Article Text

Abstract
Consistent with the diversity of Latin America, there is profound variability in asthma burden among and within countries in this region. Regional variation in asthma prevalence is likely multifactorial and due to genetics, perinatal exposures, diet, obesity, tobacco use, indoor and outdoor pollutants, psychosocial stress and microbial or parasitic infections. Similarly, non-uniform progress in asthma management leads to regional variability in disease morbidity. Future studies of distinct asthma phenotypes should follow-up well-characterised Latin American subgroups and examine risk factors that are unique or common in Latin America (eg, stress and violence, parasitic infections and use of biomass fuels for cooking). Because most Latin American countries share the same barriers to asthma management, concerted and multifaceted public health and research efforts are needed, including approaches to curtail tobacco use, campaigns to improve asthma treatment, broadening access to care and clinical trials of non-pharmacological interventions (eg, replacing biomass fuels with gas or electric stoves).
- Asthma
- Asthma Epidemiology
- Asthma Genetics
- Paediatric asthma
Statistics from Altmetric.com
Introduction
According to the WHO, ∼235 million people worldwide have asthma,1 with the number likely to be higher due to underdiagnosis. The International Study of Asthma and Allergies in Childhood (ISAAC) and other studies have shown a marked increase in the prevalence of asthma worldwide over the last few decades. Whereas there has been a recent plateau in this trend in industrialised nations, a rising trend continues in many non-industrialised countries.2 ,3
In the USA, the prevalence of current asthma is ∼8% in adults and 9.3% in children.4 In contrast, over half of Latin American countries report a prevalence of childhood asthma >15%.5 Moreover, most deaths from asthma occur in low-income and middle-income countries such as those in Latin America.
We provide an update on literature on asthma in Latin America published since a previous review 6 years ago,6 or not covered in a more recent review that excluded data from Brazil and certain topics such as perinatal and allergen exposures.7 Increased understanding of asthma in this region should lead to better prevention, diagnosis and treatment of this disease in Latin Americans.
Search strategy
We searched PubMed and SciELO for articles containing the terms “asthma”, “wheeze”, or “airway hyperreactivity” and either “Latin America” or the name of any Latin American country. We selected the most relevant articles from the last five years, with exceptions made for topics with few research articles. We used original complete texts in English, Spanish or Portuguese when available, or abstracts otherwise.
Asthma prevalence, morbidity and mortality
Latin America is a geographically, politically and economically diverse region comprising 20 countries whose languages are primarily Spanish and Portuguese (table 1). It covers ∼13% of the earth's land surface area, and stretches from Mexico, through the Caribbean and Central America, to Argentina. Including Puerto Rico (a US territory with Hispanic roots), Latin America has ∼600 million people. If all countries within the Americas where a Romance language is predominantly spoken (eg, French or Creole) were included, this population would approach 603 million people.
