Article Text

Abstract
BACKGROUND A systematic quantitative review was conducted of the evidence relating parental smoking to spirometric indices in children.
METHODS An electronic search of the Embase and Medline databases was completed in April 1997 and identified 692 articles from which we included four studies in neonates, 42 cross-sectional studies in school aged children (22 were included in a meta-analysis), and six longitudinal studies of lung function development.
RESULTS In a pooled analyses of 21 surveys of school aged children the percentage reduction in forced expiratory volume in one second (FEV1) in children exposed to parental smoking compared with those not exposed was 1.4% (95% CI 1.0 to 1.9). Effects were greater on mid expiratory flow rates (5.0% reduction, 95% CI 3.3 to 6.6) and end expiratory flow rates (4.3% reduction, 95% CI 3.1 to 5.5). Adjustment for potential confounding variables had little effect on the estimates. A number of studies reported clear evidence of exposure response. Where exposure was explicitly identified it was usually maternal smoking. Two studies in neonates have reported effects of prenatal exposure to maternal smoking. Of five cross sectional studies that compared effects of perinatal exposure (retrospectively assessed) with current exposure to maternal smoking in later childhood, the three largest concluded that the major effect was in utero or neonatal exposure. Longitudinal studies suggest a small effect of current exposure on growth in lung function, but with some heterogeneity between studies.
CONCLUSIONS Maternal smoking is associated with small but statistically significant deficits in FEV1 and other spirometric indices in school aged children. This is almost certainly a causal relationship. Much of the effect may be due to maternal smoking during pregnancy.
Statistics from Altmetric.com
The first reports of an adverse effect of parental smoking on respiratory symptoms appeared in the early 1970s.1-3Since then, many epidemiological studies have reported on the association of parental smoking and respiratory diseases throughout childhood. The first report to examine lung function was largely negative4 but in 1986 the US Surgeon General reviewed 18 cross-sectional and longitudinal studies and concluded that “available data demonstrate that maternal smoking reduces lung function in young children”.5 The US Environmental Protection Agency Review6 and the recent Californian review,7 which were also essentially narrative, concluded that there was a causal relationship between exposure to environmental tobacco smoke (ETS) and reductions in airflow parameters of lung function. Other recent reviews, of evidence from studies in neonates and from cohorts, have concluded that there is compelling evidence that the effect is present at birth and attributable to effects of maternal smoking during pregnancy on fetal lung development.8 ,9
In this paper, part of a series of systematic and quantitative reviews of the effect of exposure to ETS in childhood, we summarise the evidence relating to the effects on ventilatory function. It follows on from our previous review of the effects of parental smoking on bronchial reactivity.10 Studies of peak flow variability and acute effects of exposure to tobacco smoke were reviewed in that paper and led us to conclude that parental smoking was associated with greater peak flow variability, possibly reflecting acute effects of daily variations in ETS exposure.
Our review therefore has the following structure. We first establish from all published cross sectional studies the magnitude of effect of parental smoking on the lung function of school children. We then consider possible biases and confounding and whether any susceptible subgroups can be identified. The evidence from cohort studies pertaining to lung growth is summarised. Finally we review evidence of effects of maternal smoking during pregnancy on neonatal lung function and the relative importance of prenatal and postnatal maternal smoking in surveys of school children. Throughout the review we focus on forced expiratory volume in one second (FEV1) because it is the most commonly reported index and also the one most strongly predictive of chronic non-specific lung disease in adults. However, we also consider mid and end expiratory flow rates.
Methods
REVIEW PROCESS
This paper is part of a series of reviews of the respiratory effects of ETS exposure in children. For this broader review, published papers, letters and review articles were selected by an electronic search of the Embase and Medline databases using the search strategy described elsewhere.11 Briefly, all passive smoking references were selected by the MESH heading Tobacco smoke pollution and/or text word combinations ({passive, second hand, involuntary, parent*, maternal, mother*, paternal, father* or household} and {smok*, tobacco* or cigarette*}) in the title, keywords or abstract. Papers were then restricted to children by selecting all papers classified as containing data on neonates or children under 18 and/or by relevant text words in the title or abstract. Embase searches were entirely based on text word searches. This search, completed in April 1997, yielded 3625 references of which 1593 contained keywords relevant to respiratory or allergic disease. These 1593 abstracts were reviewed and 692 were identified as of possible relevance to the assessment of respiratory health effects.
The 692 articles were reviewed and 112 were identified from their abstracts as potentially containing data relating ventilatory function and ETS exposure. These 112 papers related to rather fewer studies because of multiple publications. Seventeen studies were excluded for the following reasons: four foreign papers which may have contained data12-15; five studies which collected data but have not been published16-20; five studies that were not population based21-25; one study that provided data but the results appeared very extreme and were not internally consistent26; one study that only measured forced vital capacity (FVC) and presented no data27; and one study of 1400 children, in Spanish, which reported no effects in its abstract, but which we were unable to obtain.28
Table 1 summarises the characteristics of 20 cross sectional studies that provide some data, but insufficient to be included in the quantitative overview, and table 2 summarises the 22 studies included in the meta-analyses.
