





Countries that have already reduced their tuberculosis (TB) caseloads to low levels are now embarking on the road to reduce them even further and faster [1, 2]. In these countries, TB cases now predominate in subgroups of the population that are at greater risk of infection, progression to disease or unfavourable outcome, risks that oftentimes overlap within the same individual [3]. As low TB incidence countries approach the pre-elimination threshold, i.e. moving from <100 TB cases per million population per year today to <10 TB cases per million, it is expected that the concentration of disease in these subgroups will persist and possibly intensify as a result of the continued, natural attrition of the older population that accounts for many of the native TB cases today [4]. If the declining trend in TB incidence in these countries continues, TB will become rarer. The prospect of having fewer cases in the future does not automatically imply that the task of controlling TB becomes any lighter for national authorities. In fact, cases may become more difficult to find and to treat as a result of patient mobility, absent or incomplete healthcare coverage, lack of entitlements for those with irregular legal status, and other vulnerabilities linked to poverty, substance use, and co-existence of diseases such as HIV and diabetes, in a context of diminishing resources and expertise for TB case management. The development of resistance to anti-TB medication, which may be potentiated by some of these factors, compounds the picture even further. These epidemiological developments may put the progress towards TB elimination at risk.
The large majority of the TB cases occurring in most of the world and in low TB incidence settings remains drug susceptible and potentially curable with standard, first-line regimens, which have become widely available in recent decades. One of the threats to TB elimination has been the propagation of resistance, much of it fuelled by the improper use of the drugs making up these regimens. The emergence of combined resistance to rifampicin and isoniazid, the two most effective anti-TB medicines today (multidrug-resistant (MDR)-TB), has now become a matter of global concern [5]. While the bulk of the global MDR-TB burden occurs in large, populous, middle-income countries, richer countries with low TB incidence rates are not spared. International clusters of drug-resistant TB cases have involved, among others, western European countries and the USA [6, 7]. In many low TB incidence countries, TB patients of foreign origin are at higher risk of MDR-TB than native patients; in 18 European countries in 2012, for instance, the pooled odds ratio for MDR-TB in foreign-born versus native TB patients was 2.38 (95% CI 1.47–3.85) [8]. Persons born in the former Soviet Union have the highest risk of MDR-TB among TB patients in Western Europe [9].
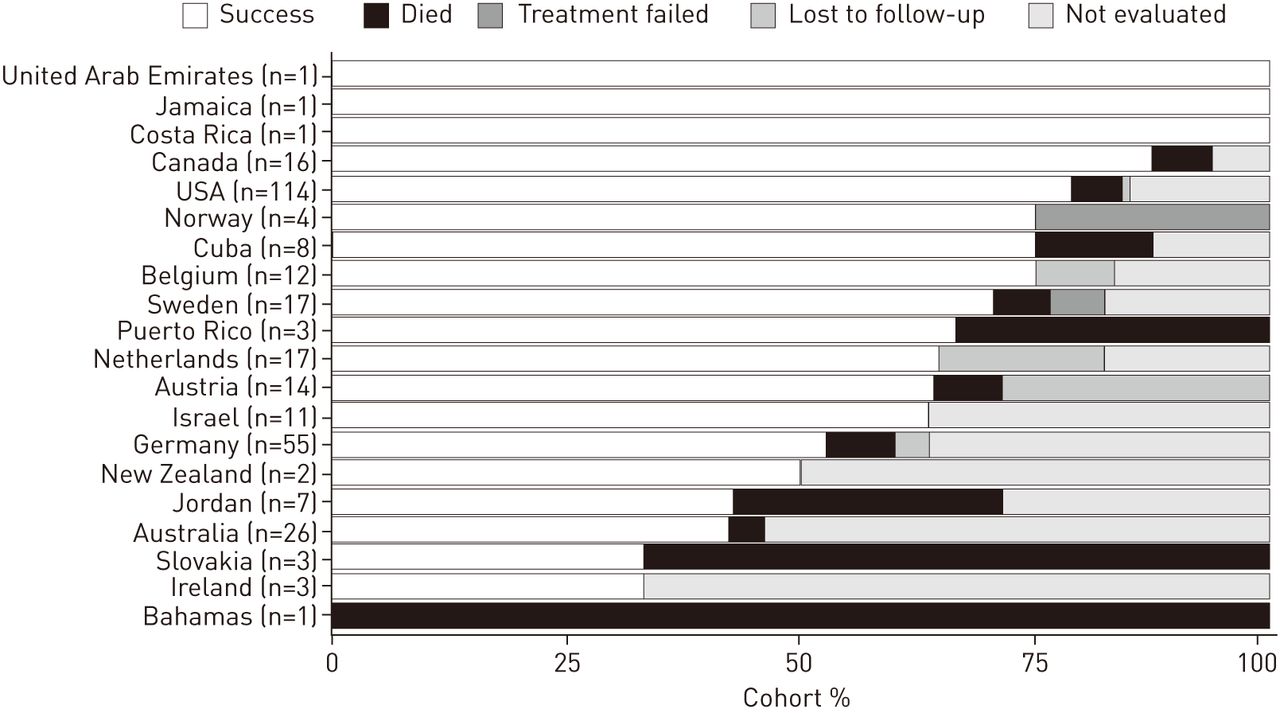
