Article Text

Abstract
Background: Chronic obstructive pulmonary disease (COPD) is characterised by both an accelerated decline in lung function and periods of acute deterioration in symptoms termed exacerbations. The aim of this study was to investigate whether these are related.
Methods: Over 4 years, peak expiratory flow (PEF) and symptoms were measured at home daily by 109 patients with COPD (81 men; median (IQR) age 68.1 (63–74) years; arterial oxygen tension (Pao2) 9.00 (8.3–9.5) kPa, forced expiratory volume in 1 second (FEV1) 1.00 (0.7–1.3) l, forced vital capacity (FVC) 2.51 (1.9–3.0) l); of these, 32 (29 men) recorded daily FEV1. Exacerbations were identified from symptoms and the effect of frequent or infrequent exacerbations (> or < 2.92 per year) on lung function decline was examined using cross sectional, random effects models.
Results: The 109 patients experienced 757 exacerbations. Patients with frequent exacerbations had a significantly faster decline in FEV1 and peak expiratory flow (PEF) of –40.1 ml/year (n=16) and –2.9 l/min/year (n=46) than infrequent exacerbators in whom FEV1 changed by –32.1 ml/year (n=16) and PEF by –0.7 l/min/year (n=63). Frequent exacerbators also had a greater decline in FEV1 if allowance was made for smoking status. Patients with frequent exacerbations were more often admitted to hospital with longer length of stay. Frequent exacerbations were a consistent feature within a patient, with their number positively correlated (between years 1 and 2, 2 and 3, 3 and 4).
Conclusions: These results suggest that the frequency of exacerbations contributes to long term decline in lung function of patients with moderate to severe COPD.
- chronic obstructive pulmonary disease
- exacerbations
- lung function
Statistics from Altmetric.com
Chronic obstructive pulmonary disease (COPD) is in the top five leading causes of deaths in the world, and is associated with a significant health and economic burden through hospital admission and absenteeism from work.1,2 The accelerated decline in forced expiratory volume in 1 second (FEV1) with age has been related to the severity of airway inflammation.3
Exacerbations of COPD are an important cause of unscheduled physician visits and hospitalisation, and patients prone to frequent exacerbations have a reduced quality of life.4 We have recently shown that COPD exacerbations may increase airway inflammation5 and that a significant proportion may not show complete symptomatic or physiological resolution.6 Thus, it is possible that exacerbations by their incomplete recovery play a part in the decline in FEV1.
Previous studies of the relation of exacerbations and decline in lung function have been inconclusive. In 1976 Fletcher and colleagues7 concluded from their 10 year study that there was no relation between lung function decline and chest infections. However, their cohort had mild or no airflow obstruction, the diagnosis of exacerbation was retrospectively based on patient recollections, and the study possibly lacked the statistical power to identify any effect after adjustment for smoking, age, and body size. Kanner and colleagues8 reported in 1979 an association between decline in lung function and episodes of lower respiratory tract illnesses, although again the patients were relatively young and with mild airflow obstruction. More recently the Lung Health Study9 has reported that one lower respiratory tract illness per year, for which a physician was consulted, increased FEV1 decline by 7 ml/year in continuing smokers and intermittent smokers. A similar effect was not observed in sustained quitters and the average number of illnesses was only 0.24 per year. However, whether the decline in FEV1 is related to exacerbation frequency in patients with moderate to severe COPD is not known. Such information would be of importance as currently only smoking cessation is known to affect FEV1 decline in COPD.
In this study we have prospectively investigated a cohort of 109 patients with moderate to severe COPD over a 4 year period. Daily lung function and symptomatic data were collected to identify exacerbations and the relationship between decline in lung function and exacerbation frequency was then evaluated.