Cross-sectional studies. Data presented but not included in meta-analyses
Cross-sectional studies included in meta-analyses
Six longitudinal studies were identified which presented data on growth of lung function in school aged children in relation to parental smoking.30 ,42 ,58 ,70 ,71 The publication providing the longest length of follow up during childhood (usually the most recent) was used. The same studies were also included in the cross sectional analyses as appropriate.
Because of the interest in the possible role of prenatal exposure we also reviewed three studies which have looked at lung mechanics in neonates in relation to maternal smoking.72-79 A further study had too few exposed infants to allow any meaningful assessment of this issue,80 while the Tucson study of 125 children has not, so far as we are aware, published data on parental smoking and neonatal ventilatory function.81
OUTCOME MEASURES
Most of the studies in school age children have reported on flow measures of respiratory function. The outcomes reported nearly always include FEV1 and FVC, with rather fewer studies presenting data on mid or end expiratory flow rates (MEFR and EEFR).
STATISTICAL METHODS
For the purposes of quantitative analysis we needed to summarise the effect of ETS exposure on the same scale in different studies. We therefore transformed all reported effect measures to the difference in outcome measure (e.g. FEV1) between the exposed and non-exposed children expressed as a percentage of the level in the non-exposed group. We were able to do this in nearly all instances where effect measures were given, the exception being one study which reported differences in standard deviation scores with no baseline data.44 An approximate standard error (SE) for the percentage difference was calculated from which confidence limits were derived82; the approximation will be good because it depends on the SE of the variable being small in relation to its mean, which will be the case when dealing with means of lung function indices and their standard errors. We have used whatever measures were reported, assuming that a percentage difference in FEV0.75was equivalent to that in FEV1. Similarly, we have assumed that relative effects on FEF25–75 are similar to those on FEF50, and that reductions in FEF75 are equivalent to those for FEF85.
Quantitative meta-analysis was carried out by testing the percentage differences for heterogeneity using a χ2test.82 Pooled percentage differences were produced using both a fixed effects approach,82 in which a weighted average was taken using weights inversely proportional to the variance, and a “random effects” model83 since, in a number of instances, there was evidence of statistically significant heterogeneity of the passive smoking effect between studies. In practice, using a “random” as opposed to a “fixed effects” model made little difference to point estimates, but produced slightly wider confidence limits.
To assess whether there was evidence of publication bias and whether the studies included in the meta-analysis were typical, a funnel plot was used. For studies where only the direction of effect and p value were known we estimated the standard error by a regression of the standard error on the square root of sample size from studies where this was known. An estimated effect could then be calculated. Where only p>0.05 was given we plotted at one standard error. If no direction of effect was given we assumed it was zero.
Results
CROSS SECTIONAL STUDIES OF SCHOOL AGED CHILDREN
Of 42 population based studies (tables 1 and 2) which reported on the relationship between some measure of parental smoking and spirometric indices, 22 could be included in a formal meta-analysis, 21 of which reported on FEV1. Amongst these, FEV1was lower in exposed children in 18 of the 21 studies (fig 1). Overall, FEV1 was reduced by 1.4% in exposed children based on a random effects model. The difference was highly significant and unlikely to be due to chance. There was evidence of heterogeneity between studies, largely arising from four small studies reporting relatively large effects (three negative, one positive), while the largest studies reported rather smaller effects (fig 1). The random effects estimate, which gives greater weight to smaller studies, was thus slightly greater than the fixed effects estimate. Some heterogeneity is hardly surprising given the variety of exposure measures reported (tables 3 and4).
