Article Text

Abstract
Background: Clinical studies suggest that inhaled corticosteroids reduce exacerbations and improve health status in chronic obstructive pulmonary disease (COPD). However, their effect on mortality is unknown.
Methods: A pooled analysis, based on intention to treat, of individual patient data from seven randomised trials (involving 5085 patients) was performed in which the effects of inhaled corticosteroids and placebo were compared over at least 12 months in patients with stable COPD. The end point was all-cause mortality.
Results: Overall, 4% of the participants died during a mean follow up period of 26 months. Inhaled corticosteroids reduced all-cause mortality by about 25% relative to placebo. Stratification by individual trials and adjustments for age, sex, baseline post-bronchodilator percentage predicted forced expiratory volume in 1 second, smoking status, and body mass index did not materially change the results (adjusted hazard ratio (HR) 0.73; 95% confidence interval (CI) 0.55 to 0.96). Although there was considerable overlap between subgroups in terms of effect sizes, the beneficial effect was especially noticeable in women (adjusted HR 0.46; 95% CI 0.24 to 0.91) and former smokers (adjusted HR 0.60; 95% CI 0.39 to 0.93).
Conclusions: Inhaled corticosteroids reduce all-cause mortality in COPD. Further studies are required to determine whether the survival benefits persist beyond 2–3 years.
- corticosteroids
- mortality
- chronic obstructive pulmonary disease
- pooled analysis
Statistics from Altmetric.com
Chronic obstructive pulmonary disease (COPD) is a major global epidemic affecting 5–15% of all adults in industrialised countries1,2 and accounting for over 3 million deaths each year worldwide.3 Even more alarmingly, the global burden of COPD will escalate over the next 20 years as more people live longer and a greater number of individuals take up smoking, especially in developing countries. By 2020 the World Health Organization predicts that COPD will be the fifth most prevalent disease (currently twelfth) and the third most common cause of death worldwide (currently fourth).3 Unfortunately, apart from smoking cessation, there is a dearth of management strategies available that can curb the rising impact of COPD.1 Smoking cessation improves the natural history of COPD. However, once COPD is established, many sustained quitters remain symptomatic and experience frequent exacerbations of their disease.1 They also have evidence for persistent airway wall inflammation.4 Thus, in symptomatic patients with COPD, additional treatments are indicated.
In view of the prominence and importance of airway inflammation in the pathogenesis of COPD,5 anti-inflammatory drugs such as inhaled corticosteroids can potentially improve health outcomes in patients with the disease. However, a few short term physiological studies have failed to demonstrate salutary effects of these medications on inflammatory indices in sputum,6,7 as one might expect given their anti-inflammatory properties, and several long term trials have failed unequivocally to demonstrate a beneficial effect in modifying the long term decline in lung function.8,9 Although several large clinical trials have evaluated the role of inhaled corticosteroids in COPD, none of them individually had sufficient statistical power to assess the effect of inhaled corticosteroids on all-cause mortality, and many did not report on mortality in their original publications. For this reason, prior meta-analyses, which relied on published grouped data, could not adequately evaluate mortality as an end point.8,9,10,11 To overcome this deficiency and determine whether inhaled corticosteroids affect all-cause and cause-specific mortality in COPD, we pooled retrospective individual patient data from the seven large randomised controlled trials evaluating the effects of these medications in stable COPD over a period of at least 1 year. Because some of these trials selectively chose patients with COPD who were actively smoking at the time of enrolment (leading to the over-representation of active smokers), we also evaluated the potential effect modification by smoking status and several other factors including sex, age, and baseline lung function.
METHODS
Studies included: design and treatment
The Inhaled Steroid Effects Evaluation in COPD (ISEEC) study included patient level data from all clinical trials in which patients with stable COPD were randomly assigned to inhaled corticosteroids or placebo for at least 12 months. These trials included the Lung Health Study-2 (LHS-2),12 Copenhagen City Lung Study (CCLS),13 Inhaled Steroids in Obstructive Lung Disease in Europe (ISOLDE),14 European Respiratory Society Study on Chronic Obstructive Pulmonary Disease (EUROSCOP),15 TRial of Inhaled STeroids ANd long acting β2 agonists (TRISTAN),16 and trials by Szafranski et al17 and Calverley et al.18 The full details of the individual trials have been published elsewhere.12–18
Participants in these trials were routinely seen at least every 3–6 months by study investigators. Mortality information was collected and collated by study personnel and recorded in the trial databases. Anonymised data collected from the seven individual trials were sent from each trial site to the central ISEEC coordinating centre where they were merged together for analytical purposes. We applied Hankinson’s prediction equation to calculate percentage predicted forced expiratory volume in 1 second (FEV1) across all studies.19 Principal causes of death were classified on reports by study investigators and were categorised into four groups: cardiovascular, respiratory, cancer, and others/unknown.