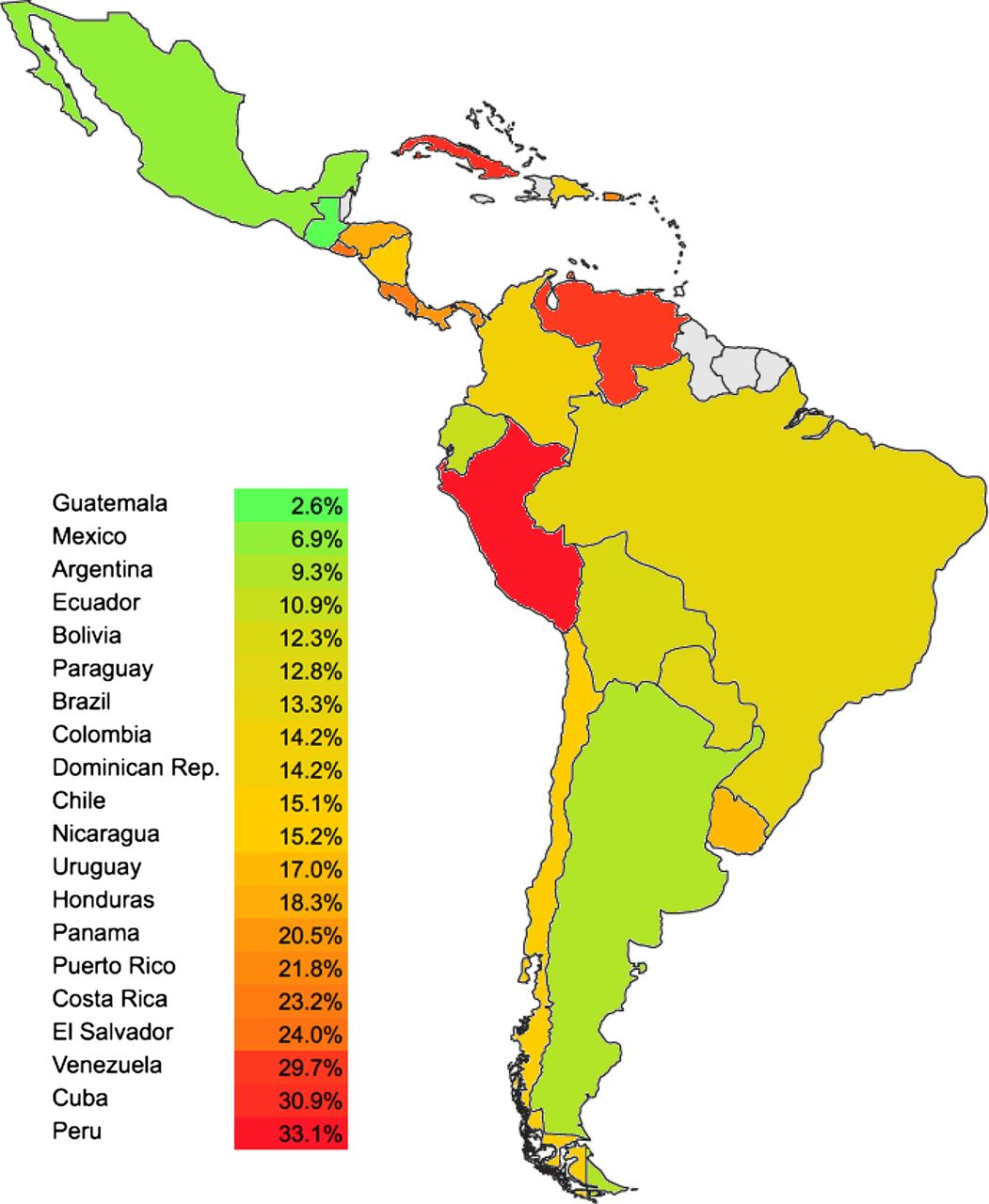
ISAAC provided the first estimates of the prevalence of asthma or asthma symptoms in the region using standardised questionnaires. The prevalence of physician-diagnosed asthma in ISAAC and other studies varies widely among Latin American countries (table 1). In children ages 13–14 years, phase III of ISAAC showed that the prevalence of ‘current wheeze’ ranged from 8.7% in Mexico to 30.8% in El Salvador, and that of ‘ever asthma’ ranged from 6.9% in Mexico to 33.1% in Peru (figure 1).5 Asthma burden also varied within countries: among 17 centres in Brazil, the prevalence of ‘ever asthma’ ranged from 7.3% (Nova Iguaçu) to 21.2% (Porto Alegre). As expected in a region with limited resources, there may be significant underdiagnosis. A study in Havana, Cuba, reported that up to ∼9% of children younger than 15 years may have undiagnosed asthma.10

Few studies have reported asthma prevalence among Latin American adults. Whereas a nationwide Colombian study estimated that 6.3%11 of adults have physician-diagnosed asthma, a Mexican study estimated that 5% of adults have physician-diagnosed asthma.12
Morbidity and mortality from asthma also vary among and within Latin American countries (table 1). While a 9-year Brazilian study found a slight increase (from 4.5% to 4.7%) in the prevalence of severe asthma among adolescents,13 an ecological study using data from Brazilian children and adolescents showed a slow but steady decrement in asthma mortality from 1980 to 2007, with the most marked decrement among children younger than 5 years.14
Consistent with findings elsewhere, urban residence is associated with higher risk of asthma in Latin America. Using the ISAAC video questionnaire in Oropeza (Bolivia), Solis Soto et al15 showed that children in urban areas had nearly twofold higher odds of asthma than those in rural areas. Similar findings were obtained in an ecological study of 59 transitional communities in Ecuador, where urbanisation was associated with higher prevalence of asthma (r=0.36, p=0.006).16 Although this rural–urban gradient in asthma could be due to differences in microbial or parasitic infections (the ‘hygiene hypothesis’), other factors (eg, stress, pollution) may play a role.