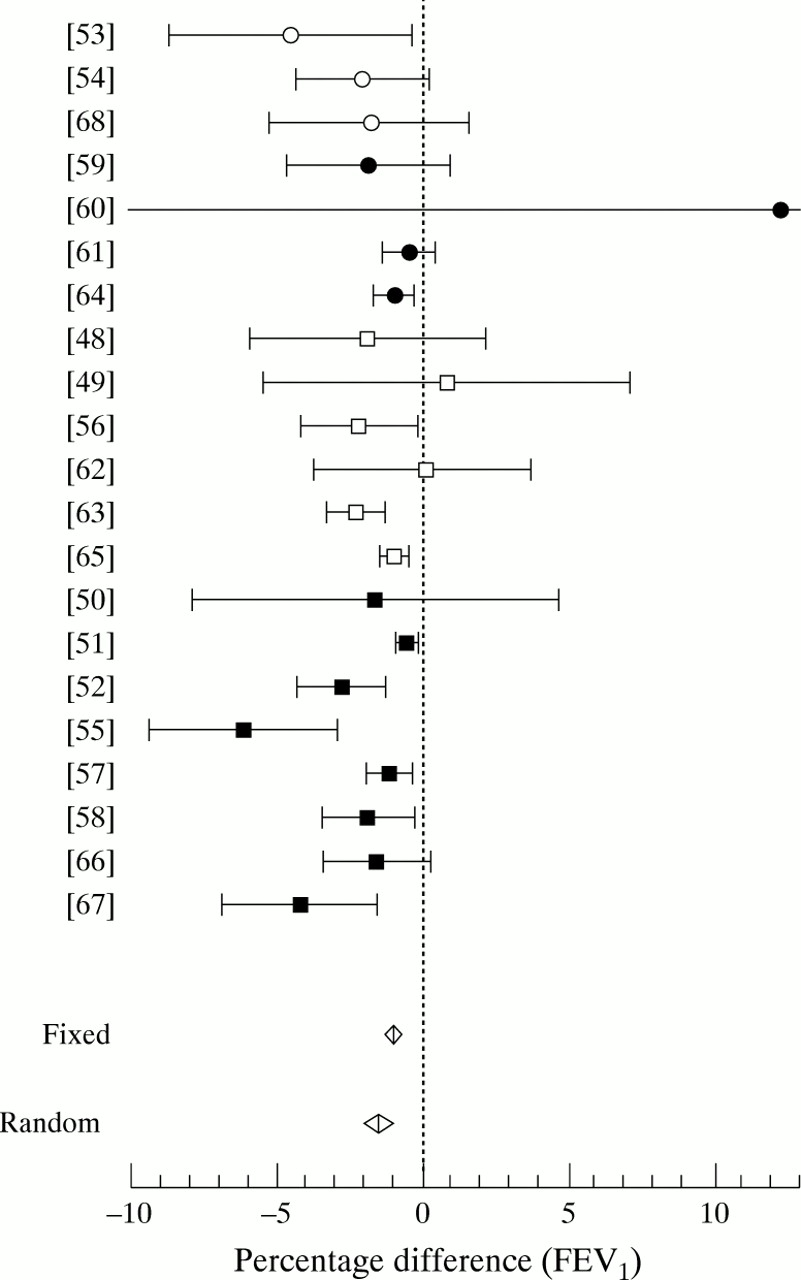
Percentage difference in FEV1 between children of smokers and non-smokers from cross sectional studies: open symbols are studies not adjusting for confounders other than age, height and sex; filled symbols are studies which adjusted for a variety of confounders. Squares = “low exposure” such as maternal smoking versus not or either parent smoking versus neither; circles = “high exposure” such as both parents smoking versus neither or top quintile of cotinine levels versus bottom.
Effects of ETS exposure on flow measures from cross sectional studies in school aged children: studies not included in meta-analysis
Effects of ETS exposure on flow measures from cross-sectional studies in school aged children: studies included in meta-analyses
Although there was no clear evidence of a greater effect in studies reporting on heavier exposures than in those reporting on lighter exposures (fig 1), most of the studies which tested for a graded relationship between level of exposure and lung function found some evidence for it, including two of the larger studies which reported clear evidence of exposure response.51 ,61 While a number of studies have reported a lower FEV1 in children where both parents smoke compared with those with only one parent or only the mother smoking, this could easily be due to greater smoking by the mother. Of 10 studies which allow comparison of the effects of maternal and paternal smoking,5 ,31 ,36 ,43 ,44 ,50 ,51 ,56 ,61 ,65nearly all report the effect of maternal smoking to be greater than that of paternal smoking (often reported to be zero), and none found a significant effect of smoking by the father only. The one study that has reported a clear effect of paternal smoking was carried out in Shanghai where women almost never smoke.52
There was no apparent difference between studies which had adjusted for factors other than age, sex and height and those that had not (fig 1). Primarily, this involved adjustment for social factors. There was no marked evidence of effect modification by age, either between studies or within studies.
For FVC the evidence for any effect of ETS was borderline, while the passive smoking effect on mid and end expiratory flow rates was rather larger than on FEV1 (table 5).
Summary of pooled percentage difference (95% confidence intervals) for effect of parental smoking on lung function from cross-sectional studies
Most studies that have commented on the effect in girls and boys separately have found a greater effect in boys, but the gender difference was rarely statistically significant. For the nine studies where we were able to extract data (fig 2), the pooled (fixed effect) estimate for boys was –2.1% (95% CI –2.8 to –1.5) and for girls was –1.3% (95% CI –2.0 to –0.6). There was no significant heterogeneity between the boy/girl differences across the individual studies (χ2 8 = 9.1, p = 0.33) and the overall gender difference was not significant at the 5% level (p = 0.06).
