Article Text

Abstract
Type-2 biomarkers and related cytokines (IL-5, IL-13), lung function and asthma symptoms were measured in 44 poorly-controlled severe oral corticosteroid (OCS)-dependent asthmatics for up to 88 days after a 7-day prednisolone boost (0.5 mg/kg). High-dose OCS reduced median blood eosinophils (−60 cells/µl; 95% CI −140 to 10), periostin (−8.4 ng/mL; −11.6 to –2.8), FeNO (−19.0 ppb; −28.5 to –4.0), IL-5 (−0.17 pg/mL; −0.28 to –0.08) and IL-13 (−0.15 pg/mL; −0.27 to –0.03). There were small improvements in mean FEV1 (0.16 L; 0.05 to 0.27) and (Asthma Control Questionnaire) ACQ-7 score (0.3; 0.0 to 0.7). Study measures returned to baseline 1-month postintervention. Following rescue OCS, 1 month is sufficient before using type-2 biomarkers to guide long-term treatment.
Trial registration number NCT01948401.
- asthma pharmacology
Statistics from Altmetric.com
Introduction
The effect of high-dose oral corticosteroids (OCS) in OCS-dependent asthmatics is currently unknown. This group is important as they represent a large proportion of the severe asthma population, are patients with multiple corticosteroid-associated morbidities and drive much of the healthcare cost of asthma.1 Type-2 biomarkers are used to guide treatment for novel biological therapies, making it important to understand the longitudinal stability of their profile following high-dose OCS. The aims of this study were to examine the trajectory of the type-2 biomarker profile in severe OCS-dependent asthmatics after additional high-dose OCS.
Methods
Participants aged between 12 and 75 with well characterised severe uncontrolled asthma were recruited from UK Severe Asthma Registry centres between July 2013 and February 2014. All patients were adherent with a maintenance dose of at least 10 mg prednisolone for at least 6 months prior to study initiation based on prednisolone/cortisol levels. Full details of study inclusion criteria are given in the online supplementary file 1. The study received Ethical Approval from National Research Ethics Service East of England (Ref: 13/EE/0099) and was registered on ClincalTrials.Gov (https://clinicaltrials.gov/ct2/show/NCT01948401).
Supplemental material
Subjects were offered a 7-day OCS escalation (0.5 mg/kg) and invited to attend four follow-up visits 1 (visit 2), 32 (visit 3), 60 (visit 4) and 88 (visit 5) days postintervention. Patient outcomes including type-2 biomarkers (blood eosinophils, FeNO, serum periostin), cytokines (serum IL-5, IL-13), spirometry (FEV1, FVC) and patient-reported symptoms (ACQ-7) were collected at baseline and during follow-up visits (see online supplementary tables e1, e2). Patients receiving additional rescue OCS for an asthma exacerbation during follow-up were excluded from future study visits.
Descriptive data are presented using the mean (SD) or median (IQR). For normally distributed variables, mean change from baseline was calculated for each follow-up visit, and paired t-tests used to formally test for differences. For non-normally distributed variables, median difference from baseline was calculated (with bootstrapped 95% CIs), and the Wilcoxon signed-rank test used to test for differences. We conducted separate short-term (visit, visit 2 and visit 3) and long-term (all study visits) analysis. For each outcome, patients with missing data at baseline, visit 2 or visit 3 where excluded from the short-term analysis. Similarly, patients with missing data at any study visit were excluded from the long-term analysis.
Results
Forty-four subjects were recruited and 17 completed long-term follow-up (6 did not consent to long-term follow-up, 2 did not attend study visits, 19 required rescue steroids) (online figure e1). Cohort details are given in table 1.
Baseline characteristics of the study population
In the short-term analysis, there were median decreases of 60 cells/µl (95% CI: 10, 140; p=0.004), 8.4 ng/mL (95% CI: 2.8, 11.6; p<0.001) and 19.0 ppb (95% CI: 4.0, 28.5; p<0.001) between baseline and visit 2 for blood eosinophils, serum periostin and FeNO, respectively (table 2, online figure e2). Serum IL-5 and IL-13 concentrations were reduced between baseline and visit 2 by 0.17 pg/mL (95% CI 0.08 to 0.28; p=0.002) and 0.15 pg/mL (95% CI 0.03 to 0.27; p=0.002), respectively. Blood eosinophils, serum periostin, FeNO and serum IL-5 concentration returned to baseline levels by visit 3 (visit 4 for cytokines), although serum IL-13 was slightly higher (0.07 pg/mL; 95% CI −0.01 to 0.33; p=0.028) than baseline (table 2, online figure e2) at this point. FEV1 (160 mL; 95% CI 50 to 270; p=0.005) and FVC (160 mL; 95% CI 40 to 280; p=0.009) showed small improvements after high-dose OCS (table 2, online figure e2), but were close to baseline by visit 3.