Ancestry, genetics and epigenetics
The wide variation in asthma prevalence and morbidity between two Hispanic subgroups in the USA (Mexican Americans and Puerto Ricans) has been described as the ‘Hispanic Paradox’,7 a term initially coined for overall and cardiovascular mortality.17 This paradox naturally extends to Latin America (where asthma burden is lowest in Mexico) and likely results from interactions between nature and nurture.
Latin Americans are often racially admixed, with heterogeneous proportions of European, Native American and African ancestry. Differences in racial ancestry could partly explain the ‘Hispanic Paradox’: whereas African ancestry has been associated with lower lung function in Puerto Rican children with and without asthma,18 Native American ancestry has been associated with higher lung function in Costa Rican adults with and without COPD.19 Moreover, a recent admixture study found a positive association between Native American subcontinental ancestry and lung function in Mexicans.20 Whether ancestral effects on lung function are due to correlated allelic variants or environmental exposures is unclear.
Relatively few studies have examined asthma genetics in Latin Americans, and even fewer have attempted to identify de novo susceptibility genes for asthma in this population. Most studies in Latin Americans include one of a few subgroups (Mexicans, Puerto Ricans, Costa Ricans, Colombians or Brazilians) and focus on replicating candidate genes identified in other populations (e.g. transforming growth factor beta 1 (TFGB1),21 the 17q21 locus,22 ,23 interleukin 13 (IL13),24 gluthatione S-transferase mu 1 (GSTM1),25 matrix metallopeptidase 9 (MMP9)26 and the beta2-adrenergic receptor (ADRB2)).27 ,28 On the other hand, two susceptibility genes for asthma-related phenotypes first identified in Latin Americans include thymic stromal lymphopoietin (TSLP)29 and matrix metalloproteinase 12 (MMP12).30 In both cases, findings in Costa Ricans have been replicated in non-Latin Americans.
Few genome-wide association studies (GWAS) of asthma have included subjects of Latin American descent, often used for replication purposes. Findings from a meta-analysis of GWAS of asthma in North American populations were replicated for four genes in ‘Latinos’: TSLP, interleukin 33 (IL33), interleukin 1 receptor-like 1 (IL1RL1) and the 17q21 locus.31 Unfortunately, the ‘Latino’ group was a mix of Costa Ricans, Hondurans, Puerto Ricans and US Hispanics, precluding conclusions about specific subgroups. Other GWAS of asthma or related phenotypes conducted in Latin Americans32 or including Latin Americans23 ,33 ,34 have not yielded genome-wide significant associations or failed to consistently replicate their findings in other populations, which may be explained by inadequate statistical power or false positive results. To date, no ethnic-specific asthma susceptibility gene has been identified in Latin American subgroups.