In May 2014, the World Health Assembly passed a landmark resolution endorsing a comprehensive strategy to address TB control in the world after 2015 [10]. One of the determinants of the future success of this strategy will be the manner in which drug resistance patterns will evolve in the world. The forms and speed with which drug-resistant strains will emerge will be closely linked to the practices of antimicrobial use [11]. Conditions that favour the spread of TB, such as poor infection control in congregate settings like hospitals and prisons, can likewise propagate drug-resistant strains even further. The impact on the future TB landscape can be posited. Firstly, immigrants are projected to come to represent a larger proportion of the total population in many high-income countries in the coming decades [12–14]. Many migrants originate from settings at higher risk of TB and drug-resistant TB than the host countries. If the proportion of migrants infected with drug-resistant TB strains who are settling in these countries increases with time, reactivated disease in these individuals is also bound to be more frequently drug-resistant in the coming years than it is today. Secondly, the reproductive fitness of MDR-TB strains (i.e. their capacity to cause disease) in the population could increase, a tendency which appears to be linked to the effectiveness of TB treatment programmes [15]. This would increase the risk of drug resistance among TB patients and, in an extreme-case scenario, highly virulent drug-resistant organisms may outpace the rate of replication of drug-susceptible strains. Thirdly, current treatment regimens for MDR-TB remain unsatisfactory in terms of safety, effectiveness, duration and cost [16]. Treating drug-resistant TB cases will impinge significantly on the national health budgets, particularly if new and expensive therapies become available [17, 18]. Even in several well resourced countries, the likelihood of a successful outcome is <60% [8] (fig. 1).
{kind=link}
Treatment outcomes for patients with multidrug-resistant tuberculosis starting treatment in 2011 in 20 low-incidence countries. Total number of cases in each cohort is shown for each country. Data from [19].
The roadmap for the elimination of TB in low-incidence countries needs to include a number of key elements targeting the prevention, early detection and care of drug resistance. Sustaining commitment and resources for TB control in the face of a dwindling epidemic will be a challenge and requires bold action. The resurgence of TB in the USA from the mid-1980s to the early 1990s, during which MDR-TB outbreaks featured prominently in certain localities, is a vivid reminder of the dangers of relaxing TB control [20]. Normality could only be regained following massive investments in public health and at the expense of much avoidable anxiety, disease and death [21]. The prospect of increased immigration should not trigger counter-productive and inhumane policies, especially towards those who cross borders illegally. Deportation of migrants with TB is likely to deter individuals from seeking adequate care when they need it, and thus fuel improper treatment and transmission within the community. Migration may well be an opportunity to help shore up some of the deficits in TB control in the world [22, 23]. A number of countries have already introduced policies that offer treatment of TB before entry into the host country or immediately after resettlement. Drug resistance needs to be considered in all TB patients, given that more than half of the global burden of MDR-TB occurs in cases with no previous history of TB and many of these may have no manifest risk factors for drug-resistance [24, 25]. Direct support by low-incidence countries for TB control efforts in the countries from where migrants originate, through technical assistance or financial grants, may be a viable option [26].
