Article Text

Abstract
Background: Systemic proinflammatory cytokines and oxidative stress have been described in association with peripheral muscle wasting and weakness of patients with severe chronic obstructive pulmonary disease (COPD), but their expression in skeletal muscle is unknown. The objectives of the present study were to determine muscle protein levels of selected cytokines in patients with COPD and to study their relationships with protein carbonylation as a marker of oxidative stress, quadriceps function and exercise capacity.
Methods: We conducted a cross sectional study in which 36 cytokines were detected using a human antibody array in quadriceps specimens obtained from 19 patients with severe COPD and seven healthy controls. Subsequently, selected cytokines (tumour necrosis factor (TNF)α, TNFα receptors I and II, interleukin (IL) 6, interferon γ, transforming growth factor (TGF) β and vascular endothelial growth factor (VEGF)), as well as protein carbonylation (oxidative stress index) were determined using an enzyme linked immunosorbent assay (ELISA) in all muscles.
Results: Compared with controls, the vastus lateralis of patients with COPD showed significantly lower protein ELISA levels of TNFα, which positively correlated with their quadriceps function, TNFα receptor II and VEGF. Protein ELISA levels of IL6, interferon γ and TGFβ did not differ between patients and controls. Quadriceps protein carbonylation was greater in patients and inversely correlated with quadriceps strength among them.
Conclusions: These findings do not support the presence of a proinflammatory environment within the quadriceps muscles of clinically and weight stable patients with severe COPD, despite evidence for increased oxidative stress and the presence of muscle weakness.
Statistics from Altmetric.com
Muscle dysfunction, characterised by reduced muscle strength and endurance, is one of the most important systemic manifestations of advanced chronic obstructive pulmonary disease (COPD), leading to reduced exercise tolerance, quality of life and survival.1 Oxidative stress and systemic inflammation, among other factors, are proposed contributors to this process of muscle wasting and dysfunction, although their actual roles remain debatable. For instance, serum levels of the cytokine tumour necrosis factor (TNF)α, its soluble receptors I and II and other inflammatory cytokines such as interleukin (IL) 6 and IL8 along with acute phase reactants were shown to be increased in patients with severe COPD and muscle wasting compared with patients with identical disease severity without weight loss.2–6
To date, only two studies7 8 have attempted to explore cytokine protein expression in the lower limb muscles of patients with severe COPD showing inconsistent results. Specifically, quadriceps of patients with severe COPD exhibited much greater levels of TNFα and inflammatory cell counts than controls in one study,7 while no immunohistochemical TNFα expression was detected in the muscles of patients or controls in the second study.8 Against this background, we hypothesised that patients with severe COPD and muscle weakness would exhibit increased levels of different cytokines, including TNFα, in their limb muscles. To test this hypothesis, we first sought to explore the profile of multiple proinflammatory and anti-inflammatory cytokines using a human cytokine antibody array in the quadriceps of patients with severe COPD, with a wide spectrum of body composition and weight, and in those of healthy subjects. On the basis of both our antibody array results and of those from the current literature,2–6 we quantified protein levels of selected cytokines in all muscles using an enzyme linked immunosorbent assay (ELISA). We also explored muscle oxidative stress levels by measuring total protein carbonylation. Finally, we also assessed whether muscle cytokine levels and protein oxidation, as measured by ELISA, were associated with quadriceps strength and/or exercise capacity in the patients.
METHODS
Subjects
Nineteen male patients with stable severe COPD and seven healthy control individuals from four different European geographical areas were recruited on an outpatient basis. All individuals were Caucasian, and were simultaneously participating in the project of the European Network for Investigating the Global Mechanisms of Muscle Abnormalities (ENIGMA) in COPD, specifically designed to investigate the mechanisms involved in muscle dysfunction in COPD (www.pul.unimaas.nl/enigma/enigma.htm). A diagnosis of COPD was established on the basis of the guidelines of the Global Initiative for Chronic Obstructive Lung Disease.9 The inclusion and exclusion criteria established in our study were identical in the four centres. All patients were exclusively receiving inhaled medication (long acting beta2 agonists, anticholinergics and low dose inhaled corticosteroids). Patients receiving oral corticosteroid treatment were not included in the study. The sample size of both patient and control populations was calculated on the basis of formerly published human studies, where similar physiological and biological approaches were used.7 8 10–12
Study design
This was a cross sectional study in which patients with COPD were compared with age matched healthy control subjects, designed in accordance with the ethical standards on human experimentation in our institutions. The ethics committees at IMIM-Hospital del Mar (Barcelona, Catalonia, Spain), Maastricht University Hospital (Maastricht, The Netherlands), Royal Brompton Hospital (London, UK) and Cruces Hospital (Barakaldo, Basque Country, Spain) approved all experiments. Informed written consent was obtained from all individuals (see the online supplement for additional information).