Statistical analysis
For the primary analysis we compared the efficacy of inhaled corticosteroids on all-cause mortality rates based on the original allocation of participants in the individual trials, regardless of whether they did or did not have complete follow up. This end point was chosen a priori. The participants in each trial were followed from the date of enrolment to the date of withdrawal (for whatever reason), death or study completion, whichever came first. In ISOLDE, complete mortality data were obtained on all study participants for 3 years through the UK Office of Population Statistics registry.20 In LHS-2, mortality status was established by the investigators for study participants over the duration of the trial. For the other studies, complete mortality data were obtained only on those who completed the trials. Deaths that occurred after the withdrawal date were not ascertained except among those who developed a serious adverse event during the trial period and died before the full resolution of the serious adverse event had occurred.
Kaplan-Meier curves were generated to compare the time to death between the steroid and placebo arms, and the log-rank statistic determined the significance of differences between the curves. Cox proportional hazards regression modeling was used to estimate the relative effect of inhaled corticosteroids on all-cause mortality according to confounding variables. Hazard ratios (HR) and the nominal 95% confidence intervals (CI) were presented. We checked for the proportional hazards assumption visually and by including a time-interaction term to the model and the assumption was met (p = 0.741). In the adjusted model we stratified by individual trials which allowed hazard functions to differ for each trial. The model also controlled for age (in quintiles), sex, baseline post-bronchodilator percentage predicted FEV1 (in quintiles), baseline smoking status, and body mass index (BMI; in quintiles) of the trial participants. Secondary analyses included subgroup analyses based on sex, baseline smoking status, and above and below median values for age, baseline FEV1, and BMI. Competing risk models were used to evaluate the hazards of cause-specific mortality. All tests were two tailed in nature and were conducted using SAS 8.2 software (Cary, NC). Continuous variables are shown as mean (SD) unless otherwise indicated.
RESULTS
The characteristics of the trials included in the ISEEC are summarised in table 1. In total, data from 5085 participants were analysed. None of the participants (including those who withdrew prematurely) was excluded from the analysis. The baseline characteristics of the trial participants are summarised in table 2. The mean (SD) age of the participants was 59.0 (9.3) years and the mean post-bronchodilator FEV1 was 58.4 (19.5)% of predicted. Nine percent of the cohort (N = 436) were in the Global Initiative for Chronic Obstructive Lung Disease (GOLD)1 class 4 (FEV1 <30% of predicted); 28% (N = 1419) were in GOLD class 3 (FEV1 30–49% of predicted); 49% (N = 2466) were in GOLD class 2 (FEV1 50–79% of predicted); and 15% (N = 764) were in GOLD class 1 (FEV1 ⩾80% of predicted). The mean bronchodilator response was 9 (12)% (0.13 (0.15) l) from pre-bronchodilator values. 71% of the participants were men and 69% were current smokers at the time of enrolment. In total, 973 participants (12%) withdrew prematurely from EUROSCOP, TRISTAN, and trials by Szafranski and Calverley and, as such, their vital status beyond the date of the study withdrawal could not be determined. In these trials, more participants withdrew prematurely from the placebo than from the steroid arm (21% in placebo versus 18% in the steroid arm; p = 0.006). The mean length of follow up was 26 (15) months; this was similar in the placebo and steroid arms of the trials.
Characteristics of individual studies at the time of randomisation
Baseline characteristics of study participants
Overall, 201 (4.0%) of the participants died during the trial period. Those who died during follow up were older (64 (7) years v 58 (9) years; p<0.001) and had lower post-bronchodilator FEV1 (48% (17)% v 59% (19)%; p<0.001) at the time of randomisation than those who survived to the end of the study period. Male participants were more likely to die than female participants (4.5% v 2.6%; p = 0.002). The baseline BMI was similar between those who did and did not die during follow up (25 (5) kg/m2v 25 (5) kg/m2; p = 0.794).