METHODS
Patients
Between November 1995 and November 1998, 161 patients with a diagnosis of COPD who attended outpatient clinics were recruited. Inclusion criteria were: FEV1 <70% predicted from age and height, β2 agonist reversibility <15% and/or 200 ml, and absence of asthma, bronchiectasis, bronchial carcinoma, or other significant respiratory disease.10,11 To investigate changes over time, the analysis was confined to 109 of these 161 patients who had recorded data on at least 365 days. The reasons for failing to record 365 days of data were withdrawal from the study, death, or inadequate completion of diary cards combined with late enrolment. These 109 patients did not differ significantly from the 52 excluded patients in any of the characteristics reported in table 1 except in peak expiratory flow (PEF).
Characteristics of the 109 study patients with COPD measured at recruitment and of the 32 who recorded FEV1
Baseline measurements were made of spirometric parameters and PEF by rolling seal spirometer (Sensor Medic Corporation, Yorba Lindo, CA, USA) when the patients were stable—that is, with no history of an exacerbation requiring treatment during the previous 4 weeks. Measurements were also taken of reversibility to 400 μg inhaled salbutamol and arterialised ear lobe blood gas tensions (model 278 Blood Gas Analyzer; Ciba-Corning, Medfield, MA, USA),12 and a history was taken of smoking, chronic symptoms, and long term inhaled and oral steroid use. The patients recorded on diary cards daily PEF (Mini-Wright, Clement Clark International Ltd, Harlow, UK) measured after medication around 10.00 hours, and increase over normal in symptoms of dyspnoea, amount and purulence of sputum, wheeze, sore throat, cough, or nasal congestion/discharge. Due to funding restrictions only 32 patients (29 men) in addition measured daily FEV1 at home using a spirometer (Micro Medical Ltd, Chatham, Kent, UK). They were similar to the other 77 patients in all characteristics listed in table 1, except they had a higher PEF (245 (IQR 180–300) v 174 (IQR 150–240) l/min, p=0.003 (Wilcoxon test)).
The study was approved by the ethics committee of the East London and City Health Authority and the patients provided written informed consent.
Exacerbation identification and treatment
Every 3 months patients were reviewed in the outpatients clinic and their diary cards collected. Exacerbations were diagnosed according to previously accepted criteria4–6,13 if the following symptom patterns were experienced for at least two consecutive days: either two or more of three major symptoms (increase in dyspnoea, sputum purulence or sputum volume) or any one major symptom together with any one of the flowing minor symptoms: increase in nasal discharge, wheeze, sore throat, cough or fever. Symptoms recorded continuously in the 5 day period before exacerbation onset were discounted when deciding whether an exacerbation had occurred or not. Some exacerbations where no diary card symptoms were recorded were identified by questioning the patient about their symptoms when at the clinic visits or on admission to hospital. Patients experiencing increased symptoms were encouraged to contact the clinical team and were generally seen before treatment within 48 hours. These exacerbations were classified as “reported exacerbations” with those unseen termed “unreported exacerbations”. During the study the number of hospital admissions and length of hospital stay for acute exacerbations of COPD were noted. Records of drug treatment, dosage, and course duration at these visits were kept from November 1996 and any treatment by primary care physicians was obtained where possible.
Exacerbation frequency
The annual exacerbation rate of each patient was calculated by dividing the number of exacerbations by the number of days they participated in the study, and multiplying by 365. As the study focused on decline in FEV1, we calculated the median exacerbation rate in the 32 patients recording FEV1 and divided all the patients into two groups—those experiencing less than the median rate of 2.92 exacerbations per year (“infrequent exacerbators”) and those with more than 2.92 per year (“frequent exacerbators”). Exacerbation rates for each 12 month period for all the patients who took part in the study were also calculated from the date of their enrolment and used to assess consistency in exacerbation frequency from year to year.
Statistical analysis
Data are presented as mean (SD) or median (interquartile range; IQR) values and comparisons were performed by unpaired t test, Wilcoxon matched paired sign rank test, or χ2 tests as appropriate.