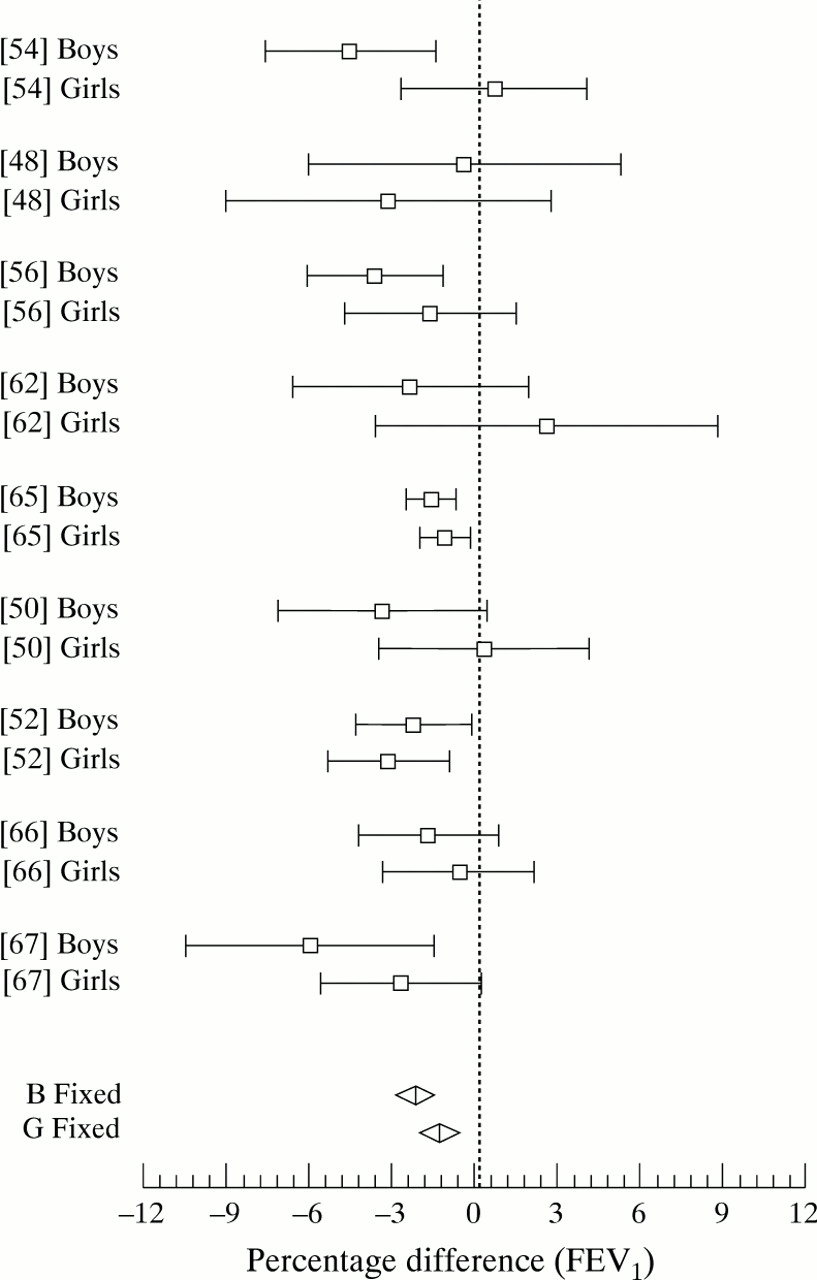
Percentage difference in FEV1 between exposed and non-exposed children, separately for boys and girls
While one study84 of 94 referrals to an allergy clinic has reported large effects of ETS on lung function (13% reduction in FEV1 and 23% reduction in MEF), population based studies suggest that any difference in effect between asthmatic and non-asthmatic subjects is rather small. Of two studies which allow a clear comparison of the relative magnitude of effects for FEV1 in these two subgroups, one61 suggests slightly greater effects in asthmatics (–0.4% in non-asthmatics versus –3.1% in asthmatics), while the East Boston study55 found effects greater in non-asthmatics (–6.1% in non-asthmatics versus –2.0% in asthmatics). Another study31 reported greater effects in asthmatics, but only for mid and end expiratory flow rates, while the Six Cities study found significant effects even when asthmatic subjects were excluded.65
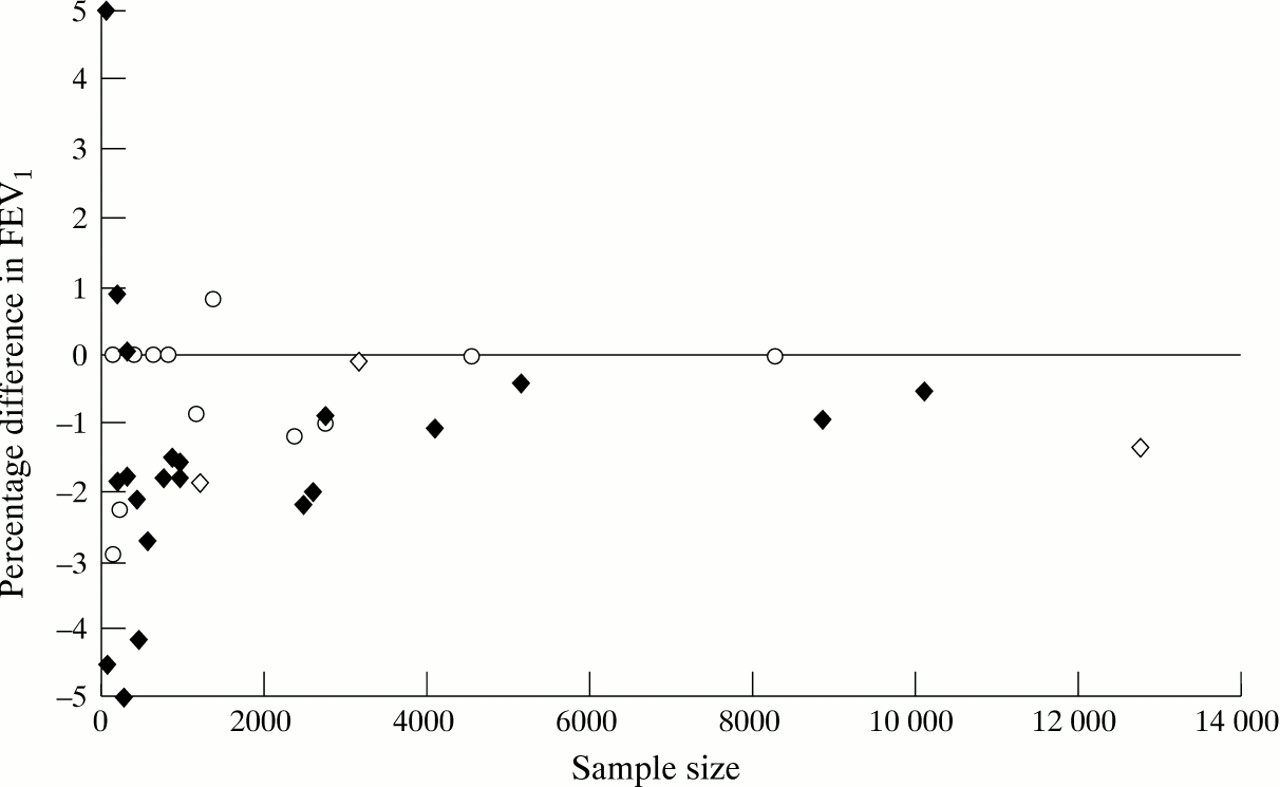
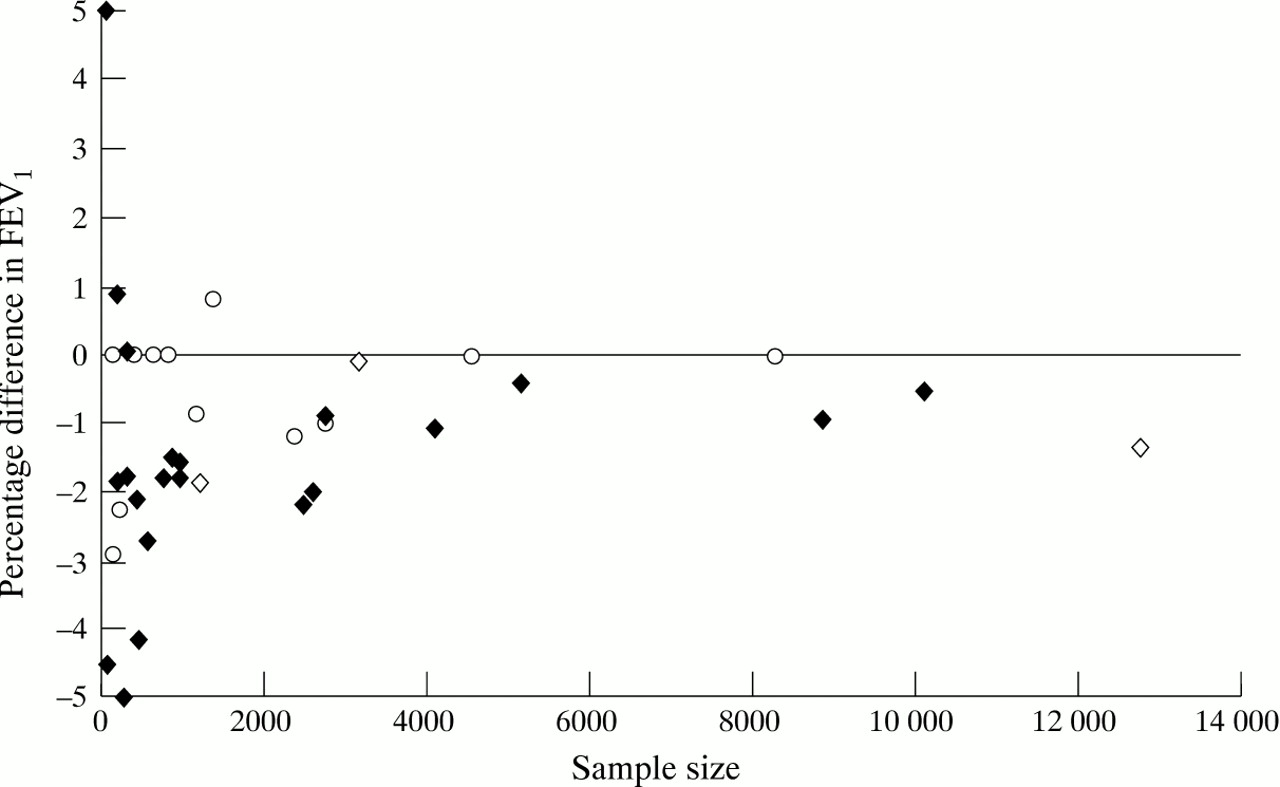
In order to investigate whether the studies included in the meta-analysis give a misleading impression, we examined the relationship between sample size and p values with direction of effect of ETS on FEV1 being indicated when known (fig 3). Studies included in the meta-analysis appear as filled symbols. There is evidence of publication/inclusion bias amongst the smaller studies with three studies reporting a greater than 4% deficit being included in the meta-analysis53 ,55 ,67 compared with only one very small study reporting a 12% increase.60 However, this inclusion/publication bias is not apparent in those with over 2000 subjects (fig 3). When we carried out separate meta-analyses of studies with under and over 2000 