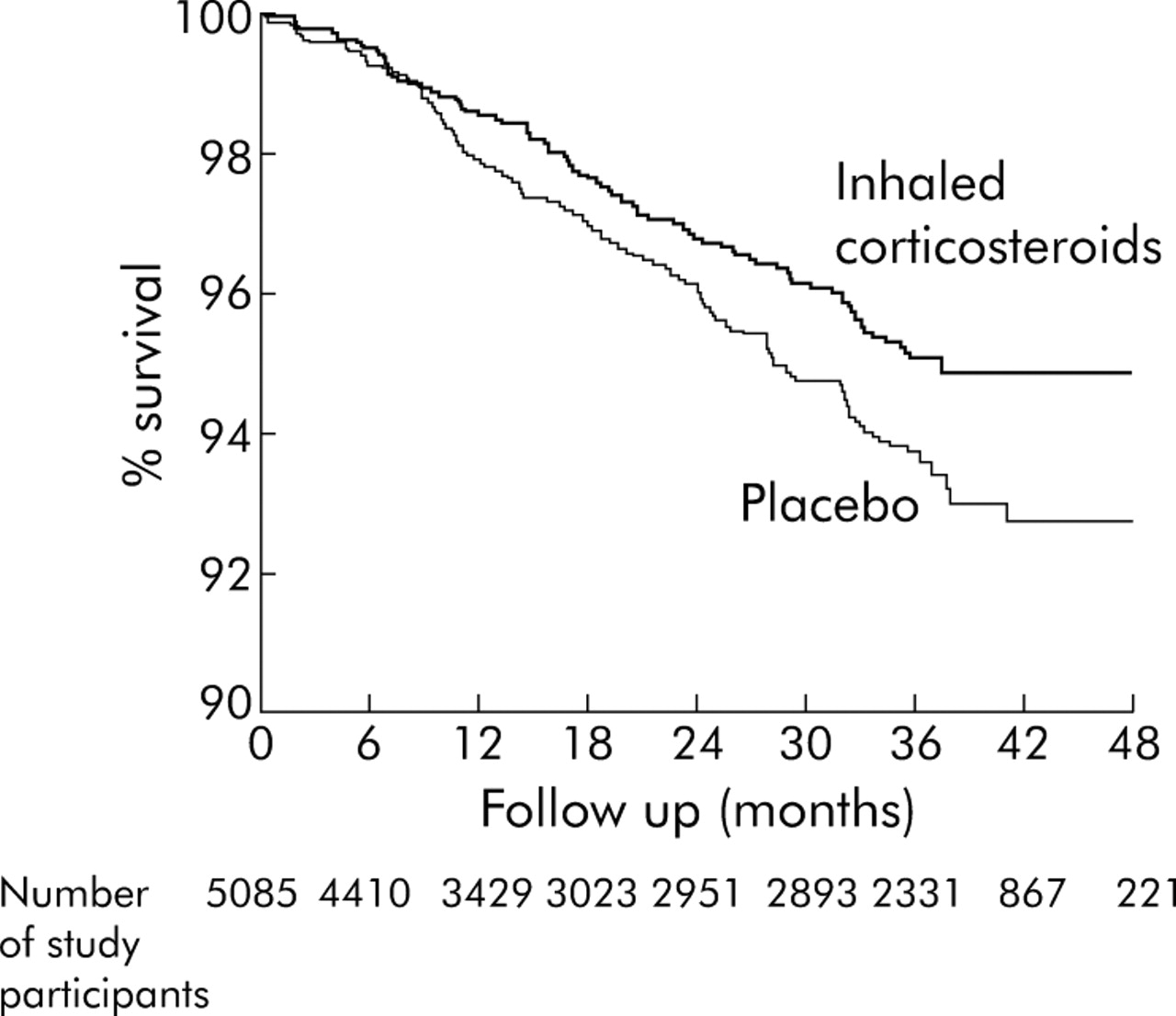
Compared with placebo, participants assigned to inhaled corticosteroids had a lower risk of mortality (HR 0.75; 95% CI 0.57 to 0.99; fig 1). Stratification by individual trials and adjustments for age, sex, baseline post-bronchodilator percentage predicted FEV1, baseline smoking status, and BMI did not materially change the results (adjusted HR 0.73; 95% CI 0.55 to 0.96).

Comparison of Kaplan-Meier survival curves between patients treated with inhaled corticosteroids and placebo in COPD (log rank p = 0.039).