Nutritional and functional assessment
Nutritional evaluation included body mass index (BMI) and determination of the fat free mass index (FFMI) by bioelectrical impedance.13 Forced spirometry and determination of static lung volumes, carbon monoxide transfer and arterial blood gases were performed using standard procedures, and reference values by Quanjer and colleagues14 were used. Arterial blood gases were performed using standard procedures. Patients with COPD only performed a progressive incremental exercise test on a cycloergometer (Monark-Crescent 864; Varberg, Sweden).15 Quadriceps strength was evaluated in both patients and controls by isometric maximum voluntary contraction (MVC) and in response to magnetic stimulation of the dominant lower limb as formerly described, respectively16 17 (see the online supplement for additional information).
Biopsies
Muscle samples from patients with COPD and controls were obtained from the quadriceps (vastus lateralis) by open muscle biopsy, as described previously,10 11 at both IMIM-Hospital del Mar and Cruces Hospital (11 patients and five controls), while the needle biopsy technique18 was used at Maastricht University and Royal Brompton Hospitals (eight patients and two controls). Samples were 20–30 mg in size, on average. Muscle specimens were immediately frozen in liquid nitrogen and stored at −80°C for further analysis or immersed in an alcohol-formol bath for 2 h to be thereafter embedded in paraffin (see the online supplement for additional information).
Muscle biopsy analyses
All muscle biology analyses were conducted in the same laboratory (IMIM-Hospital del Mar).
Human cytokine antibody arrays
The expression of 36 cytokines was detected in the quadriceps muscles of both COPD patients and healthy controls using a specific human cytokine antibody array19 (Panomics, Inc. Redwood City, California, USA) following the manufacturer’s instructions (see the online supplement for additional information).
Cytokine ELISA
After a careful analysis of the microarray cytokine profile in the quadriceps of both COPD patients and controls and on the basis of former studies,2–6 protein expression of the cytokines TNFα, TNFα receptors I and II, IL6, interferon γ, transforming growth factor (TGF) β and vascular endothelial growth factor (VEGF) was quantified in all muscles using specific sandwich ELISA kits (Biosource Europe, Nivelles, Belgium) following the manufacturer’s instructions for each cytokine (see the online supplement for additional information).
Protein carbonyl ELISA
Total levels of those highly reactive carbonyl groups in the protein side chains were detected by reaction (derivatisation) with 2,4-dinitrophenylhydrazine using the protein carbonyl enzyme immunoassay kit (Zenith Technologies Corp. Ltd, Dunedin, New Zealand) following the manufacturer’s instructions (see the online supplement for additional information).
Immunohistochemistry
Muscle morphometry in both patients and controls was assessed as previously described.10 12 Monoclonal anti-MyHC-I (clone MHC; Biogenesis Inc., UK, 1/20 dilution) and monoclonal anti-MyHC-II (clone MY-32; Sigma, St Louis, Missouri, USA, 1/100 dilution) antibodies were used to identify type I and type II muscle fibres, respectively. At least 100 fibres were counted in each specimen (see the online supplement for additional information).
Statistical analysis
Data are presented as mean (SD) with 95% confidence intervals (CI) for parametric data (table 1) and as median (interquartile range) for non-parametric data (table 2). The unpaired t test or the Mann–Whitney non-parametric test was used for comparisons between controls and COPD patients. While 95% CI, mean differences and p values were indicated for the parametric t test, only exact p values were noted for the Mann–Whitney non-parametric test. Spearman’s correlation coefficient was used to assess relationships among different variables within all COPD patients. The sample size was based on assumptions of 80% power to detect an improvement of more than 20% in measured outcomes at a level of significance of p⩽0.05.