Cross sectional random effects models were used to determine the effect of exacerbation frequency on decline in lung function,14 with lung function as the dependent variable and time (in years) as the independent variable. These models allow examination of the time variations independently of the cross sectional variations in panel data. The lung function data were logarithmically transformed as the work of Fletcher7 suggests a non-linear decline in lung function over time; the transformation also gave higher r2 values for the regression analysis, indicating that it provided a better model. We calculated the regression coefficients for infrequent and frequent exacerbators groups separately. The coefficients were then compared using their standard errors.15 We also tried the more conventional approach of testing the interaction between exacerbation frequency, as a binary variable, and time after allowance for their main effects. This showed frequent exacerbations as having a highly significant faster decline in FEV1 (p<0.001). We believe the simpler comparison of standard errors, although not optimal, is statistically more secure as the sample size in this study is relatively small. We also repeated the analysis but stratified the patients into four groups by exacerbation frequency and whether or not the patient currently smoked. The analysis was also repeated after stratifying the patients into two groups according to whether they had more or less than 1.5 reported exacerbations per year. This was the median rate for those exacerbations seen at clinic by the clinical team. The rationale for this was that the symptoms for these exacerbations were validated. Cross sectional, random effects models were also used to examine changes in binomial data on treatment with oral steroids and antibiotics over time assuming a logit relationship. The analysis was performed using Stata 5.0 (Stata Corporation) and the cross sectional models fitted using the Xtreg and Xtgee commands.