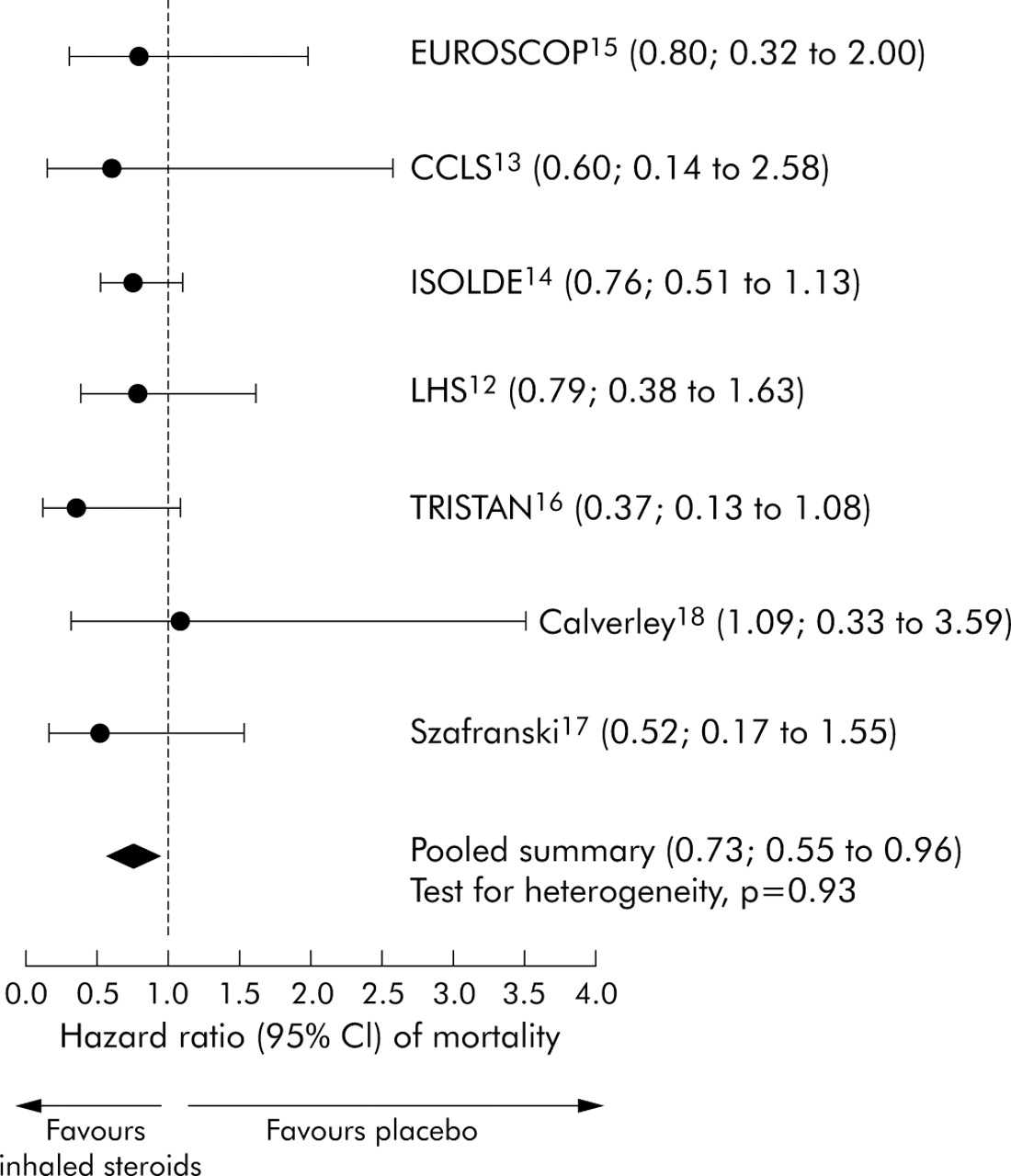
The effects of inhaled corticosteroids in the various subgroups are summarised in table 3. The beneficial effect of inhaled corticosteroids was especially noticeable in women (adjusted HR 0.46; 95% CI 0.24 to 0.91), former smokers (adjusted HR 0.60; 95% CI 0.39 to 0.93), and in those whose baseline post-bronchodilator FEV1 was below 60% of predicted (adjusted HR 0.67; 95% CI 0.48 to 0.94). We chose this FEV1 cut off because it was the median FEV1 value. None of the interaction terms was significant at the p<0.05 level. Subgroup analyses based on GOLD severity classes showed that, in participants in GOLD classes 3 and 4, inhaled corticosteroids reduced mortality (adjusted HR 0.66; 95% CI 0.45 to 0.96). The effect was non-significant among participants in GOLD class 1 (adjusted HR 0.84; 95% CI 0.19 to 3.65) and 2 (adjusted HR 0.79; 95% CI 0.51 to 1.23). The effects of inhaled corticosteroids were similar between fluticasone, budesonide and triamcinolone, although the width of the confidence intervals were different, reflecting the different sizes of the trials. We also performed subgroup analyses in which trials with a follow up time of 12 months or less were excluded. The results were similar whether trials were included or excluded in those with FEV1 <60% of predicted. In such patients, the exclusion of these three studies resulted in an HR of 0.67 (95% CI 0.47 to 0.95). There was no significant heterogeneity in the HRs across the trials (p value for test of heterogeneity 0.93; fig 2).
