general practitioner.
Written information about the disease, its medicolegal aspects and relevant organisations should be available to the patient and family.
Assessment of psychological, social and spiritual needs of patient and family/carers should be undertaken at key points during the disease pathway. Information should be offered about appropriate support services.
The general practitioner should be reminded that all deaths have to be reported to the Coroner (in Scotland the Procurator Fiscal); an inquest is usually required.
Treatment strategy
Essential management points to be considered on diagnosis are:
Management of the pleural effusion.
Indications for prophylactic radiotherapy to intervention sites.
Indications for chemotherapy.
Immediate supportive care requirements.
Compensation issues.
Suitability for radical surgery.
Suitability for clinical trial entry.
Referral to the specialist multidisciplinary team.
Organisation of care
This is discussed in detail in the Mesothelioma Framework document.2 The difficulties facing patients with malignant mesothelioma are diagnosis, palliation, allocation to a specialist treatment (eg, surgery), recruitment into randomised trials and obtaining advice about social, financial and legal issues. For these reasons, every patient has a right to have his or her disease considered by an experienced team with a declared interest in this cancer. The essential composition of such a team is a chest physician, a radiologist, a pathologist, a surgeon, an oncologist and a cancer nurse, all with expertise and an expressed interest in the disease. The team should have ready access to specialist palliative care services and opinions. If local services cannot meet these criteria, we consider it advisable that arrangements are made for the routine referral of patients with malignant mesothelioma to a team with the required attributes (the specialist multidisciplinary team). Such referrals could be managed by record review, teleconferencing or by attendance at a clinic, depending on individual circumstances. Ongoing care should continue to be with the local team if it is in the patient’s best interest. We recommend that initially a network of identified cancer nurses with expertise in malignant mesothelioma is established to facilitate such referrals at a local level.
There is no evidence to support the contention that the management of a given number of cases of malignant mesothelioma per year provides evidence of expertise, either in individuals or a multidisciplinary team. An expressed and evident special interest may be more important, although we consider that teams diagnosing fewer than 10–15 cases per year are unlikely to develop and retain the attributes required. A typical specialist multidisciplinary team would be expected to discuss a minimum of 25 cases annually.2
Surgery
The role of surgical resection in malignant mesothelioma is very uncertain. Two approaches can be taken. The more radical is extrapleural pneumonectomy (EPP) (sometimes referred to as pleuropneumonectomy). The less radical approach is a debulking operation (sometimes known as cytoreductive surgery), which is either performed at open thoracotomy or by video-assisted thoracic surgery (VATS). Both are being tested in randomised controlled trials (see below). Radical treatment should only be considered for patients with epithelioid tumours (although the Mesothelioma And Radical Surgery (MARS) trial has not made this distinction owing to unreliability of sampling techniques).
Extrapleural pneumonectomy (EPP)
This procedure was first described in the 1970s63 and its aim is to eradicate all macroscopic disease, ideally with good clearance margins. The nature, extent, pattern of growth and proximity to major organs makes mesothelioma impossible to eradicate completely without resection of all the parietal and visceral pleura, the underlying lung, the diaphragm and the pericardium. Even then there are often doubts about resection margins. Operative mortality is 4–9%,64 but significant complications from EPP occurs in over 60% of patients.63–67 A median survival of 19 months following this radical operation with adjuvant chemotherapy and radiotherapy has been reported in the largest series, but this is based on highly selected patients reported with no indication of the denominator from which they were drawn and no control or comparative group.68 There have been further series reporting “improved” outcomes following EPP with multi-modality therapy, but again with no control group.69–74
The absence of randomised controlled trials on the role of EPP for mesothelioma led a recent systematic review of surgical management to conclude that the role of EPP could not be defined.75 Currently, the MARS trial is recruiting in the British Isles in its pilot phase. This is a randomised study comparing EPP against no EPP surgery within the context of trimodality therapy (neoadjuvant chemotherapy and postoperative radical hemithoracic radiotherapy). The aim is to randomise 50 patients to determine the feasibility and acceptability of performing an adequately powered randomised trial. The primary outcomes of the main trial will be survival and quality of life. Patients being considered for EPP should be treated within the context of the MARS trial.
With potentially high mortality and morbidity, patients must undergo rigorous preoperative assessment before being considered for EPP. Fitness for surgery should be assessed according to standard BTS guidelines for pneumonectomy in lung cancer76 and should also include preoperative echocardiography to assess pulmonary artery systolic pressure.
Preoperative staging with a CT scan, PET scan and mediastinoscopy are important to assess resectability (T1–3, N0–1, M0). Together with positive resection margins and non-epithelioid subtypes, involvement of mediastinal lymph nodes has been shown to be a negative predictor of survival following EPP.69 77 A PET scan, particularly integrated CT-PET imaging, identifies distant metastasis78 but is less good at identifying positive N2 lymph nodes owing to the proximity of the mediastinal pleura. Accurate staging of the mediastinum by mediastinoscopy is therefore required in the MARS trial in all patients for whom randomisation is being considered for possible EPP.
As most patients who present are usually already in advanced stages of the disease, only a minority may be eligible for EPP. Of these, it is likely that only a few will benefit from radical treatment with or without EPP. Until there is clear evidence for EPP, it cannot be recommended as the treatment of choice.
Debulking/cytoreductive surgery
This less radical approach, which can be performed by VATS or thoracotomy, involves removal of as much of the tumour burden as possible without removing the underlying lung, diaphragm or pericardium. Where the underlying lung is trapped by the diseased pleura, re-expansion of the lung may be possible following decortication,79 thereby offering symptom control with less morbidity.80 VATS pleurectomy/cytoreductive surgery has been reported to be effective in preventing fluid recurrence81 and may also be associated with increased survival82 although, like EPP, it has not yet been tested in a randomised trial.
MesoVATS is an ongoing randomised study in the UK comparing VATS cytoreductive surgery against bedside talc pleurodesis in patients with a pleural effusion secondary to proven or suspected mesothelioma. Survival and quality of life are outcome measures, as well as clinical and cost effectiveness. Patients who present with a pleural effusion and have been deemed ineligible for the MARS trial should be considered for the MesoVATS trial.