RESULTS
Patients
The 109 patients studied had moderate to severe COPD (table 1). Of these, 100 patients took inhaled steroids daily and 12 were on prednisolone taking a mean (SD) dose of 5.91 (3.0) mg /day; 10 patients used both oral and inhaled steroids. Data on exacerbation treatment collected over the last 3 years of the study showed that 124 of 561 exacerbations (22.1%) were treated with oral steroids and 341 of 561 (60.8%) with antibiotics. Table 2 shows how the probability of treatment changed per year in the frequent and infrequent exacerbator groups, and indicates that there was no significant change over time in the likelihood of treatment with either oral steroids or antibiotics. No significant change was seen if the groups were combined (data not shown).
Annual changes in treatment of exacerbations with oral steroids and antibiotics
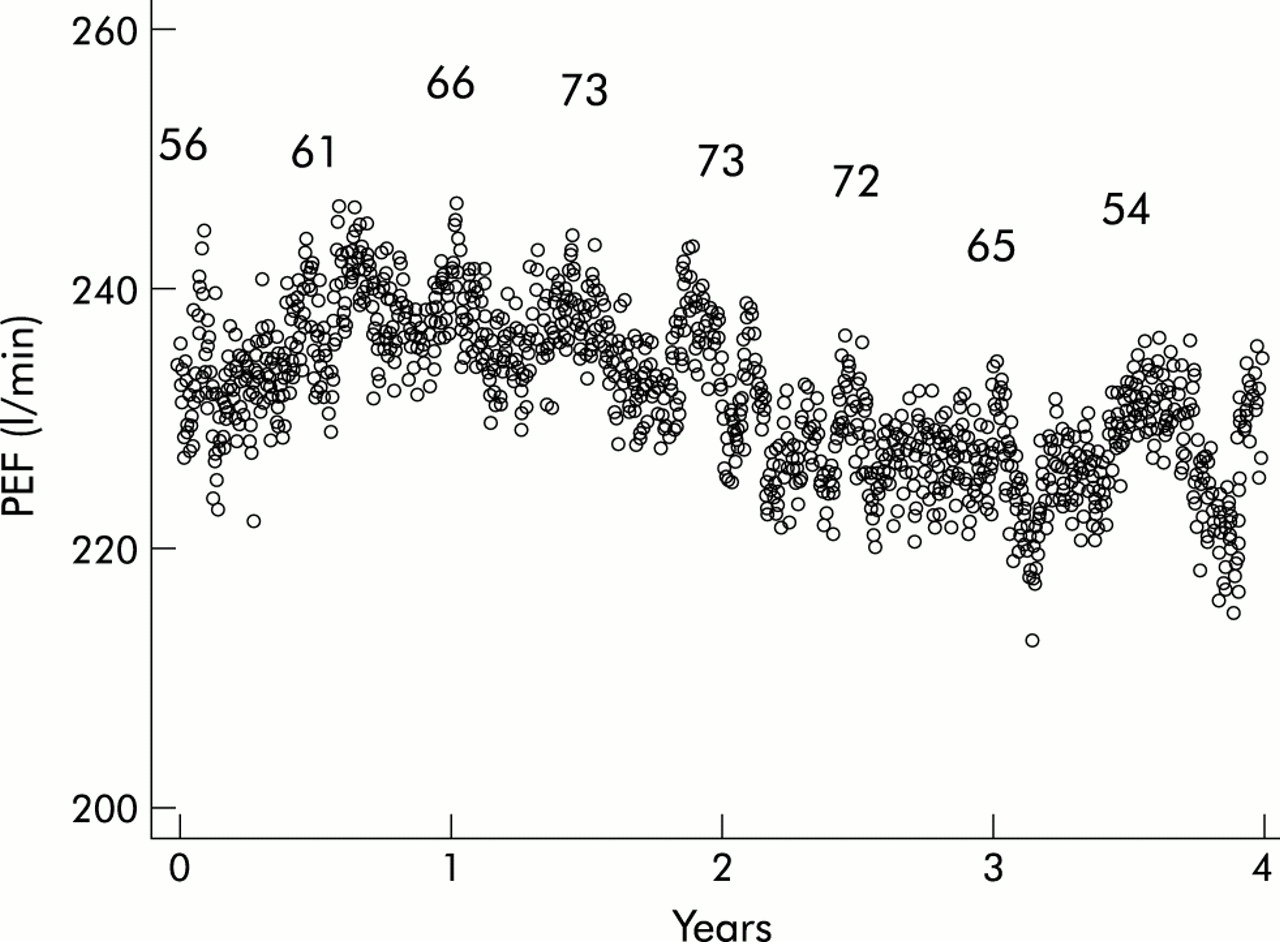
The patients participated in the study for a median of 958 days (range 405–1489) but diary card data were recorded on only a median of 801 days (range 366–1460) or 83% of this time (a total of 95 776 patient days). Figure 1 shows daily mean PEF over the 4 years of the study, although comparisons between days are not possible because patients withdrew and entered the study as it progressed. Non-compliance in recording data was due to diary card loss, non-completion while on holiday or in hospital, or when the patient felt too unwell. Eleven patients died and 20 withdrew before the end of the study.