Comparison of inhaled corticosteroids and placebo for all-cause mortality per 100 patient-years in the various subgroups

{kind=link}
{kind=link}
Forest plot of hazard ratios for all-cause mortality across the individual trials. Data are presented as point estimates with 95% confidence intervals.
The principal causes of death are summarised in table 4, grouped into four major categories as described above. Most of the deaths were cardiorespiratory in nature (64% of all deaths). Approximately 21% of the deaths were from cancer. Of the 42 cases of carcinoma related deaths, 79% were attributed to lung cancer (N = 33). Other causes of death (including sudden deaths) and unknown causes accounted for the remaining 15% of deaths. Because of the small number of deaths in each category, none of the comparisons was significant at the p<0.05 level.
Comparison of clinical characteristics of patients who died from various causes of mortality and the effect of corticosteroids for these causes of mortality
DISCUSSION
The most important and novel finding of this study is that treatment with inhaled corticosteroids is associated with a 27% reduction in all-cause mortality in individuals with stable COPD. The beneficial effects of these medications appear to be especially pronounced in women (adjusted HR 0.46) and former smokers (adjusted HR 0.60). However, none of the interaction terms was significant so the survival data in the various subgroups should be interpreted cautiously.
This study has some limitations. Firstly, none of the primary studies included in the pooled analysis was designed to evaluate mortality as an end point, which imposed certain restrictions to the pooled analysis. For instance, five of the seven trials included in this pooled analysis did not ascertain mortality information on participants who withdrew prematurely from the trials. In these trials, participants were followed up to the date of withdrawal and any deaths occurring after this date were not recorded in the trial databases, except for those decedents who withdrew initially because of a serious adverse event from the study medication or placebo. As such, those who withdrew prematurely in these trials were recorded as “alive” at the final date of their assessment and any subsequent follow up period they were recorded as “missing.” Data from the ISOLDE trial indicate that the placebo group is more likely to withdraw prematurely than the steroid group (53% v 44%; p = 0.008), and mortality is much more likely in those who withdrew prematurely than in those who remain in the trial (p<0.001).20 It is therefore likely that, by not fully capturing deaths which occurred in the post-withdrawal period, we may have underestimated the true effect of inhaled corticosteroids because the rate of withdrawals was higher in the placebo arms than in the steroid arms of the trials and these participants tended to be sicker and to have a more rapid decline in FEV1.21 Indeed, in the trials in which complete mortality information was present (LHS-2, ISOLDE), inhaled corticosteroids were effective in reducing all-cause mortality in patients with COPD who had FEV1 <60% of predicted (adjusted HR 0.60; 95% CI 0.40 to 0.91). In contrast, in the other five trials in which complete mortality data were not available for participants who prematurely dropped out, the adjusted HR was 0.69 (95% CI 0.37 to 1.30).
Secondly, there was a lack of information on long term serious adverse events. The trials included in this analysis were too short to determine the long term effects of inhaled corticosteroids on such outcomes as hip fractures and glaucoma. In the short term at least, in the two trials that collected information on fractures (EUROSCOP and ISOLDE), inhaled corticosteroids did not appear to increase the risk of fractures (relative risk 0.70; 95% CI 0.36 to 1.38).11 Thus, to assess formally whether the benefits in the current pooled analysis outweigh the adverse effects, there needs to be long term clinical studies to define better the risk of important side effects related to inhaled steroid treatment. A third limitation was the difference in investigational medications between the trials. It was reassuring that we did not observe any significant differences between the different formulations, suggesting a class effect of these medications on mortality. Because the trials used relatively homogeneous dosing schedules for specific inhaled corticosteroids, we could not determine whether different doses produced differential outcomes in COPD patients. Finally, as with most pooled and meta-analyses, publication bias is a source of concern. To mitigate this possibility we included all studies that met the inclusion and exclusion criteria, even those with a relatively short follow up period (12 months). We found three such trials. Their inclusion was also important to model accurately the effects of inhaled corticosteroids on mortality during the first 12 months of treatment.