Short-term change in study measures between baseline visit (visit 1) and 1 day (visit 2) and 32 days (visit 3) after completing 7 days of high-dose oral corticosteroids (0.5 mg/kg)
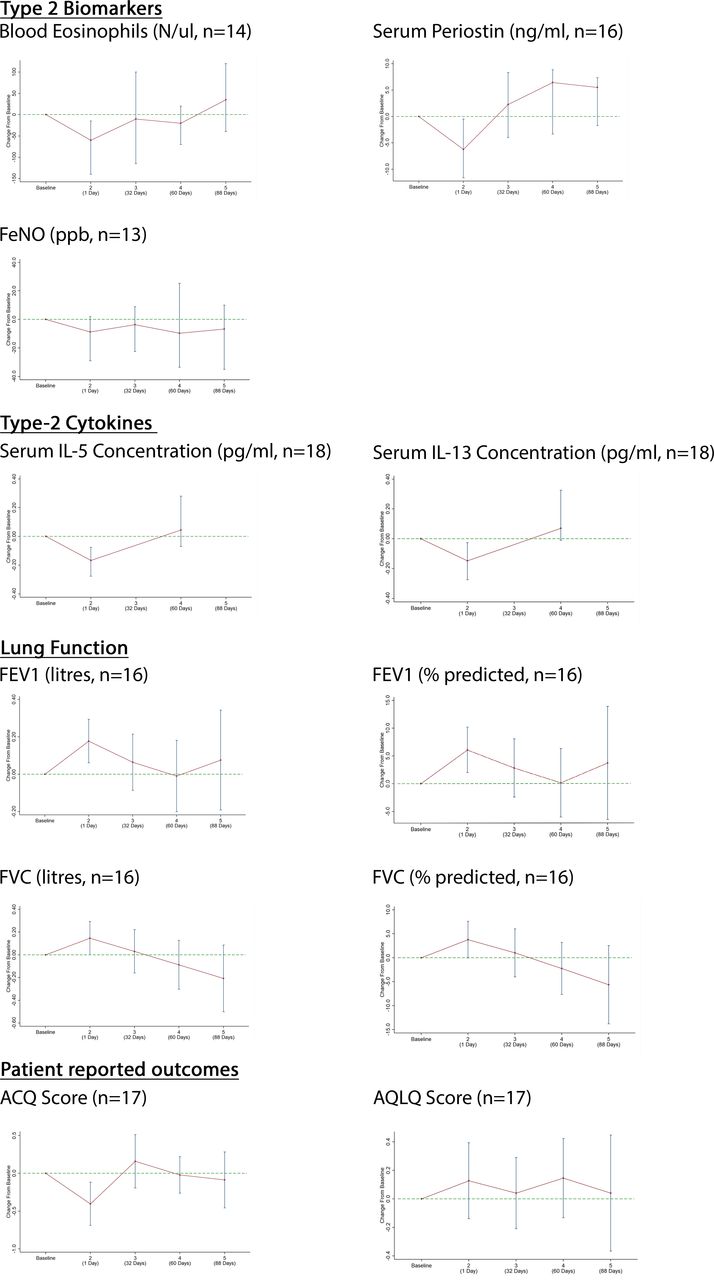
These short-term changes were replicated in patients with complete data to study end, although standard errors were noticeably larger due to a smaller sample size. Each of the study measures was close to baseline by visit 4 and remained relatively stable until visit 5 (figure 1, online supplementary table e3).
{kind=link}
Trajectories of type-2 biomarkers and cytokines, patient-reported outcomes (ACQ and AQLQ) and lung function (FEV1 and FVC) over serial study visits—subjects with missing data at any of the study visits or who required additional rescue corticosteroids for exacerbation in addition to the high-dose OCS between baseline visit and study 2 were excluded. Data are shown as median or mean difference (with 95% CIs) as appropriate.
Discussion
Seven days of high-dose OCS treatment significantly reduced type-2 biomarkers and related cytokine levels, but was associated with only small improvements in lung function and patient-reported symptoms. In general, all study measures had returned to baseline levels 1 month postintervention and remained stable until 3 months postintervention.
To our knowledge, this is the first study to investigate the effect of high-dose OCS in severe OCS-dependent asthmatics. Our data concur with studies of broader severe asthma populations which reported significant reductions in blood eosinophils2–4 and FeNO2–4 after high-dose OCS. Changes in serum type-2 cytokine levels have been variably reported.2 5 Increased FEV1 2–9 and improved ACQ scores3 4 have been reported after high-dose OCS in patients not on maintenance steroids.