RESULTS
Characteristics of the study subjects
Table 1 shows the main characteristics of the study subjects. As expected, no significant differences were found in age between controls and patients with COPD, and pulmonary function testing confirmed the presence of advanced disease among the patient group. BMI and FFMI were significantly lower in patients compared with controls. Muscle strength, as evaluated by quadriceps MVC, was significantly reduced in patients compared with controls (mean (SD) MVC 40.4 (6.2) kg vs 29.9 (8.9); p = 0.02), although this did not achieve significance for twitch tension. The proportions of type I fibres were significantly lower while those of type II fibres were higher in the quadriceps of patients with COPD compared with controls (p = 0.03).
Microarray expression of the different cytokines
Table 2 shows the cytokine levels (optical densities expressed as arbitrary units) detected using the specific human cytokine antibody arrays (see the online supplement for additional information).
Muscle specific protein expression (ELISA measurements)
Expression of TNFα and TNFα receptors I and II
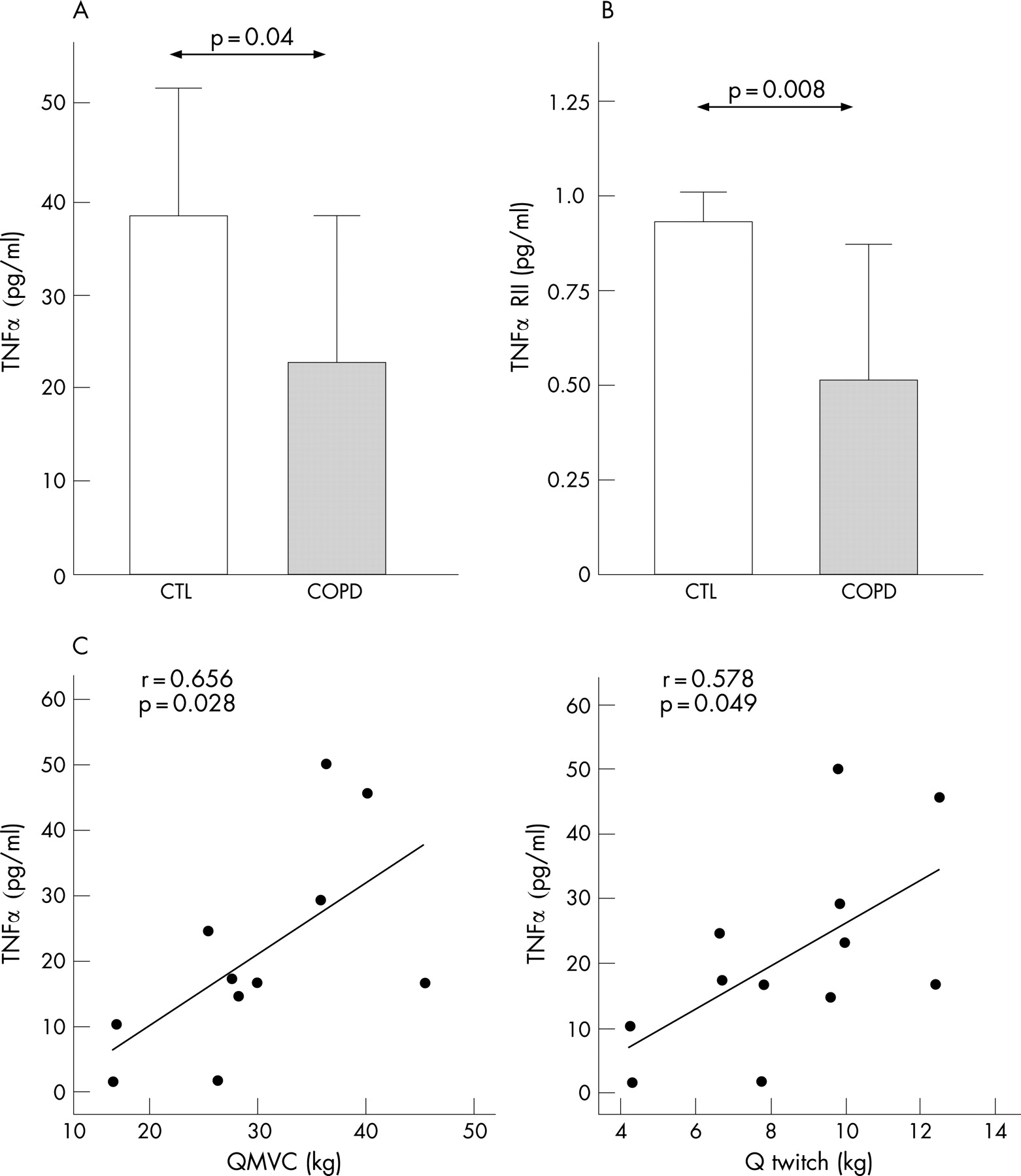
As shown in fig 1A, protein expression (ELISA measurements) of the cytokine TNFα was lower in the muscles of the patients with COPD compared with controls. No significant differences were observed in the levels of TNFα receptor I in the muscles of the COPD patients compared with those in controls (0.20 (0.051) pg/ml (95% CI 0.17 to 0.23) vs 0.21 (0.04) pg/ml (95% CI 0.157 to 0.256), mean difference +0.003 (95% CI −0.047 to +0.054)). However, ELISA levels of the TNFα receptor II were significantly reduced in the quadriceps of patients with COPD compared with controls (fig 1B). When the COPD patients were analysed as a group, muscle TNFα ELISA levels significantly and positively