The current study cannot determine the potential mechanisms by which inhaled corticosteroids reduce all-cause mortality in COPD. However, since exacerbations increase both the acute and long term risk of mortality in COPD,22 these medications may confer survival advantage by reducing the frequency of moderate to severe exacerbations by nearly a third.10 The beneficial effects on exacerbations are most obvious in participants with spirometrically defined moderate to severe disease.23 It was in these participants (FEV1 <60% predicted) that the effect of treatment on mortality was seen, and not in those individuals with less impaired lung function where death was infrequent. In addition, these medications improve the health status of participants with moderate to severe disease.14 Reduced health status has been associated with both increased frequency of exacerbations24 and mortality.25 Inhaled corticosteroids also have a small effect on attenuating airway hyperresponsiveness,12 which is found in 60–80% of patients with mild to moderate COPD.26 Increased airway hyperresponsiveness has been linked to increased COPD mortality.27 Interestingly, airway hyperresponsiveness is more common in women than in men with COPD.26 The relative importance of these potential mechanisms requires further exploration.
This study was underpowered to evaluate the effects of inhaled corticosteroids on specific causes of mortality. However, there was a trend towards a lower risk of cancer related mortality for those randomised to inhaled corticosteroids. Whether or not this is a real effect will require further study. Chronic inflammation has been implicated in the development of malignant diseases.28 In particular, cycloxygenase (COX)-2 enzymatic activities may regulate immune responses that promote tumour growth.29 Inhaled corticosteroids over 6 months have been shown to reduce prostaglandin E2 levels, a product of COX-2 pathways, and to downregulate proto-oncogene (for example, BCL2) expression in the airways of smokers.30 In murine models, corticosteroids modulate proto-oncogene expression and inhibit tumour growth by as much as 70%.31 A prospectively randomised population of a similar size and follow up to this one will be needed to address these issues in patients with COPD.
Intriguingly, inhaled corticosteroids may be more effective in former than in current smokers. This pattern has also been observed in asthma.32,33 Acutely in COPD, smokers have a lower therapeutic response to oral corticosteroids than former smokers.34 It has been postulated that smoking induces a state of relative steroid resistance by increasing oxidative stress35 and by upregulating production of various pro-inflammatory cytokines including interleukin-6 (Il-6), IL-8, IL-1β, and monocyte chemoattractant protein-1.36 Additionally, cigarette smoke appears to reduce histone deacetylase activity and its expression in alveolar macrophages, making these cells relatively resistant to corticosteroids since one of the principal targets of corticosteroid action is by switching off gene expression of inflammatory genes through the recruitment of histone decetylases.37 Consistent with these findings, our data suggest that, for patients with COPD to experience maximal benefit from inhaled corticosteroids, cessation of smoking is of prime importance. Because the individual trials included in the current pooled analysis were originally designed and conducted at a time when anti-inflammatory drugs were thought to be most helpful in smokers with COPD, trials generally oversampled the smoking subpopulation of COPD patients. This may have attenuated (or even negated) the beneficial effects of inhaled corticosteroids observed in these studies.
In summary, the present pooled analysis indicates that inhaled corticosteroids are likely to be effective in reducing all-cause mortality in stable COPD. Further research is needed to understand better the molecular and physiological mechanisms by which inhaled corticosteroids reduce mortality in COPD.
Acknowledgments
The authors dedicate this paper to the fond memory of their loving friend and colleague, Professor Romain Pauwels.
REFERENCES
Footnotes
-
↵† Deceased.
-
Published Online First 14 October 2005
-
This work was funded in part by the Michael Smith/St Paul’s Hospital Foundation for Health Research and by a Canada Research Chair.
-
Competing interests: DDS has received honoraria for speaking engagements from AstraZeneca (AZ) and GlaxoSmithKline (GSK) and has received consultancy fees and research funding from GSK. JV has received honoraria for speaking engagements and research funding from AZ and GSK. JAA is currently an employee of GSK R&D, manufacturer of respiratory drugs. JBS was an employee of GSK. PMAC has received honoraria for speaking engagements and research funding from AZ and GSK. RP received honoraria for speaking engagements and research funding from AZ and GSK. NRA and ASB are members of a respiratory advisory board for GSK. BL is currently an employee of AZ, manufacturer of respiratory drugs. DSP has received honoraria for speaking engagements and research funding from AZ and GSK.
Linked Articles
- Airwaves