Unregulated use of second-line drugs and inadequate treatment regimens can generate more drug resistance, perpetuating a vicious cycle, the end-product of which will be patients infected with strains for which no treatment options are available [27]. About 9% of MDR-TB cases have extensively drug-resistant (XDR)-TB (MDR-TB plus resistance to any fluoroquinolone and any second-line injectable drug), a form of disease associated with very poor outcomes [28, 29]. By mid-2014, >100 countries and territories across the world had documented at least one XDR-TB case, including 22 of the 33 considered to have a low incidence of TB. The disruptive effect of single cases of MDR/XDR-TB on the healthcare resources of countries with small numbers of TB cases (such as Iceland and Malta) is a forewarning to other countries as they advance on their path to elimination. Moreover, cases with resistance beyond XDR-TB have been reported from different settings, including countries targeting elimination [30, 31]. Resistance patterns other than those that we know of today are destined to emerge as new anti-TB medicines are discovered and released on the market; the public health significance of new types of resistance may eclipse in importance that of the MDR/XDR-TB strains as treatment regimens evolve in the coming decades.
The new global TB strategy is projected to deliver fully on its promises only if new diagnostic, preventive and curative tools will start to be implemented on a large scale by about 2025 [10]. Until then, the path to elimination will require the optimisation of prevention and care of drug-resistant TB based upon time-proven approaches to TB control, using the currently available tools more effectively and engaging the collaboration of different actors towards this aim. The World Health Organization has just issued practical guidance on how to implement the programmatic management of drug-resistant TB based on the most recent evidence [32]. First of all, treatment of drug-susceptible disease needs to improve in order to reduce the risk of acquisition of resistance. The low cure rates observed in certain countries for a treatable condition are unacceptable. Secondly, if the control of drug-resistant TB is not to be achieved at the expense of the unnecessary death of many patients who could otherwise be cured, the affected patient will need a rapid diagnosis followed by appropriate treatment. Infection control depends to a large extent upon these patients being rendered noninfectious fast. The difficulties associated with drug-resistant TB treatment makes a patient-centred approach more important, including access to comprehensive social support. Financial enablers, provided alongside other adherence interventions [33], may become more cost-effective when TB control hinges upon a smaller number of cases required to complete their treatment. As TB starts to become rare, so will be the number of specialists and health services available to provide appropriate care. Measures to improve the awareness of healthcare professionals through continuous education, sensitisation about the realities of TB, networking between specialists, exchange of information and support in clinical decision-making for complicated cases could be effective [34, 35]. Thirdly, continued surveillance of resistance patterns and programme performance will be required and needs to adapt to a changing environment. Pharmacovigilance will be needed to promote the safer use of anti-TB medicines, and manage adverse drug reactions particularly when new drugs and novel regimens are introduced [36, 37]. Better use of available information technology to facilitate reporting is important. Fourthly, the uninterrupted availability of quality-assured drugs and proper antimicrobial stewardship to ensure their rational use (particularly measures to enhance regulatory structures and assistance in clinical decisions) will be required more than ever. And finally, the management of MDR-TB should be grounded on solid ethical principles, upholding the respect and promotion of human rights, and preventing the discrimination that patients suffer through the stigma attached to the disease. This is particularly relevant when infection control practices infringe upon the fundamental liberties of the patient.
If research is to make a difference to patients with drug-resistant TB, there needs to be a rapid translation of scientific findings into treatment and care practices in the coming years. The development of point-of-care rapid diagnostics for resistance will be crucial [38]. Safer, more affordable and more effective medicines in regimens that are shorter in duration and easier to administer are key to improving treatment outcomes. Repurposing of drugs that have anti-TB activity needs to continue. Studies of the chemoprophylaxis of drug-resistant TB will need to inform not only about its effectiveness in protecting the individual contact but also its potential role among the other population-level interventions available for the elimination of TB. And last but not least, evidence of which interventions can improve patient awareness and health-seeking behaviour in low-incidence settings will be needed to make programmes more effective in the face of drug-resistant TB.
Footnotes
D. Falzon and E. Jaramillo are staff members of the World Health Organization (WHO). The authors alone are responsible for the views expressed in this publication and they do not necessarily represent the decisions or policies of WHO. The designations used and the presentation of the material in this publication do not imply the expression of any opinion whatsoever on the part of WHO concerning the legal status of any country, territory, city or area, or of its authorities, nor concerning the delimitation of its frontiers or boundaries.
Conflict of interest: None declared
The content of this work is ©the authors or their employers. Design and branding are ©ERS 2014
- Received July 29, 2014.
- Accepted August 2, 2014.
- ©ERS 2014
References