Few candidate-gene studies have examined gene-by-environment interactions, and only one study has examined asthma epigenetics in Latin America.35–38 Two studies replicated interactions between candidate genes (IL10 and TGFB1) and dust mite allergen in Costa Ricans in an independent cohort, and another demonstrated that violence exposure is associated with DNA methylation of the gene for the pituitary adenylate cyclase-activating polypeptide type 1 receptor (ADCYAP1R1), which is in turn associated with asthma in Puerto Rican children.
In summary, current evidence suggests that whereas most risk alleles for asthma are ‘cosmopolitan’ (affecting all ethnic groups to various degrees), some are ‘race/ethnic-specific’ (affecting only or predominantly certain groups).31 Large-scale genetic and epigenetic studies are needed to assess the relative contribution of risk alleles to asthma in Latin American subgroups, acting alone or interacting with the environment. Studies of this magnitude are challenging, but ISAAC3 and the Proyecto Latino-Americano de Investigación en Obstrucción Pulmonar (PLATINO) study of COPD39 are successful models of collaborative studies in Latin America.
Early-life risk factors
A cross-sectional study of 3003 infants in Brazil showed that risk factors for recurrent wheeze included daycare attendance, ≥6 colds in the first year of life (adjusted OR (aOR)=1.3, 95% CI 1.2 to 1.4)), pets other than dogs during pregnancy (aOR=1.3, 95% CI 1.1 to 1.5) and mould in the home. In contrast, up-to-date immunisations (aOR=0.8, 95% CI 0.6 to 1.0) and a bathroom in the home were inversely associated with recurrent wheeze.40 Similar findings were obtained in a study of >28 000 infants in Latin America (Brazil, Chile and Venezuela) and Europe (Spain and the Netherlands).41 In that study, risk factors for recurrent wheeze in Latin America included a cold in the first trimester of life, daycare attendance and maternal smoking during pregnancy; factors associated with lower risk of recurrent wheeze included breast feeding >3 months (aOR=0.8, 95% CI 0.7 to 0.9) and maternal education beyond high school (aOR=0.8, 95% CI 0.7 to 0.9). Similar findings for breast feeding were obtained in a recent cross-sectional study of Puerto Rican school-aged children, in whom breast feeding for ≤6 months was associated with 30% lower odds of asthma (95% CI 0.5 to 1.0).42
Little is known about perinatal events and asthma in Latin America. Among 678 Puerto Rican children ages 6–14 years,43 prematurity was associated with nearly fivefold increased odds of asthma in atopic children (95% CI 1.5 to 14.3). In contrast, there was no significant association in non-atopic children. Although findings from this cross-sectional study must be cautiously interpreted, they are consistent with a ‘two-hit’ hypothesis involving structural lung changes and atopy in the development of asthma in premature children.
In summary, current findings suggest that early-life risk or protective factors for recurrent wheeze in Latin American infants are similar to those identified elsewhere. Birth cohort studies are needed to assess the relative contribution of these exposures and identify novel risk factors for asthma in Latin America.
Diet and obesity
Vitamin D deficiency or insufficiency has been associated with asthma in Peruvian children and with severe asthma exacerbations in Costa Rican and Puerto Rican children.44–46 Other studies have focused on global diet instead of vitamins or nutrients, reporting that fast food47 or a ‘Western’ dietary pattern48 is associated with higher asthma risk in Mexico and Brazil, while higher fruit and vegetable intake or a ‘Mediterranean’ diet is associated with reduced airway inflammation and higher lung function in Mexican children.49
In one of few clinical trials of nutrients and asthma in Latin America, docosahexaenoic acid supplementation in the second and third trimesters of pregnancy led to lower risk (aOR=0.76, 95% CI 0.58 to 1.0) and shorter duration of colds, cough and wheezing in Mexican infants at age 1 month, but not at 3 or 6 months.50 Further clinical trials of dietary interventions on asthma are needed in this region.