Patients referred for radical surgery should be aware that it is likely to be either preceded or followed by chemotherapy and followed by hemithorax radiotherapy (“trimodality therapy”). Patients should be given realistic information about the perioperative risks and the chances of long-term survival.
Key points
There are no randomised control trials to establish the role of radical surgery.
Radical surgery should only be considered within a randomised trial.
Surgery should be concentrated in centres where there is experience in performing extrapleural pneumonectomies.
The present claims for benefit are for surgery within multimodality therapy.
Patients should be aware of the potential for trimodality treatment and be given realistic information about outcomes.
Management of pleural effusion
One of the central aims in the management of patients with symptomatic pleural effusions caused by mesothelioma is to achieve an early and successful pleurodesis. This helps symptom control and a trapped lung is less likely to occur if the procedure is performed promptly. Given the low diagnostic yield of bedside procedures, early thoracoscopy also gives an opportunity to obtain a definitive histological diagnosis.
Thoracoscopy82–86 is an extremely useful technique in the evaluation and management of undiagnosed exudative pleural effusions. As well as providing a high diagnostic yield, it allows complete drainage of the pleural space followed by talc poudrage. Thoracoscopy can be performed under conscious sedation (usual for medical thoracoscopy) or under general anaesthesia (VATS). Complications are uncommon but include pleural space infection and surgical emphysema.
If the patient is either too frail to undergo thoracoscopy or a firm diagnosis has already been made, talc slurry pleurodesis may be performed via an intercostal drain.87 88 Occasionally, simple repeated pleural aspirations without pleurodesis may be appropriate for very frail patients with advanced disease. Small-bore indwelling catheters and drainage systems are an alternative in these circumstances.
Chemical pleurodesis should be performed via a small bore (16–18F) that should be flushed regularly with normal saline to maintain its patency.89 Lignocaine (3 mg/kg; maximum 250 mg) should be administered intrapleurally just before sclerosant administration. In addition, premedication should be considered to alleviate anxiety and pain associated with pleurodesis. Satisfactory apposition of the parietal and visceral pleura should be confirmed radiographically. There are no data to suggest that suction improves the success rate,89 or that frequently changing the position of the patient improves either dispersion of the sclerosant or the success of pleurodesis.90 91
Currently the most effective freely available pleurodesis agent is sterile talc.88 89 92 93 The dose of the talc should not exceed 4 g, and it should be calibrated to avoid the rare risk of the development of adult respiratory distress syndrome.94 The intercostal tube should be clamped for 1 h after sclerosant administration and, in the absence of excessive fluid drainage (>250 ml/day), removed 24–48 h later. Recent data showed no difference in success rates between talc poudrage and talc slurry.94
Pleuroperitoneal shunts have been used where pleurodesis has failed and for trapped lung. However, there is a high complication rate, including shunt occlusion and infection. Their use is therefore diminishing.95
Unfortunately, a minority of patients will have a trapped lung at presentation or develop the problem during the course of their disease. If asymptomatic, partial entrapment and little fluid production then no action is required. However, if there are symptoms due to rapid re-accumulation of pleural fluid, an indwelling pleural catheter may be inserted. Catheters may be inserted as day case procedures and, with nursing support, allow patients and their carers to drain their effusions at home. They have been shown to significantly improve the quality of life96 and, with regular drainage, up to 45% of effusions undergo spontaneous pleurodesis.97 Complications are rare but include pleural infection.96 97
None of the available techniques designed to control pleural effusion in malignant mesothelioma is universally successful. Patients and their carers should therefore be made aware of the risk of re-accumulation of pleural fluid and the methods of accessing the secondary care team—for example, via the cancer nurse specialist.
Key points
Early pleurodesis is a key aim for symptom control and prevention of the development of a trapped lung.
Thoracoscopy is an extremely useful diagnostic and therapeutic tool.
Calibrated talc is the pleurodesis agent of choice.
Indwelling pleural catheters are useful for symptom control in cases of trapped lung or where chemical pleurodesis has failed.
Radiotherapy
Radical radiotherapy as a single modality
Irradiation of the pleura is limited by toxicity to the lung and adjacent organs, particularly the bowel and stomach (for left-sided lesions). A retrospective review of 123 patients treated with hemithoracic radiation after surgical debulking of tumour (pleurectomy/decortication) showed actuarial local control at 1 year of 42% and median survival of 13.5 months.98 The lung is sensitive even to small (palliative) doses of radiation and, in the same study, severe pulmonary toxicity was found in 10% with 1.5% treatment-related mortality at 1 month.98 Hemithoracic irradiation with the lung in situ is therefore not indicated for mesothelioma.
Palliative radiotherapy
Retrospective and uncontrolled series suggest that radiotherapy can help relieve pain from mesothelioma in around half of patients treated.99 100 Although there are no controlled trials evaluating the effect of field size on pain relief, retrospective studies suggest that palliation of pain can be achieved by treating relatively small volumes of symptomatic disease and using short schedules (1–5 fractions) of radiotherapy.100 Such schedules have been shown to be effective and well tolerated in palliating pain from both thoracic and non-thoracic malignancy. Large-volume radiotherapy has been used, but its effect is usually short-lived and the need to treat bulky disease (necessitating long treatment times) limits its usefulness.101 Patients with symptoms from mediastinal infiltration such as superior vena caval obstruction have a poor response to radiotherapy and generally have a short survival. Other means of palliation are more appropriate.
Radiotherapy as an adjunct to surgery
When extrapleural pneumonectomy is performed, radical radiotherapy is viewed as an integral part of management and can result in local control in 60–90% of patients, albeit with significant (though acceptable) morbidity.71 102 Radiotherapy can be delivered with conventional techniques or with the aid of sophisticated planning and treatment hardware and software known as intensity modulated radiotherapy (IMRT).103 Preliminary evidence suggests that this technique does result in improved local control over more traditional ways of delivering radiotherapy.104 However, no improvement in overall survival has yet been observed as most patients develop progressive disease outside the hemithorax.