correlated with both MVC and the involuntary twitch force of the quadriceps (fig 1C). Moreover, TNFα levels were also positively correlated with those of the TNFα receptor II (r = 0.932, p<0.001). No other relationships were found between TNFα or TNFα receptors I and II and lung function, exercise tolerance parameters or fibre type distribution among all patients with COPD.
Expression of IL6, Interferon γ and TGFβ
Mean (SD) values for IL6, as measured by ELISA, did not differ between patients with COPD and controls (18.9 (3.1) pg/ml (95% CI 17.4 to 20.4) vs 19.5 (2.2) pg/ml (95% CI 16.8 to 22.2), mean difference +0.6 (95% CI −2.1 to +3.3)). Likewise, muscle protein levels of interferon γ did not show any significant difference between patients and controls (10.4 (1.7) IU/ml (95% CI 9.3 to 11.5) vs 11.9 (2.9) IU/ml (95% CI 8.2 to 15.6), mean difference +1.5 (95% CI −2.1 to +5.1)). Muscle levels of the cytokine TGFβ were also similar between patients with COPD and controls (23.2 (6.9) pg/ml (95% CI 19.9 to 26.5) vs 23.0 (2.5) pg/ml (95% CI 19.9 to 26.1), mean difference −0.1 (95% CI −4.2 to +3.9)).
Expression of VEGF
Protein levels of the cytokine VEGF (ELISA measurements) were significantly reduced in the quadriceps of COPD patients compared with control muscles (fig 2). No relationships were found between muscle levels of VEGF, lung or muscle functions, exercise tolerance parameters or fibre type distribution among all patients with COPD (see the online supplement for additional information).

Muscle protein carbonylation (ELISA measurements)
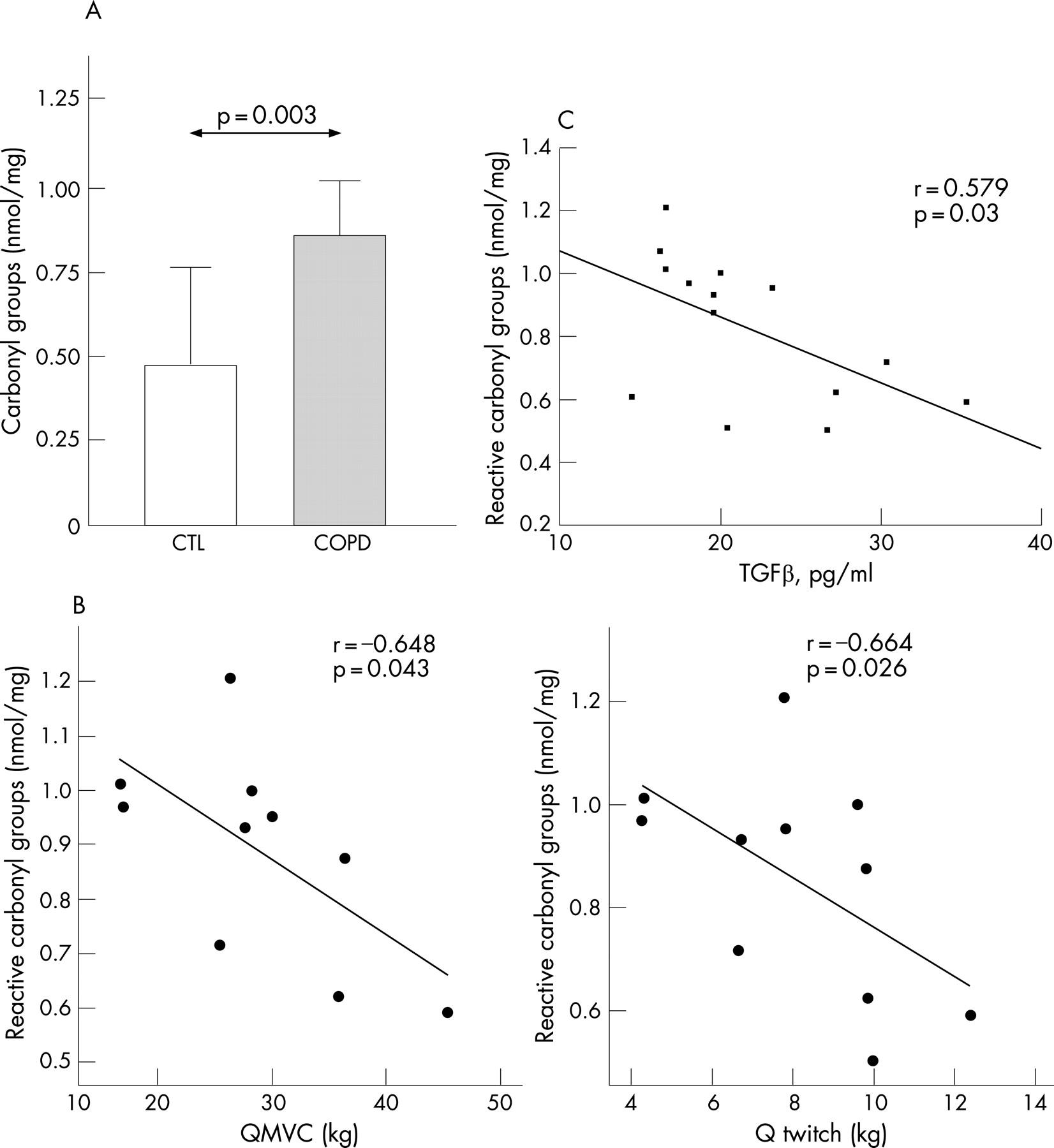