Our results suggest that, after rescue steroids, clinicians should wait 1 month before using type-2 biomarkers to guide treatment in OCS-dependent asthmatics. This is particularly relevant for patients where type-2 biomarkers are used to guide treatment for biological therapies, where failure to account for recent high-dose OCS could lead to effective therapies being unnecessarily withheld. The high exacerbation rate observed within our study suggests that the issue of how to interpret type-2 biomarker results in light of recent rescue steroids is commonly faced in routine clinical practice. Our data confirm that high-dose OCS inhibit both the IL-5 and IL-13 pathways, but despite significant reductions in type-2 inflammation, patients had significant residual impaired lung function and high symptoms scores. This suggests that broad therapeutic targeting of the type-2 cytokine axis may still leave significant unmet clinical need.
The study has some potential weaknesses as it is observational and hence open to confounding. The first postintervention follow-up was 1 month after the intervention period, therefore a more precise timing of biomarker levels returning to baseline prior to this time-point could not be determined. However, type-2 biomarkers were decreased 2 weeks after prednisolone treatment for acute exacerbation, suggesting that shorter time periods are unlikely to be sufficient.10 We necessarily excluded patients who had additional rescue OCS to treat exacerbations during follow-up which reduced the sample size in our long-term analysis and may have hindered generalisability.
In summary, type-2 biomarker and serum cytokine levels are significantly suppressed after high-dose OCS treatment in OCS-dependent asthmatics, but return to baseline levels after 1 month. Following rescue steroids, 1 month is a sufficient time period before using type-2 biomarkers to guide long-term treatment decisions.
Footnotes
Contributors JB conducted the statistical analysis and drafted the manuscript. CTJH, AC, FC, JGM, TS and LGH contributed to the planning and conduct of the clinical trial including assay development and interpretation of data and critical review of the study. PB, RC, AHM, JLL, AM-G and RN contributed to the planning and conduct of the clinical trial, interpretation of data and critical review of the study. All authors reviewed and approved the final version of the manuscript. JB acts as study guarantor.
Funding Data were generated and supplied by Genentech Inc. Funding for the analysis was supplied by the Medical Research Council (MR/M016579/1).
Competing interests CH, AC, JGM, TS are (or were at time of study) employees of Genentech Inc., a Member of the Roche Group and own Roche stock. RC has attended Advisory Board Meetings for AstraZeneca, GSK, Novartis and Teva and been a speaker at meetings for AstraZeneca. She has attended conferences supported by Boehringer, Teva, AstraZeneca and received educational grants from Novartis and Aerocrine. AHM received personal and department funds for talks and advisory board meetings and was sponsored to attend national and international conferences from pharmaceutical companies that include GlaxoSmithKline, Astra Zeneca, Novartis, NAPP, Boehringer Ingelheim, Roche, Chiesi. AM-G has attended advisory boards with GlaxoSmithKline, Novartis, AstraZeneca, Boehringer Ingelheim and Teva. He has received speaker fees from Novartis, AstraZeneca, Vectura, Boehringer Ingelheim, Sanofi and Teva. He has participated in research with Hoffman La Roche, GlaxoSmithKline, Boehringer Ingelheim and Astra Zeneca. He has attended international conferences with Teva and Boehringer Ingelheim and has consultancy agreements with AstraZeneca, Sanofi and Vectura. RN has received an unrestricted grant of £10,000 from Novartis in 2010 towards development of clinical services at the University Hospital of South Manchester. He has run preceptorship programmes in 2015 and 2016. These programmes have resulted in payment to the University Hospital of south Manchester for amounts not exceeding £10,000. He has also performed lecturing at Pharmaceutically sponsored meetings for the following pharmaceutical companies in the last 3 years: Astra Zeneca (<£1000), Boehringer Ingelheim (<£2000) Boston scientific (<£5000) Chiesi (<£1000), Novartis < £10,000, Napp (<£2000), Teva (<£2000). He has sat on advisory boards for the following companies in the last 3 years (Astra Zeneca, Boehringer Ingelheim, Boston scientific, Chiesi, GSK, Novartis Vectura and Teva), receiving reimbursement not exceeding £5000 per company. He has received sponsorship support to attend international academic meetings from Astra Zeneca, Boehringer ingelheim, Novartis, GSK, Chiesi and TEVA. RN (or any members of his family) has no shares or any pecuniary interest in any pharmaceutical industry and has no shareholdings or dividends and is not a paid consultant for any company. LGH is Academic Lead for the Medical Research Council Stratified Medicine UK Consortium in Severe Asthma which involves industrial partnerships with a number of pharmaceutical companies.
Patient consent for publication Not required.
Ethics approval National Research Ethics Service East of England (Cambridge South Committee Ref: 13/EE/0099).
Provenance and peer review Not commissioned; externally peer reviewed.