Prophylactic radiotherapy
There is a risk of seeding of malignant cells in the scar produced by biopsy and/or pleural drainage, resulting in an uncomfortable subcutaneous tumour (although ulceration is rarely a problem). A randomised trial has shown that the risk of this happening can be reduced from 40% to 0% by the administration of three fractions of radiotherapy to scars.81 Observational studies and first principles suggest that such treatment should be given promptly (ie, as soon as the wound has healed). However, a recent randomised trial showed that the use of a single dose of radiotherapy was ineffective for prophylaxis, with recurrences occurring in 10% of sites not given radiotherapy compared with 7% of sites irradiated.105 However, this study did show a trend for a lower prevalence of seeding with less invasive procedures. The overall rates of drain site disease were 22% for Abrams’ needles, 9% for thoracic drains and 4% for fine needle aspirates. Similarly, a randomised study of 61 patients given three fractions of radiotherapy showed no difference in the prevalence of wound seeding at 1 year with 23% of treated patients and 10% of controls developing scar-related nodules (N Rourke, personal communication).
The current recommendation is that patients of good performance status (and therefore longer survival) who have chest wall wounds should be referred for radiotherapy promptly and treated with a three-fraction schedule. If the patient is of poor performance status and/or has had a minimally invasive procedure, radiotherapy may be unnecessary. Tumour seeding can also occur in the abdominal wall after paracentesis for secondary thoracic malignant mesothelioma or primary peritoneal mesothelioma; however, the potential need for either repeated drainage of ascites or the use of an implantable device may limit the usefulness of prophylactic radiotherapy to this site.
Key points
Palliative radiotherapy provides pain relief in about half of all patients.
Palpable masses respond to radiotherapy in about half of all patients.
Breathlessness and superior vena caval obstruction rarely respond to radiotherapy.
Prophylactic radiotherapy may reduce chest wall implantation following invasive procedures, but may be most applicable for patients with a better prognosis and after more invasive procedures.
Chemotherapy
In general, palliative chemotherapy should be considered for all patients with performance status 0–2. The objective response rate that should be expected is of the order of 20–40%, and two randomised controlled trials have shown significant differences in survival between regimens, implying that chemotherapy may extend the life expectancy of some patients with mesothelioma. This benefit is not dependent on age, stage or histology.106–108 However, there is no randomised trial evidence showing that chemotherapy confers better quality of life and survival than supportive care without chemotherapy. These questions continue to be addressed by the BTS study MSO-1 which compares two alternative chemotherapy regimens (single agent vinorelbine and the combination of mitomycin, vinblastine and cisplatin) with active symptom control alone.109 This trial closed to recruitment with 409 patients randomised and the results are expected by late 2007.
A number of phase II studies of various chemotherapy regimens have demonstrated both objective response rates comparable to those seen in advanced non-small cell lung cancer and worthwhile palliation of symptoms in half or more of the patients treated (table 4). Symptom relief may occur in patients whose tumours have not shown radiological response as defined by conventional criteria.
There has been considerable interest in a new chemotherapeutic agent for malignant mesothelioma, pemetrexed (Alimta; Eli Lilly). The main evidence supporting its use consists of a randomised study which compared a combination of pemetrexed and cisplatin (PC) with cisplatin (C) alone in patients with mesothelioma. The trial showed that the combination regimen extended median survival by nearly 3 months.106 On the basis of this study, the US Food and Drug Administration (FDA) approved pemetrexed for the treatment of mesothelioma and it has also been licensed for this indication in Europe, including the UK. Inclusion criteria included Karnofsky performance status (PS) ⩾70 corresponding to WHO or ECOG PS 0–1. Part way through the trial folic acid and vitamin B12 supplementation was introduced to reduce toxicity resulting in three patient subgroups: never supplemented (NS), partially supplemented (PS) and fully supplemented (FS). The sample size was substantially increased to ensure adequate statistical power of the FS subgroup; 456 patients were randomised but eight who did not receive chemotherapy were excluded from analysis. Patients in the PC arm received a median of six cycles while those in the C arm received a median of four cycles. NS patients received a median of two cycles on each arm. Median survival in the whole group was 12.1 months with PC and 9.3 months with C (p = 0.02). Among 331 FS patients, median survival was 13.3 months with PC compared with 10.0 months with C (p = 0.05). The investigators reported a tumour partial response rate of 41.3% in the PC arm, but a review by the FDA confirmed only half of these.120 Quality of life data, published in abstract form in 2003, reported a significant improvement in quality of life and symptom relief when compared with cisplatin alone.121 However, full quality of life data have not been published. The subsequent paper reported that 84 patients from the PC arm and 105 from the C arm received second-line chemotherapy which was associated with significant prolongation of survival after adjustment for baseline prognostic factors and treatment received.122 This strengthened the conclusion that first-line pemetrexed prolonged survival since the survival advantage was seen despite the fact that more patients in the C arm had received second-line chemotherapy. The subset analyses performed in this study mean that the results should be interpreted with caution. It is important to note borderline significance in survival advantage in the FS group, as well as the fact that the patients were younger and fitter than most with mesothelioma.
Two phase II studies have suggested that efficacy may be approximately similar when carboplatin (in a dose of area under the curve 5) is used instead of cisplatin in combination with pemetrexed.123 124 The substitution of carboplatin for cisplatin is associated with reduced symptomatic toxicity (particularly nausea and vomiting) and increased ease of administration with less need for prolonged hydration with intravenous fluids. This has the potential to improve quality of life.
Support for the efficacy of antifolates is provided by similar results from a smaller study of cisplatin with or without raltitrexed (another antifolate) in 250 patients with mesothelioma.125 Median overall and 1 year survival with cisplatin vs raltitrexed was 8.8 (CI 7.8 to 10.8) months vs 11.4 (CI 10.1 to 15) months and 40% vs 46%, respectively (p = 0.05). There was no detriment to quality of life from raltitrexed. Unfortunately, the manufacturers do not intend to continue development of raltitrexed for treatment of mesothelioma and may stop production for economic reasons, leaving only pemetrexed in this class in the short to medium term.