Overweight and obesity affect ∼16–36% of children in Latin America.51 Consistent with findings elsewhere, overweight or obesity has been associated with asthma (aORs ∼1.3–1.8)52 ,53 or asthma severity53 ,54 in Latin Americans. However, the mechanisms or modifiers (eg, age, gender and type of obesity (general vs central)) of the putative effects of obesity on asthma remain unclear. Obesity has been associated with a pro-inflammatory state in Mexicans,55 in whom ‘obese asthma’ has been linked to metabolic syndrome.56 There has been no adequate clinical trial of weight loss and asthma in Latin America.
Psychosocial stress
Intimate partner violence, which is frequent in Latin America, is associated with adverse pregnancy outcomes.57 Similarly, perinatal depression can affect up to 20% of mothers.58 Consistent with findings outside of Latin America, stress, depression and mental illness in the mother or father have been linked to childhood asthma in Brazil59 ,60 and Puerto Rico.61
We reported that physical or sexual abuse is associated with asthma morbidity in school-aged Puerto Ricans.62 Exposure to violence has been associated with asthma or asthma symptoms among children in Brazil (aOR for symptoms=1.9, 95% CI 1.1 to 3.4)63 and Puerto Rico,38 and preliminary evidence suggests that this may be partly explained by ADCYAP1R1 methylation.38 More recently, we showed that child stress may affect asthma morbidity by reducing bronchodilator response (BDR), and that an ADCYAP1R1 single-nucleotide polymorphism is associated with both reduced ADRB2 expression and reduced BDR.64 To date, there has been no study of stress-reducing interventions on asthma in Latin America.
Infections and parasite infestation
Findings from Latin America suggest that chronic and heavy parasitic infection reduce the risk of atopy, while intermittent or light parasitic infection may increase such risk.65 ,66 Moreover, timing of infection may be key, as heavy infection with Trichuris trichiura and Ascaris lumbricoides during infancy has been shown to reduce the risk of atopy at school age among Brazilians (aOR=0.40, 95% CI 0.17 to 0.94).67
A. lumbricoides sensitisation (without or with concurrent infection) has been associated with asthma, wheeze or greater asthma severity68–70 among children in Costa Rica, Brazil and Ecuador (aOR for asthma ∼2.24 to 2.60, 95% CI 1.33 to 4.38; aOR for asthma hospitalisations=3.08, 95% CI 1.23 to 7.68). Whether this finding is explained by intermittent/light helminthiasis71 ,72 (affecting the immune system or the lung through larvae migration) or other mechanisms (eg, a genetic predisposition to poly-sensitisation or cross-reactivity with other allergens) is unclear.
Conflicting results illustrate the complex relation between parasitic infections and asthma in Latin America. Whereas some studies have shown that helminthiasis or toxocariasis increase the risk of non-atopic wheezing,73 airway hyper-reactivity,74 atopic asthma70 and severe asthma75 in Brazilian and Argentinean children, studies in Ecuadorean children have shown that active parasitic infections might reduce the risk of atopic wheeze68 ,76 or that treatment with anti-helminthics does not affect asthma symptoms.77 Longitudinal studies are needed to better delineate the roles of host and type of infection on asthma at different ages (as risk factors for early-childhood wheeze may protect against asthma later in life).
Consistent with findings elsewhere, early or frequent non-parasitic respiratory infections (eg, viral) have been associated with wheeze or asthma in Brazilian children.78–80 However, no study has used molecular-based techniques to assess the long-term impact of these infections on asthma in Latin Americans.
Allergens and pollutants
Exposure and sensitisation to dust mite allergens are common and associated with asthma in cross-sectional studies in Latin America.81 ,82 More recently, several studies have examined allergens other than dust mite and asthma in this region. Indoor exposure to fungi or mould has been associated with asthma symptoms, airway hyper-responsiveness and severe asthma exacerbations in Colombian, Costa Rican and Puerto Rican children.82–84 Among school-aged Puerto Ricans with and without asthma, mouse allergen was associated with higher FEV1 and lower risk of atopy (aOR=0.8, 95% CI 0.6 to 0.9) or allergic rhinitis (aOR=0.75, 95% CI 0.62 to 0.92).85 ,86 This finding is consistent with that of a North American study87 and may be due to the effects of anaerobic bacteria in murine faeces on immune responses.