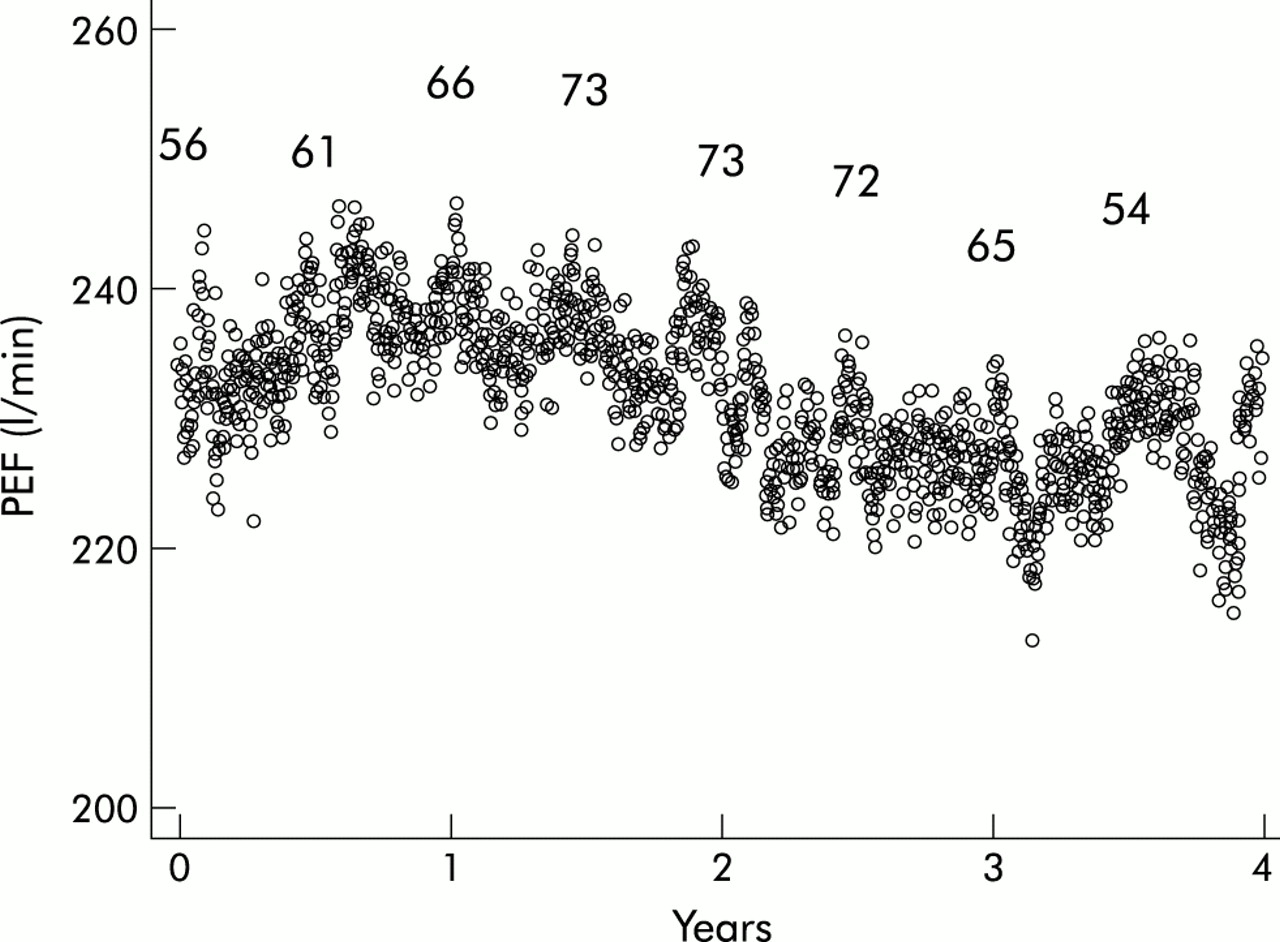
Mean morning PEF after treatment over 4 years. Numbers reflect the number of patients recording data on 1 November and 1 May each year.
Seven of the 63 infrequent exacerbators were admitted to hospital on a median of one occasion (IQR 1–1) for 10 days (IQR 4–12) while 20 of the 46 frequent exacerbators were admitted on a median of 1.5 occasions per year (IQR 1–3) for 10 days (IQR 7–14). Frequent exacerbators were therefore admitted more frequently (p=0.0001, Wilcoxon) and for longer (p=0.0032, Wilcoxon).
Exacerbations
One hundred of the 109 patients had one or more exacerbations, with a total of 757 of which 649 (85.7%) were identified from the symptom data recorded by the patients on their diary cards. A total of 380 (50.1%) exacerbations were reported and seen by the clinical team. There were no differences in daily symptoms recorded by the patient at exacerbation onset between those unreported and those reported to the clinic team (dyspnoea 61% and 62% respectively; sputum purulence 26% and 24%; sputum amount 44% and 39%; wheeze 33% and 31%; sore throat 13% and 11%; cough 23% and 28%) except in nasal congestion/discharge (22% and 34%; p<0.001, χ2 test). Including those patients who experienced no exacerbations over the study period, the median exacerbation rate was 2.53 (IQR 1.33–3.80) exacerbations per year, and for those patients recording FEV1 the median rate was 2.92 (IQR 1.94–4.23) per year; these rates were not significantly different (p=0.210, Wilcoxon). Of the patients who recorded FEV1, those classified as frequent exacerbators had a median rate of 4.2 (IQR 3.5–6.2) per year and infrequent exacerbators had a median rate of 1.9 (IQR 1.0–2.4) per year.