The message from the randomised studies of pemetrexed and raltitrexed is that, unless cisplatin alone actually shortens survival—which seems unlikely—these drugs probably do confer a small median survival advantage and, as with any chemotherapy, patients whose tumours respond well to therapy are likely to gain more than average in terms of survival. The effects on quality of life are not yet fully evaluated but appear to be beneficial. Despite the need for caution in interpretation of the data, pemetrexed is an agent with demonstrable clinical efficacy in the treatment of mesothelioma and, as such, it is to be welcomed. It is less toxic than alternatives, particularly when used with carboplatin rather than cisplatin, and easily administered with a 3-weekly outpatient treatment schedule. Pemetrexed is the only drug licensed for the treatment of mesothelioma on the basis of randomised trial evidence and therefore may be considered the drug of first choice, used in combination with cisplatin or carboplatin. Other cheaper agents with useful activity include vinorelbine, gemcitabine, irinotecan and mitomycin, but none has yet been shown to confer a survival advantage in a randomised trial.
All patients who are fit enough to receive chemotherapy (all PS 0–1 and some PS 2 patients) should therefore be given accurate information and should have the opportunity to discuss chemotherapy with a specialist experienced in its use for mesothelioma. Patients who prefer to receive chemotherapy after a discussion of the merits of this form of treatment should be offered it.
Key points
Several chemotherapeutic agents can reduce tumour bulk and help symptoms. The combination of pemetrexed and cisplatin significantly prolongs survival compared with cisplatin alone.
All patients with mesothelioma and performance status 0–2 should have the opportunity to discuss the merits of chemotherapy with either an oncologist or a respiratory specialist experienced in the use of chemotherapy for malignant mesothelioma.
There are no published trials comparing either survival or symptom control in patients treated with chemotherapy or best supportive care. The results of the first such trial (BTS MSO-1) are expected by mid 2007.
Further clinical trials of chemotherapy should be encouraged.
New approaches to treatment
Some new approaches to drug treatment of mesothelioma that may be important in the future are summarised in table 5.
Attempts have been made to improve the outcome after surgery by use of additional treatment modalities. Cytoreductive surgery with intraoperative photodynamic therapy has been studied by several groups with disappointing results.132
Supportive and palliative care
Supportive and palliative care of patients with mesothelioma and their families is very important, given that the disease has a poor and relatively well-defined prognosis and that most patients need symptom palliation from the time of diagnosis onwards. The patient, family and general practitioner may often have difficulty in accepting that palliative care is the only available treatment for the majority of cases. Anger and frustration are common, and there are particular issues in malignant mesothelioma concerning blame for the disease, obtaining benefits and litigation.
The National Institute for Clinical Health and Excellence62 describes supportive care as an umbrella term for services encompassing information giving, self-help and support, user involvement, symptom control, psychological support, social support, spiritual support, rehabilitation, complementary therapies, palliative care, end-of-life and bereavement care. Palliative care is described as the active holistic care of patients with advanced progressive illness. Management of pain and other symptoms and provision of psychological, social and spiritual support is paramount. The goal is achievement of the best quality of life for patients and their families. This document does not present a comprehensive account of supportive and palliative care and symptom relief, and more details can be found in standard references.133 134
Referral of the patient and/or their carers to specialist palliative care services is appropriate for a range of issues. These include unresolved symptoms and complex physical, psychosocial or spiritual needs, and end-of-life and bereavement issues.
Key points
Most patients need symptom palliation from the time of diagnosis onwards.
Supportive and palliative care aims to provide relief from pain and other physical symptoms and to respond to emotional, psychological, social and spiritual needs.
Supportive care and the clinical nurse specialist
Clinical nurse specialists have a central role in providing and coordinating the specialist supportive care needs of patients and carers. This includes liaising with services such as specialist palliative care, dietetics, physiotherapy and the spiritual team where advanced specialist supportive care is needed.
Role of the lung cancer clinical nurse specialist
Patients with malignant mesothelioma and their carers should have access to a lung cancer clinical nurse specialist or, where the local incidence of the disease is high, a mesothelioma clinical nurse specialist. Given the rarity of the disease, the complex support and information needs, it is appropriate for those diagnosed with peritoneal mesothelioma also to have access to the lung cancer clinical nurse specialist.
The role of the clinical nurse specialist includes the following core elements:135
Communication
Information
Coordinated care
Nursing assessment
Patient advocacy
Accessibility
Support
Communication
It is usually the consultant that provides the patient with the diagnosis and an initial outline of management and prognosis, and support from a clinical nurse specialist is crucial at this stage. The clinical nurse specialist should be promptly available for further discussion of these issues with patients and their families and carers, and offer supportive information. Rapid communication with the general practitioner should be ensured and should include details of the known extent of the disease, what was said to the patient and the management plan.
It is not unusual for several members of the lung multidisciplinary team and the general practitioner to be involved in providing medical care, resulting in complex communication pathways that need to be maintained. The clinical nurse specialist should ensure that the patient and/or carer are aware of the need for a Coroner’s post mortem examination and report to the Coroner or Procurator Fiscal and that this is confirmed in writing to the general practitioner.
Information
Patients with malignant mesothelioma and their families should have access to verbal and written information about the disease and its symptoms, end-of-life issues, treatments and the medicolegal implications. Regular contact with the clinical nurse specialist allows a steady flow of information according to the patient’s needs.
Lung cancer clinical nurse specialists have expressed concerns about obtaining up to date information and maintaining knowledge and expertise in the field of mesothelioma. Information and support for nurses to allow them to meet the needs of their patients with malignant mesothelioma is available from the organisations listed in Appendix 3 (available online at http://thorax.bmj.com/supplemental). The clinical nurse specialist should advise (or clarify) patients and their carers that, following a diagnosis of malignant mesothelioma, entitlement to some benefits and allowances is automatic. Applying for benefits requires attention to detail and can be time-consuming. Patients and carers should be advised to make photocopies of everything they send to benefits centres for their own reference. The clinical nurse specialist should assist in directing or referring the patient and carer to an organisation that can help with the completion of benefit applications. The lung cancer clinical nurse specialist will advise patients about what help is available locally and Macmillan Cancer Support (on freephone 0800 500 800) can also direct people to local benefits advisory organisations. National organisations offering a telephone benefits advice service, including help with completion of claim forms, are listed in Appendix 3 (available online at http://thorax.bmj.com/supplemental).