Environmental tobacco smoke (ETS) and current smoking are risk factors for asthma morbidity. In a study from Argentina, ∼60% of the population was exposed to ETS in their homes and ∼90% at work.88 Active smoking is common among Latin American teenagers due to cultural factors, lack of regulation and poor law enforcement. Active smoking was associated with ∼83% increased odds of asthma in a study of Argentinean adolescents, who were more likely to be smokers when exposed to ETS at home.88 Further emphasising the detrimental effects of smoking, a study of 4738 Latin American adolescents in ISAAC showed that ≥27% of asthma symptoms were attributable to tobacco use.89
Air pollution is a risk factor for asthma morbidity in urban Latin America. Exposure to traffic exhaust (particularly from diesel-fuelled motor vehicles) was associated with cough, wheezing and lower lung function among children with asthma in Mexico City.90 Similar findings for lung function were reported for PM10 and NO2 in Brazilian children.91 In Argentina, children living near the country's main oil refinery had a higher prevalence of asthma and asthma exacerbations, and lower lung function than those living in other regions.92
Recent findings suggest joint detrimental effects of vitamin D insufficiency and traffic-related air pollution on severe asthma exacerbations in Puerto Ricans.93 Compared to children who had vitamin D sufficiency and lived furthest from a major road, those who had vitamin D insufficiency and lived closest to a major road had nearly fivefold higher odds of ≥1 severe asthma exacerbation in the previous year (95% CI 2.1 to 10.7). A study in Mexico City showed that children with low vitamin C levels and certain GSTM1 genotypes may be more susceptible to the negative effects of ozone exposure on lung function.37 These findings suggest that low levels of antioxidants such as vitamin D or C may lead to increased oxidative stress or, alternatively, more severe viral infections after exposure to pollutants.
Indoor pollution is a health hazard in rural Latin America: ∼27 million people use biomass fuels as a source of energy in rural Mexico. In a 1-year interventional study in Mexican women, using a Patsari stove for cooking reduced cough by ∼23% and wheeze by ∼70%, and decreased the rate of lung function decline.94 A global analysis of ISAAC (which included ∼46 500 Latin American children) reported an association between open-fire cooking and asthma symptoms.95
Management interventions and economic impact
Public health efforts have improved asthma management in some countries. An ecological study showed a marked decrement in hospitalisations and mortality from asthma in Costa Ricans from 1997–2000 to 2011, likely due to nationwide educational campaigns leading to greater prescription of inhaled corticosteroids (ICS).96 Similar findings were reported for Argentina between 1990 and 1999.97 Laws regulating public smoking may also have reduced hospitalisations for childhood asthma.98
As few as 40% of patients are compliant with long-term medications for asthma,99 and thus education is critical. In a Colombian study, lower educational status, older age and unemployment were associated with inadequate use of metered-dose inhalers.100 In other studies in Brazil and Chile, education on self-management led to improved asthma control.101 ,102 Medication cost is another major treatment barrier. A few studies of cost-effectiveness in Latin America have shown superiority of beclomethasone over other ICS, as well as of salmeterol/fluticasone over montelukast, in children whose asthma is not well controlled on ICS.103 ,104
Among 2074 patients from 10 Latin American countries, asthma had a negative impact on daily activities: ∼46% of people with mild asthma and ∼72% of those with severe asthma reported ≥1 unscheduled healthcare visit, representing up to 73.2% of annual asthma-related costs.105 Thus, monitoring disease control is key to asthma treatment. Sputum nitrite has been correlated with asthma morbidity in Peruvian children,106 and questionnaires used to assess disease control in the USA (childhood asthma control test for schoolchildren107 and Test for Respiratory and Asthma Control in Kids for preschoolers108) have been recently validated in Latin Americans.