The number of exacerbations a patient experienced over the first year was highly and positively correlated with the number suffered during the following year (Spearman’s rho=0.53 , p<0.001, n=109). For those patients with data for more than 2 years the correlation between the annual rates for years 2 and 3 was rho=0.56, p<0.001, n=67 and, similarly, between years 3 and 4 was rho=0.35, p=0.044, n=33.
Lung function decline and its relationship to exacerbation frequency
Table 3 shows that the decline in FEV1 of 16 frequent exacerbators was at a significantly faster rate than in the 16 infrequent exacerbators (40.1 ml/year (95% CI 38 to 42) v 32.1 ml/year (95% CI 31 to 33), p<0.05). The difference between the two groups was therefore 8.0 ml/year (95% CI 2.6 to 13.5). Similarly, PEF showed a faster decline in 46 frequent exacerbators than in 63 patients with infrequent exacerbations (2.94 l/min/year (95% CI 2.8 to 3.1) v 0.72 l/min/year (95% CI 0.52 to 0.92), p<0.001). Figure 2 shows that the percentage decline in FEV1 of frequent exacerbators (4.22% per year) was greater than for those with infrequent exacerbations (3.59% per year). Similar results were found if the patients were stratified by their annual rate of reported exacerbations into two groups of <1.5 and >1.5 exacerbations per year. In the group with infrequent exacerbations FEV1 declined by 25.3 ml/year compared with 46.1 ml/year in those with frequent exacerbations (p<0.001).
Initial and annual change in lung function in patients with infrequent and frequent exacerbations

{kind=link}
{kind=link}
Percentage change in FEV1 with standard errors over 4 years. Open circles represent infrequent exacerbators; closed circles represent frequent exacerbators.
Table 4 shows there were no major differences in age, physical size, sex, lung function, blood gas tensions, and smoking habits between the infrequent and frequent exacerbators. There were also no differences in long term inhaled steroid use. However, chronic symptoms of dyspnoea and wheeze were significantly more likely in the frequent exacerbators. Similar comparisons limited to the 32 patients who recorded FEV1 showed, in addition to the chronic symptoms above, differences in age (frequent exacerbators were slightly younger than those with infrequent exacerbations (median 61.6 years (IQR 56.9–70.5) v 71.5 years (IQR 63.7–74.0); p=0.033, Wilcoxon)) and in the chronic symptom of cough (75% v 12.5% (p=0.001, χ2 test).
Comparison between patients who experience infrequent exacerbations (<2.92 per year) and those who experience frequent exacerbations (>2.92 per year)
In these 32 patients there were more current smokers among the frequent exacerbators (9 of 16) than among those with infrequent exacerbations (1 of 16). Analysis of the effect of smoking status at recruitment and exacerbation frequency on decline in FEV1 showed that frequent exacerbations contributed 21.5 ml/year (95% CI 20.2 to 22.7) to the decline in FEV1 independently of smoking which added a further 6.8 ml/year (95% CI 4.1 to 9.7); both effects were significant (p<0.001).
DISCUSSION
This study has shown for the first time that patients with moderate to severe COPD who suffered frequent exacerbations (>2.92 per year) experienced a significantly greater decline in FEV1 of 40 ml/year and in PEF of 2.9 l/min/year than patients who had infrequent exacerbations (<2.92 per year) in whom FEV1 declined by only 32 ml/year and PEF by 0.7 l/min/year. Similar differences in the decline in FEV1 were found whether or not the patient visited a physician at exacerbation. Frequent exacerbations were also associated with a faster decline in FEV1 if allowance was made for smoking status, although there was only a relatively small effect of smoking, possibly because there was only one smoker in the infrequent exacerbator group. A faster decline in the group with frequent exacerbations could be explained by less treatment of their exacerbations, but during the study we found no change over time in the probability of treatment of exacerbations with antibiotics or oral steroids in the frequent and infrequent exacerbation groups. Patients with frequent exacerbations had significantly more hospital admissions and spent a longer time in hospital. Other studies have recently shown that exacerbation frequency is an important independent risk factor for treatment failure and hospitalisation.16,17
The mean decline in FEV1 of 36 ml/year for all the patients is consistent with other recent studies of patients treated with long term inhaled steroids; 92% of our patients were treated with inhaled steroids. Renkema et al18 found a median decline of 30 ml/year with budesonide, but the ISOLDE study reported a 50 ml/year decline in FEV1 with fluticasone.19 Vestbo et al20 reported values of 30.0 ml/year and 45.5 ml/year respectively for male non-smokers and heavy smokers without mucus hypersecretion, which suggests a figure of around 35 ml/year in a patient group comprising 30% current smokers, although their subjects did not have a diagnosis of COPD and were about 10–15 years younger than the patients in our study.