Coordinated care
The clinical nurse specialist facilitates the pathway of care for the patient and the family throughout the illness, ensuring good liaison between hospital services and primary care and access to specialist palliative care services as required. Patients should be made aware of whom to contact in case of need. The community nursing team (palliative care or district nurse) should be made aware of patients diagnosed with malignant mesothelioma within their area. A team approach should then be adopted to meet the nursing needs of the patient.
Nursing assessment
It is good practice to ensure that there is assessment of the needs of both the patient and the family or carers.136 Assessment of patients should include physical symptoms and physical functioning, psychological problems, social care needs and need for spiritual support. Assessment of family members and carers includes their concerns and need for support, including eventually bereavement support. Such assessment may need to be repeated at key times during the illness.
Patient advocacy
The limited treatment options, variation in expert opinion and universally poor outcome means that patient preference is particularly relevant when making treatment decisions about malignant mesothelioma. The relationship between the clinical nurse specialist and patient should help elicit patient and carer hopes and expectations and ensure that treatment plans are mutually agreed upon.
Accessibility
Timely access to the health care team is vital to ensure rapid attention to symptoms. The clinical nurse specialist is often best placed to provide a contact point and should be aware of any other points at which the patient may contact the service.
Support
Patients should be directed to an appropriate cancer support group such as the Lung Cancer Support Group. Where there is a sufficient number of patients with malignant mesothelioma, the development of a local Mesothelioma Support Group is recommended. Patients’ carers should be offered information about carer support when required.
Key points
The lung cancer clinical nurse specialist acts as the key worker facilitating the pathway of care for the patient and the family throughout the illness.
Clinical nurse specialists are pivotal to meeting patients’ specific supportive care needs.
Patients with malignant mesothelioma and their carers should have access to a lung cancer clinical nurse specialist.
The clinical nurse specialist should maintain complex communication pathways.
Providing information to people with cancer and carers should be an ongoing process.
The clinical nurse specialist should provide help and guidance to patients and their carers concerning entitlement to benefits and allowances.
Physical, psychological, social and spiritual assessment may need to be repeated at several key times during the illness.
Patient preference is particularly relevant when making treatment decisions about malignant mesothelioma.
Timely access to the health care team is vital.
Symptom control
All symptoms need a working diagnosis, as some may be caused by concurrent non-cancer related problems. It is often helpful to record symptom severity on a simple scale to assess progress and response to treatment. Relief of pain, breathlessness and other symptoms can occur with response to chemotherapy.
Pain
The treatment of pain in malignant mesothelioma follows the same principles as for any other cancer but can include more specific techniques where initial methods are inadequate. These may necessitate early referral to a specialist pain service. Specific techniques include:
Transcutaneous electrical nerve stimulation machines and acupuncture.
Intercostal, paravertebral or brachial plexus nerve blocks.
Interpleural,136 epidural or intrathecal analgesic infusions.
Local thoracic spine neurolytic blocks.
Percutaneous cervical cordotomy137 (particularly when the patient is still ambulant).
In pain from chest wall involvement the response to opioids is variable because of added inflammatory and neuropathic components. In this situation, the following adjuvant analgesics should be considered early: non-steroidal anti-inflammatory drugs (with gastric cover); steroids (with gastric cover); noradrenergic antidepressants such as amitriptyline; or anticonvulsants such as gabapentin or carbamazepine.
Pain control will be improved by attention to emotional, psychological, social and spiritual problems. Distraction and relaxation techniques and complementary therapies may also be helpful.
Pain associated with localised tumour invasion of the chest wall may respond to radiotherapy.99
Dyspnoea
The common causes of breathlessness in mesothelioma are pleural effusion, lung compression and chest wall stiffness. Weakness and malaise, and anxiety or panic will also contribute. Progressive breathlessness should be treated according to general palliative care guidelines62 that include pharmacological approaches such as opioids, benzodiazepines and oxygen, and non-pharmacological methods such as breathing exercises and relaxation combined with re-adaptation.138
Cough, anorexia, weight loss, fatigue, excessive sweating and depression all occur in malignant mesothelioma and should be managed according to palliative care guidelines.62
Key points
Early involvement of a pain relief specialist is indicated if pain is not controlled after initial measures.
Dyspnoea, cough and other symptoms should be managed according to palliative care guidelines.
PERITONEAL MESOTHELIOMA
The incidence of peritoneal disease, like pleural mesothelioma, has been steadily increasing over the last 30 years, but the ratio of pleural to peritoneal disease in an asbestos-exposed population remains high (in the order of 12:1) and is slowly increasing. Factors favouring the development of peritoneal disease appear to be longer, heavier exposure to asbestos and, perhaps, to mixed dust. Although the age distribution is similar to pleural disease, there is less male preponderance.
Pathology
The disease may be localised, multinodular or diffuse. Epithelioid subtypes are much more common with only about 15% of tumours being either mixed or sarcomatoid. In two-thirds of patients the disease remains confined to the abdomen. The undersurface of the diaphragm is almost always involved, but tumour rarely penetrates through into the thorax. Spread to the omentum, pelvis and right subhepatic space is common.
Well-differentiated papillary and cystic mesotheliomas seem to be a separate disease, distinct from malignant peritoneal tumours. These conditions are unrelated to asbestos exposure, usually occur in women and have a good prognosis.
Symptoms
These are non-specific and include abdominal pains, constipation, weight loss, abdominal distension, palpable masses and ascites. Small bowel obstruction is usually a feature of the terminal stages.
Imaging
The optimal imaging modality is probably CT scanning. This may show omental and mesenteric thickening (the commonest findings), sheet-like masses, tumour nodules and usually only minimal ascites which may be loculated. The differential diagnosis includes peritoneal secondaries from adenocarcinoma, peritoneal endometriosis and pseudomyxoma peritonei. Retroperitoneal nodal enlargement is more in favour of an adenocarcinoma.
Diagnosis
Cytological examination of the ascitic fluid rarely gives an answer but fine needle aspiration of omental masses has been advocated. If the diagnosis is suspected, this can be confirmed by laparoscopy.