Comprehensive approaches are critical for asthma control. The Programme for Control of Asthma and Allergic Rhinitis (ProAR), aimed at severe asthma in Salvador (Brazil), reported a 74% reduction in hospitalisations, as well as reductions in costs to the patient and healthcare system.109 Direct asthma-related costs for a participant's family were reduced from 24% to 2% of annual income.110 ProAR included specialised care, patient education and free medications (including ICS).
Little is known about the impact of comorbidities on asthma in Latin America. Although treating allergic rhinitis may reduce asthma morbidity, this disease is significantly underdiagnosed among children with asthma in Costa Rica111 and Puerto Rico.112 In the Puerto Rican study, physicians were shown to miss >75% of cases of allergic rhinitis in children with asthma.112 Such underdiagnosis could be easily corrected by asking about symptoms and triggers of rhinitis and measuring dust mite-specific IgE or total IgE.112
In summary, multipronged approaches to asthma management are needed. Such strategies must include adequate access to medications, patient education and monitoring asthma control.
Summary and future directions
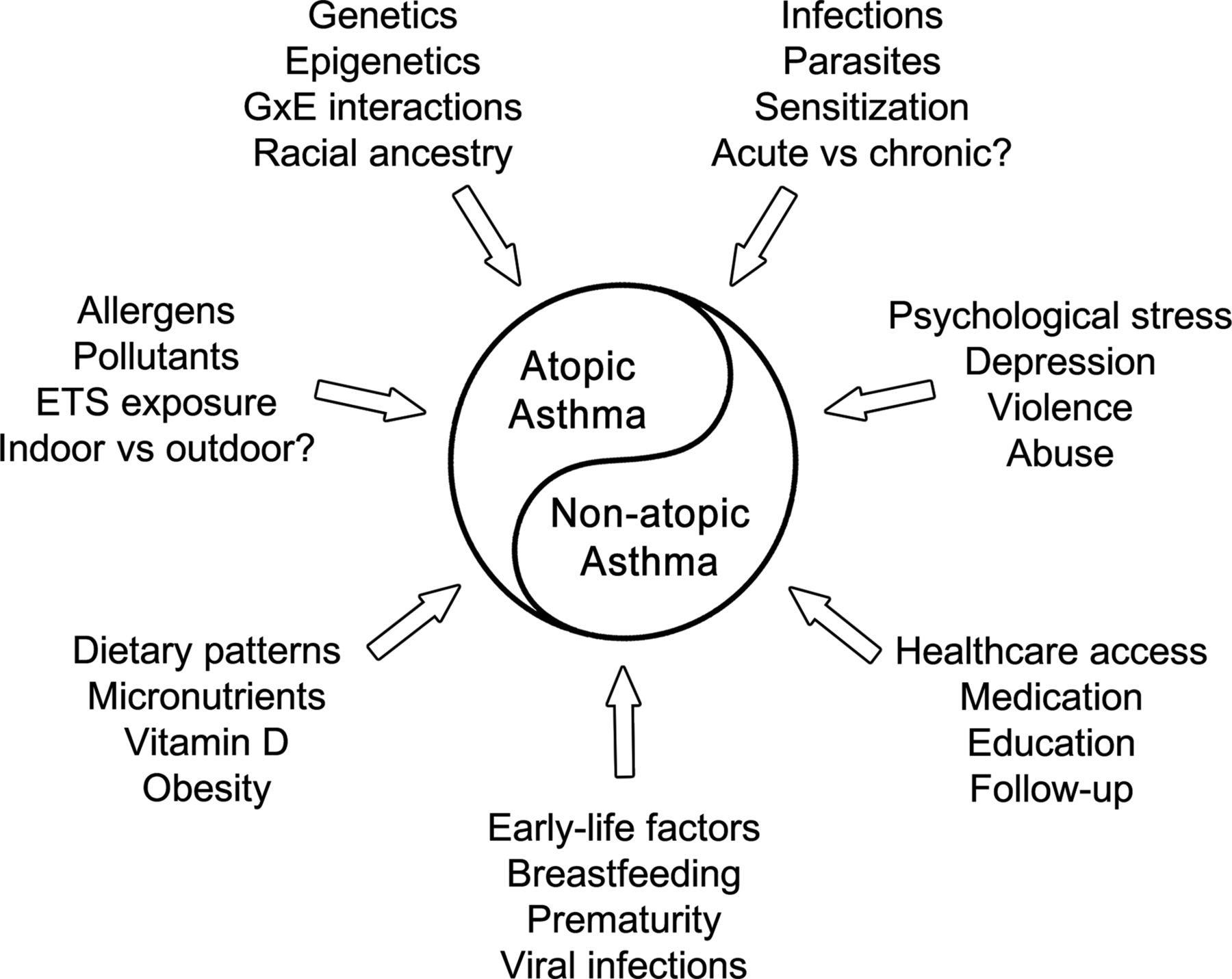
Asthma is a syndrome comprising distinct phenotypes (eg, atopic vs non-atopic asthma, ‘obese asthma’) and diverse risk factors (see online supplementary table for a summary of the most relevant articles). While some causes of these phenotypes may overlap, others may be unique to a phenotype. Given the size and diversity of Latin America, one expects to encounter variability in the relative importance of each asthma phenotype and its contributing risk factors (figure 2). Atopic asthma predominates in countries such as Costa Rica or Puerto Rico,69 ,84 while non-atopic asthma prevails in nations such as Ecuador or Brazil (particularly in rural or impoverished areas).113 ,114 However, over-reporting of non-atopic asthma is likely in studies that included young children, in whom transient wheeze (often non-atopic) is common and ‘true asthma’ is difficult to diagnose. Thus, longitudinal studies are needed to fully characterise the relative importance of diverse asthma phenotypes in Latin America. Such studies, including biomarkers often lacking in previous literature, would allow better characterisation of risk factors for asthma in this region.