The difference in the decline in FEV1 between the infrequent and frequent exacerbators was 8 ml/year, and their median exacerbation rates were 1.9 and 4.2 per year, respectively. In the Lung Health Study9 FEV1 in continuing smokers and intermittent quitters declined by 7 ml/year with each lower respiratory tract illness, with 0.15–0.25 illnesses reported per year. This suggests that exacerbations in moderate to severe COPD contribute a greater proportion to the decline in FEV1. In this study the difference of 8 ml/year between the two groups represents a 25% increase in decline due to the effect of frequent exacerbations.
Patients in this study were monitored on a daily basis over a 4 year period with exacerbations identified using previously accepted criteria of respiratory symptom increase.4–6 About half the exacerbations identified from the patients’ self-reported symptoms were confirmed by the study team at the clinic. We are therefore confident that few exacerbations were missed or misdiagnosed. The median exacerbation rate for the whole cohort of 2.53 per year was higher than that previously reported for patients with COPD of similar severity of lung function (1–2 per year18 and 0.99 per year19) This can be explained mainly by inclusion of about 50% of the exacerbations which were not seen in the clinic by the study team but which were diagnosed from diary cards. These unreported exacerbations would not have been included in the previous studies where definitions required a worsening of respiratory symptoms that involved physician intervention. However, we found no symptomatic differences between reported and unreported exacerbations except that the incidence of nasal congestion was higher with reported exacerbations.
There are a number of mechanisms that might explain the association between frequent exacerbations and decline in lung function, but it is also possible that a common mechanism leads to both. The decline may be mediated by airway inflammation which would be further increased by COPD exacerbations,5 especially if triggered by viral or bacterial infections.21 The presence of bacteria in the airways has been associated with increased airway neutrophilia and inflammatory markers,22,23 and persistent bacterial colonisation of airways is related to the severity of the underlying airflow obstruction.24–26 We have recently found that patients with frequent exacerbation are more likely to have increased bacterial colonisation.27 We have also shown that patients with frequent exacerbations have higher levels of the cytokines interleukin (IL)-6 and IL-8 in induced sputum, which suggests that frequent COPD exacerbations are associated with increased airway inflammation.5 The increased airway inflammation in patients with frequent exacerbations may therefore lead to the accelerated decline in FEV1 seen in this study.
We have shown that the annual exacerbation rate remains fairly consistent within a patient from one year to the next. The consistency is important in contributing to the accelerated decline in FEV1 associated with frequent exacerbations. We have previously shown that exacerbation frequency is strongly related to health status4 and to airway inflammatory markers. This finding confirms the basis for categorising patients into frequent and infrequent exacerbation groups, and emphasises the importance of targeting treatment at those with frequent exacerbations.
This study has shown that exacerbation frequency is an important determinant of decline in lung function in COPD. Strategies for prevention or ameliorating COPD exacerbations may have an important impact on the health burden of this common disease and thus improve the morbidity and mortality.
Acknowledgments
We would like to thank Dr Mark Roland for assistance with data collection and to express our gratitude to the British Lung Foundation for support for this study and to GlaxoSmithKline for financial assistance with the analysis of part of the data.
REFERENCES
Footnotes
-
Funding: The British Lung Foundation
Linked Articles
- Correction