subjects, the random effects estimates for the percentage reduction in FEV1 were –2.3% (95% CI –3.2 to –1.5) and –1.0% (95% CI –1.6 to –0.4), respectively, suggesting that, while bias does exist, the influence on the overall random effects estimate (–1.4%, table 5) is small.
{kind=link}
{kind=link}
{kind=link}
Funnel plot for studies included (filled symbols) and not included (empty symbols) in meta-analysis. Where effect size is known it is plotted (lozenges), where unknown (empty circles) it was either assumed to be zero, or “guestimated” from known direction of effect, p value and sample size.
COHORT STUDIES
The principal design features and findings for the six cohort studies reporting on the effect of ETS exposure on lung function development are summarised in table 6.
Summary of principal design features and findings from cohort studies of effect of ETS exposure on lung function development
The East Boston study exhibited the largest cross sectional effect of any reported. In longitudinal analyses it was estimated that, over a five year period, the lungs of non-smoking children whose mothers smoked grew at only 93% of the rate of the lungs of non-smoking children whose mothers did not smoke.85 Taking a child of age 11 with no deficit in lung function, the deficit by age 16 would be 3%. Clearly these estimated effects are rather greater than the effects seen in most cross sectional studies (fig 1).
In contrast, the Tucson study exhibited no effects of ETS exposure on lung function cross sectionally, nor was there any influence on last recorded lung function in childhood nor any effect on growth in lung function.71 Recent re-analyses, based on follow up into early adulthood, have suggested some interaction effects including reduced growth in boys with initially low lung function who are exposed to ETS87 and possible interactions with active smoking.88 However, these interaction analyses lacked statistical power.
Because the East Boston and Tucson cohorts yielded different results, the two data sets were reanalysed using the Tucson89 and East Boston methodology.71 Both groups concluded that any differences were not due to statistical methodology, but the East Boston analysis suggests they could be due to chance, despite the fact that these two studies are at the extremes of the cross sectional results (table 3, fig 1).
The results of the Dunedin birth cohort42 are difficult to interpret since only statistically significant effects were included in models and a number of interaction effects were fitted. Boys and girls were analysed separately, and data only presented for FEV1/VC as “no significant changes in any pulmonary function measures were found in subjects who reported smoking during and/or after pregnancy”.
The US Six Cities study70 is the largest of the longitudinal studies by an order of magnitude as well as having 12 annual follow ups during childhood. The estimated effect of current maternal smoking on FEV1 growth is small but highly statistically significant, and is only one-tenth that of the East Boston study (table 6).
The Dutch study58 has the least power of all the longitudinal studies, both because of the limited number of subjects followed and the shortness of follow up (only two years). The confidence limits for the effects on FEV1 in boys and girls overlap with the Six Cities study.
Finally, a second Arizona study30 did appear to find reduced FEV1 growth in exposed children. However, this study also lacked power, no overall estimate of effect is available, nor are any standard errors.