{kind=link}
{kind=link}
Risk factors for asthma in Latin America. ETS, environmental tobacco smoke; GxE, gene-by-environment.
Because of the profound diversity of Latin Americans, genetic and epidemiological studies should include large subgroups that are defined with regard to place of birth, area of residence, migration history and racial ancestry. Given recent conflicts leading to forced displacement in several Latin American countries, the region offers a unique opportunity to examine the impact of these factors (and resulting stress) on asthma. Likewise, factors that may affect asthma and are common in certain Latin American countries deserve to be studied, including urbanisation, parasitic infections and biomass fuels. Along with these exposures, other emerging problems deserve attention, including diet and obesity.
Some problems may be unique to particular nations, but most Latin American countries share barriers to asthma management. Thus, concerted public health and research efforts could have a major impact at a regional level. Such efforts should include vigorous campaign to curtail and eliminate tobacco use, nationwide campaigns on asthma (directed at patients and healthcare providers), broadening access to care and clinical trials of relevant non-pharmacological interventions (eg, replacing biomass fuels with safe cooking techniques, violence and stress reduction, and weight loss).
References
Supplementary materials
Supplementary Data
This web only file has been produced by the BMJ Publishing Group from an electronic file supplied by the author(s) and has not been edited for content.
- Data supplement 1 - Online supplement
Footnotes
Contributors EF, MG, JAC-R and JCC contributed to the study concept, literature search, data collection and manuscript writing. AC, AY, DS, MS-Q, LA and PC contributed to the literature search and manuscript writing.
Funding This work was supported by grants HD052892, HL079966, HL073373 and HL117191 from the US National Institute of Health, and by the Heinz Endowments. Neither funding agency had any role in the preparation of this manuscript.
Competing interests None declared.
Provenance and peer review Not commissioned; internally peer reviewed.
Linked Articles
- Airwaves