Prognosis and treatment
The prognosis is worse than for pleural mesothelioma. In one study the mean survival time was 7.4 months compared with 11.4 months in a group with pleural mesothelioma.21 Like pleural mesotheliomas, the epithelioid subtype seems to be associated with a better prognosis, as is youth and a good performance status. There is limited evidence to support the benefit of chemotherapy, although responses are reported and small case series suggest prolonged survival with regimes based on cisplatin and including mitomycin C, doxorubicin and pemetrexed. The role of radiotherapy is unclear and is associated with considerable morbidity but might be considered prophylactically to laparoscopy port sites. It has been suggested that debulking procedures may improve the response to chemotherapy but there are no controlled trials.
It is important to remember that the management of peritoneal mesothelioma should also include multidisciplinary patient care and consideration of medicolegal aspects.
Key points
Peritoneal mesothelioma is related to asbestos exposure but is less common than pleural mesothelioma.
The outlook is poor and no treatment has been shown to alter prognosis.
BENEFITS AND COMPENSATION FOR MESOTHELIOMA
The respiratory specialist and clinical nurse specialist are often best placed to advise patients and families about opportunities for compensation. The legal test is that the diagnosis and causation should be established on the balance of probability. Hence, pathological diagnosis is not mandatory for compensation issues, although an unequivocal diagnosis will remove subsequent room for debate. Patients who cannot identify occupational exposure to asbestos are not eligible for compensation.
Patients may be entitled to claim compensation in two ways:
A claim for Industrial Injuries Disablement Benefit from the Department of Social Security (via the Benefits Agency) or through the War Pensions Scheme. Other benefits for incapacity and disability may also be payable.
A Common Law claim for damages from the firm/firms where exposure to asbestos occurred.
Industrial injuries disablement benefit (IIDB)
Industrial injuries benefit is awarded under the terms of the Social Security Contributions and Benefits Act 1992. This Act specifies that the following criteria must be met to qualify for industrial injuries benefit:
The person must be suffering from a prescribed disease or personal injury which developed after 4 July 1948.
(a) The claimant must have been an employee, ie, not self-employed and (b) they should have worked in a scheduled occupation, ie, one where there had been exposure to asbestos.
Mesothelioma is designated a Prescribed Disease (D3) under Schedule 1 of the Social Security (Industrial Injuries) (Prescribed Diseases) Regulations 1985. Under new regulations (The Social Security (Industrial Injuries) (Miscellaneous Amendment) Regulations 1997), the schedule of prescribed occupations was broadened to include any occupation in which there has been “exposure to asbestos, asbestos dust or any admixture of asbestos at a level above that commonly found in the environment at large”. Thus, work may not have involved the actual handling of asbestos but may have been carried out in its presence, sometimes known as para-occupational exposure.
Procedure for claiming benefit
A claim for IIDB is made by contacting the local Jobcentre Plus or by ringing the Department of Works and Pensions (DWP) enquiry line (0800 88 22 00) and asking to be sent form B1 100 PN(A). A supply of these forms should be available in chest clinics and the doctor or clinical nurse specialist should provide confirmation of the patient’s diagnosis in writing. Occasionally the claimant may need help with completion of the form. Leaflets SD5 (“Ill or Disabled because of Work”) and NI12 (“If you have an Industrial Disease”) may also be helpful.
In 2005 the Industrial Injuries Advisory Council reviewed the term of prescription for all asbestos-related diseases. They concluded that those for mesothelioma did not require any modification. However, they noted that the uptake of IIDB was less than the Council would have expected and therefore recommended various measures to raise awareness of the provisions of the scheme, one of which has been liaising with the British Lung Foundation to ensure that clinical nurse specialists are fully aware.
Another concern of the Council was the issue of prompt payments for terminally ill claimants, including all cases of malignant mesothelioma. The “90 day” rule for most benefits has already been waived, and measures have been put in place to reduce any administrative delays to a minimum. Providing the claimant qualifies, he or she should get 100% disability benefit backdated to the date of diagnosis/application. Currently, this is approximately £120 per week.
The Council also recognised that, although such claimants are assessed at 100% disablement, because of their poor life expectancy they receive only a fraction of the total amount payable compared with those suffering from less severe prescribed diseases. The Government has indicated that it intends to put in place a long-term solution to ensure that sufferers of malignant mesothelioma can receive compensation so that they themselves can benefit from it while knowing that their families are secure in the future. The Government is presently going out to consultation, and it is anticipated that they will be making some changes to the way in which mesothelioma sufferers are compensated during 2007.
War pensions scheme
Mesothelioma caused by asbestos exposure during service in the defence forces is compensated under the War Pensions Scheme. A claim should be registered with the War Pensions Agency; details of the local office should be in the telephone book or enquires can be made from the Veterans Agency help line (0800 169 22 77). Those in receipt of IIDB cannot also receive a War Pension, and vice versa.
Additional benefits payable for incapacity and disability
Patients should obtain Benefits Agency leaflet SD1 “Sick or Disabled” (available in tape, Braille and a number of languages). This gives full details of the various additional benefits for which they may be eligible:
Income replacement:
For those with adequate National Insurance contributions: Statutory Sick Pay (SSP) or Occupational Sick Pay from the employer for the first 6 months of illness or Short Term Lower Rate Incapacity Benefit where there is no employer to pay. After 6 months Incapacity Benefit (IB) is then payable.
For those with inadequate National Insurance contributions: Income Support (IS) for those whose income and capital is below specified limits and/or Severe Disablement Allowance (SDA) after 28 weeks of incapacity for work.
Help with excess costs of disability:
For those with an assessment for Industrial Injuries Disablement Benefit of 100%, Constant Attendance Allowance (CAA) is available.
For those not entitled to CAA, Disability Living Allowance (DLA) is available for those whose disability began before their 65th birthday and Attendance Allowance (AA) is available for those whose disability began on or after their 65th birthday.
The lung cancer clinical nurse specialist has a pivotal role in assisting patients with this process. Further, reassessment of benefit entitlement should be encouraged at regular intervals as further benefits may be applicable as the patient deteriorates or upon death.
Common law compensation
Clinicians seeing any case of asbestos-related lung disease should promptly advise the patient to consider seeking legal advice. This will reduce the risk of subsequent claims for malignant mesothelioma being “statute barred” (see below). Damages may be recovered from an employer by suing them. The claimant must show that, on the balance of probabilities, his or her injuries and/or disability are due to occupational exposure to asbestos, this exposure being attributable to the employer’s negligence in maintaining the standards required by common law. There may also be a breach of the employer’s statutory duty to comply with specific health and safety regulations. Claims can be made against a former employer’s insurer, even if the employer is no longer in business.