STUDIES OF NEONATES
It has been suggested that the small deficits seen in flow rates for children of smoking mothers may be attributable, not to current ETS exposure, but to maternal smoking in utero. In order to investigate this and other hypotheses three studies have been carried out which measured various indices of respiratory function during infancy.
The East Boston neonatal study75-78 is a cohort study set up specifically to examine the influence of maternal smoking on infant respiratory function measured shortly after birth. Between March 1986 and October 1992, of 1000 women approached, 159 consented to respiratory function testing in their infant. Maternal smoking was documented during and after pregnancy with maternal reports being validated by maternal urinary cotinine levels. In 80 healthy infants tested shortly after birth (mean (SD) 4.2 (1.9) weeks), flow at functional residual capacity was markedly reduced (p = 0.0007) in infants born to smoking mothers (mean (SE) 74.3 (15.9) ml/s) compared with infants of mothers who did not smoke during pregnancy (150.4 (8.9 ml/s).75 These differences remained when flow was corrected for lung size. No differences in pulmonary function were evident in relation to postnatal exposure after stratifying by prenatal exposure. However, the power of these stratified analyses was severely limited. Subsequently, a study of 159 infants from the same study evaluated the effects of maternal smoking during pregnancy on growth in lung function during the first 18 months of life.78Maternal smoking during pregnancy was associated with reductions in functional residual capacity (mean (SE) –9.4 (4.3) ml, p = 0.03) and in flow at functional residual capacity (–33 (12) ml/s, p = 0.008). There was evidence that the effects were greater in girls than in boys. There was no evidence that growth of lung function was adversely affected. Moreover, the reductions in flow at functional residual capacity declined with increasing age from a 17% deficit at birth to 10% and 5% at 18 weeks and one year.
The Perth longitudinal study was based on random recruitment at the prenatal clinic at one hospital (26% participation rate).72-74 ETS exposure was assessed by questionnaire with validation by serum cotinine levels in half the cohort. Based on the 63 infants recruited in the first year of the study, there were no apparent or statistically significant reductions in maximal flow at FRC (measured at a mean of 4.5 weeks) if either parent smoked compared with both being non-smokers. In an analysis of 461 infants recruited subsequently,74 time to peak expiratory flow as a proportion of total expiratory time (measured 1–6.5 days postnatally) was found to be reduced in infants whose mother smoked >10 cigarettes per day compared with non-smokers. Infants whose mothers smoked 1–10 cigarettes per day were intermediate.
Finally, in a cross sectional study from Indiana79 112 healthy infants born at full term were recruited by advertisement in a university newsletter. FRC and maximal flow at FRC were measured at 1–31 months (mean 10.7 months) and ETS exposure was assessed by questionnaire at time of testing when 61 of the 112 were exposed. There were no overall effects of ETS exposure on maximal flow at FRC. However, while there were no effects in girls there was a deficit amongst exposed boys which was of borderline statistical significance (p = 0.07), with the difference in effect between boys and girls also being of borderline significance (p = 0.07).
EFFECTS OF PRENATAL AND POSTNATAL EXPOSURE IN CROSS SECTIONAL STUDIES
An analysis of data from the large US Six Cities study compared the effects of current maternal smoking with that during the first five years of life.70 The effects appeared to be independent and of similar magnitude. For FEV1 at ages 6–10 years the estimated effects were –0.4% (–0.9 to 0.1) for current smoking and –0.3% (–0.9 to 0.4) for smoking in the first five years. The authors concluded that, in school age children, the decrement in pulmonary function associated with maternal smoking appears to be due to a combination of a persistent deficit associated with earlier (including in utero) exposure and an additional deficit related to current exposure. A more recent paper based on 8863 non-smoking white children from 22 cities compared the effect of maternal smoking during pregnancy with maternal smoking in the previous year.65 Again the exposures were treated as dichotomous variables. In multiple regression analyses the effect of maternal smoking during pregnancy appeared to be larger than that for current smoking and not to be affected by adjustment for current smoking, while the effects of current smoking were small and not significant after adjustment for smoking during pregnancy. These analyses were supported by analyses of subjects who only smoked in pregnancy or only smoked currently. An effect of smoking during pregnancy independent of current smoking was also reported in a study of inner city children, but no data on current smoking effects were given.66
In contrast, one Dutch study of 965 children states that “adjustment for smoking in pregnancy (data not shown) slightly attenuated the associations between ETS and spirometry, but the coefficients for PEF and MEF remained of borderline significance.”58 The Dunedin study of 634 subjects also reported no effect of smoking in pregnancy.42
Discussion
In keeping with previous reviews5-7 we conclude that cross sectional studies show a consistent small deficit in lung function indices among children whose parents smoke. The proportionate reduction is smallest for FVC (–0.4%) and FEV1 (–1.4%), but larger for mid and end expiratory flow rates (–5.0% and –4.3%, respectively). A similar pattern is seen when looking within individual studies. Not surprisingly, given the variety of exposure measures used, there is some heterogeneity in effect between studies. While the effects seem to be real, they are hardly in themselves of clinical importance. The effects appear to be larger in boys, although the gender difference is not significant and there is the possibility that a degree of publication bias has occurred.
In large studies, which have investigated the amount smoked by mothers, there has been clear evidence of exposure response in relation to lung function. Only one study from China52 has shown an effect of smoking by the father only, which contrasts with the findings for respiratory symptoms and lower respiratory infections in infancy.11 ,90 Moreover, two of the largest and best American studies have reported no independent effect of paternal smoking.51 ,61 The greater effect if both parents smoke reported by a number of studies could well represent heavier smoking by the mother.
There is emerging evidence that neonatal lung mechanics are altered when mothers smoke during pregnancy. Both the East Boston and Perth studies made measurements sufficiently close to birth to effectively exclude effects due to postnatal ETS exposure. Such findings fit with a “programming” hypothesis—that is, the permanent alteration of the structure and function of organs by factors operating at critical periods of development in fetal or early postnatal life. Effects on lung function arising from in utero or neonatal exposure to cigarette smoke fit well with such a concept since the airways are fully present before the end of pregnancy, while alveolar proliferation continues to about four years after birth.9 However, the technical difficulty in measuring neonatal lung function implies that the magnitude of any effect of maternal smoking during pregnancy is imprecisely estimated. We do not know what the implications are for respiratory function in older children, nor whether these effects are permanent or reversible. Given the small size of the neonatal studies reviewed here, it seems unlikely that follow up of any of these cohorts will deliver a clear answer.
A blunter but more powerful way of assessing the long term effect of early life exposure is to identify children whose mothers smoked during pregnancy but who subsequently have stopped. Effectively this is the approach adopted by the 24 cities (only 22 out of 24 communities were included in this analysis)65 and the Six Cities studies.70 Both of these large studies suggest that maternal smoking during pregnancy or during the early years of life may result in small but persistent deficits in lung function. The Six Cities study suggests there may also be independent effects of current exposure. While these studies are of considerable interest, they are limited by the retrospective nature of their data collection and consequent imprecision in estimation of the effects of maternal smoking during pregnancy. However, taken together with the studies of in utero exposure and infant lung function, they suggest an important role for maternal smoking during pregnancy in causing the lung function deficits seen in cross sectional studies. Nevertheless, it would be premature to conclude that current exposure has no effect given the results from longitudinal studies suggesting small deficits in lung growth in relation to current exposure.
The Six Cities study is an order of magnitude larger than any of the other cohorts and has an annual follow up over 12 years as well as covering a broad geographical area. Its results must therefore be given substantial weight in any overall interpretation. The small but statistically significant effects of maternal smoking on lung growth (–3.8 ml/year for FEV1) are compatible with the inconsistent effects seen in most other cohorts where lack of power would explain many of the negative results. The exception is the East Boston study where the estimated effect of maternal smoking on FEV1 was 10 times greater at –27.8 ml/year. However, that estimated effect has extremely wide confidence limits.
None of the longitudinal studies have looked at change in lung function in relation to change in exposure. To determine if effects are reversible is perhaps the major advantage of cohort over cross sectional studies. Such studies require good estimates of exposure. So far no longitudinal studies of lung function in relation to cotinine levels have been published. Such studies would have the advantage that they would take account of changes in ETS exposure that occur as children spend less time with their parents as they grow older and thus their ETS exposure will fall even while parental smoking habits remain constant.
Conclusions
Children whose mothers smoke exhibit small but clear deficits in lung function, with the effects being larger for mid and end expiratory flow rates than for FEV1 and smaller still for FVC. The effects are not due to chance and do not appear to be due to publication bias or to residual confounding by other environmental factors. There is emerging evidence that in utero or early postnatal exposure plays an important role in explaining these deficits.
Convincing evidence for a role for current exposure would come from studies demonstrating change in lung function in relation to change in exposure. So far none of the longitudinal studies have examined this issue. A convincing demonstration of the effect of in utero exposure requires a large study with detailed prospective data on prenatal as well as subsequent exposure. It seems unlikely that the existing longitudinal studies of infant lung function will be large enough to achieve this.
It seems likely that the small differences in lung function in children associated with exposure to cigarette smoke will translate into small differences in adults given the tracking of lung function from an early age.91 However, such subtle reductions are unlikely to impact on the rates of development of chronic airflow obstruction unless evidence emerges that children exposed to cigarette smoke in early life have faster rates of lung function decline in adult life.
Acknowledgments
The Department of Health commissioned this review. The views expressed are those of the authors and are not necessarily those of the Department of Health. We are indebted to Jenny Taylor and Claire Chazot for their diligent work in assembling the relevant literature.