Proceedings for these claims must be started within 3 years of the claimant’s “date of knowledge” of any injury caused by asbestos exposure. A claim brought after the expiry of 3 years is generally “statute barred” and it may not be possible to pursue it in the courts. The “date of knowledge” is based on when the claimant first becomes aware:
that the injury is significant;
that the injury is attributable in whole or in part to the act/omission alleged to constitute the negligence or breach of duty; and
of the identity of the defendant.
The date of knowledge is not necessarily the first time a potential claimant is examined by a doctor. The courts have the discretion to extend the 3 year time limit, but the claimant will have to persuade the court to do so.
The Compensation Act 2006 ensures that sufferers can receive full compensation from any of their employers/insurers where asbestos exposure has occurred.
If a patient is awarded damages, the final sum is based on a combination of:
compensation for pain and suffering (and interest on that);
loss of earnings (and interest on that);
care costs;
other expenses (eg, modifying the home);
compensation for bereavement.
Compensaton under the Pneumoconiosis etc (Workers’ Compensation) Act 1979
For those in whom neither an employer nor an insurer can be identified, a claim can be made to the Department of Works and Pensions under the Pneumoconiosis etc (Workers’ Compensation) Act 1979. The purpose of this scheme is to provide lump sum payments to or in respect of certain persons who are, or were immediately before they died, disabled by pneumoconiosis, byssinosis or diffuse mesothelioma. Eligibility for an award depends on the following criteria being fulfilled:
Industrial Injuries Disablement Benefit (IIDB) is payable to the claimant in respect of the disease;
every relevant employer of his has ceased to carry on business; and
the claimant has not “brought any action, or uncompromised any claim, for damages in respect of the disablement”.
This last criterion means that, if the claimant has already begun a damages claim against the employer and has either settled that claim or that claim ended because the evidence against the employer was weak, then he will not be eligible for a payment under the scheme of this Act. The lump sum payable is derived from tables which are dependent upon age and the percentage disability of the IIDB, which should be 100% in the case of mesothelioma.
A summary of the compensation and benefits for mesothelioma is shown in fig 2. Appendices 2 (Staging systems) and 3 (Sources of information and help available for patients and carers, and advice on benefits and compensation) are available online at http://thorax.bmj.com/supplemental
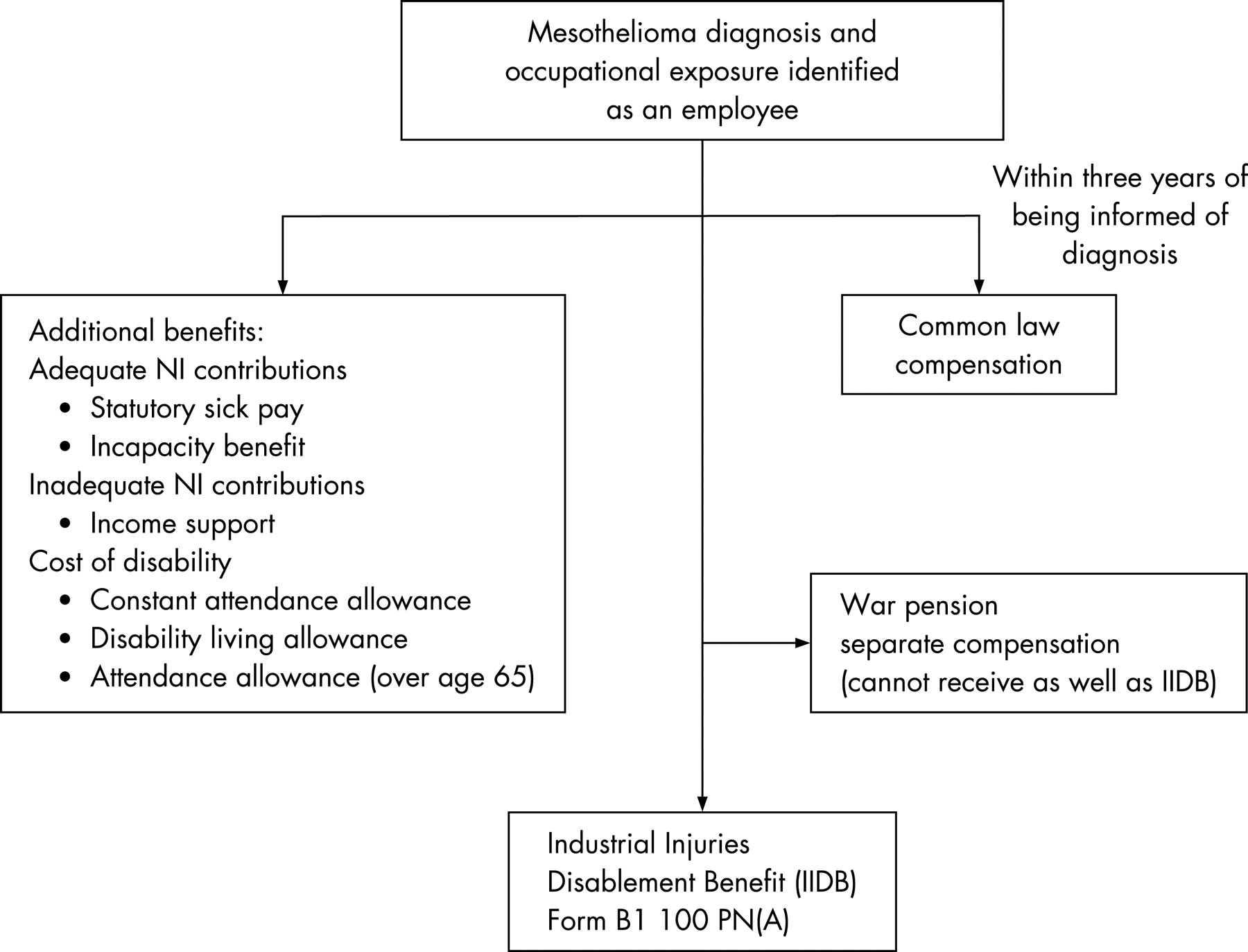
{kind=link}
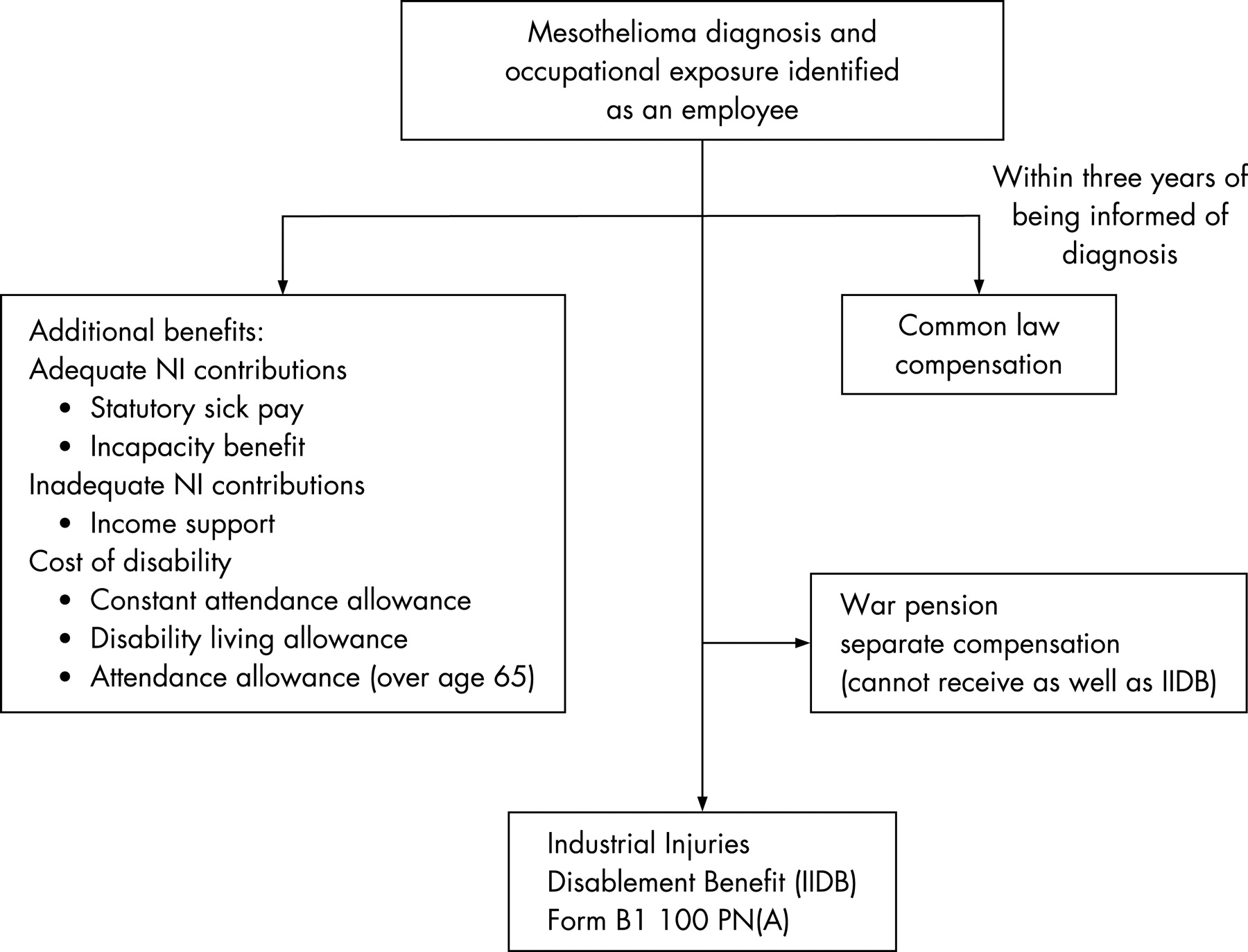{kind=link}
Appendix 1: Membership of the BTS Working Party
Professor M G Britton, Consultant Chest Physician, St Peter’s Hospital, Chertsey, Surrey; Ms L Darlison, Consultant Nurse, Glenfield Hospital, Leicester; Dr J Entwisle, Consultant Radiologist, Glenfield Hospital, Leicester; Dr M A Greenstone, Consultant Physician, Castle Hill Hospital, Cottingham, Hull; Dr M Hetzel, Consultant Physician, Bristol Royal Infirmary, Bristol; Dr C Higgs, Medical Director, Dorothy House Hospice, Winsley, Bradford-on-Avon, Wiltshire; Dr N Maskell, Consultant Physician, Bristol; Dr M F Muers, Consultant Physician, The General Infirmary, Leeds; Dr R Rudd, Consultant Physician, London Chest Hospital, London; Professor T Treasure, Consultant Thoracic Surgeon, Guys Hospital, London; Dr J Wiggins (Chairman and Editor of Statement), Consultant Physician, Wexham Park Hospital, Wexham, Slough, Berkshire.
Additional contributions were obtained from Dr A Darnton, Epidemiology and Medical Statistics Unit, Health and Safety Executive, Magdalen House, Stanley Precinct, Bootle; Dr M Snee, Consultant Medical Oncologist, Leeds; Dr M Sheaff, Consultant Histopathologist, St Bartholomew’s Hospital, London; Ms C Tan, Specialist Registrar, Guys Hospital, London; Dr D R Baldwin on behalf of the BTS Lung Cancer and Mesothelioma Specialist Advisory Group.
REFERENCES
Footnotes
- Abbreviations:
- CALGB
- Cancer and Leukaemia Group B
- CT
- computed tomography
- EORTC
- European Organisation for Research and Treatment of Cancer
- EPP
- extrapleural pneumonectomy
- FDG
- 18F-fluoro-deoxyglucose
- IIDB
- industrial injuries disablement benefit
- MARS
- Mesothelioma And Radical Surgery
- MRI
- magnetic resonance imaging
- PET
- positron emission tomography
- PS
- performance status
- RECIST
- Response Evaluation Criteria in Solid Tumours
- SMRP
- soluble mesothelin-related proteins
- SUV
- standardised uptake value
- VATS
- video-assisted thoracic surgery