Muscle protein carbonylation levels were significantly higher in the quadriceps of COPD patients than in controls (fig 3A). When considering all COPD patients as a group, muscle protein carbonylation levels were significantly and negatively correlated with both MVC and the involuntary twitch force of the quadriceps (fig 3B), as well as with muscle levels of TGFβ (fig 3C). There was a trend towards an inverse correlation between TNFα levels and the magnitude of protein carbonylation in the muscles of all patients with COPD (r = −0.451, p = 0.08). No other relationships were found between muscle protein carbonylation, lung function, exercise tolerance parameters or fibre type distribution among all COPD patients.
{kind=link}
{kind=link}
{kind=link}
DISCUSSION
The main findings in this study were obtained as a result of a prospective exploratory approach using antibody microarrays followed by specific quantification of selected cytokines in the muscles. Hence, in patients with COPD compared with control subjects, we found that: (1) BMI, FFMI, quadriceps force and type I fibres were significantly reduced, (2) muscle TNFα levels were significantly reduced and positively correlated with quadriceps strength, (3) muscle levels of the TNFα receptor II were also significantly reduced and were related to those of TNFα, (4) muscle levels of the cytokine VEGF were lower and (5) muscle protein oxidation, as measured by total protein carbonylation, was significantly increased and negatively correlated with quadriceps muscle strength among all patients.
Study limitations
The main limitations of our study are related to the small size of the muscle specimens and the relatively small number of both patients and controls recruited. As the study involved the use of relatively “invasive” procedures and many different tests were performed in most of the study subjects, we were compelled to obtain rather small muscle specimens. In addition, the volunteer healthy control individuals were recruited on an outpatient basis and had not been hospitalised for any reason in the previous months before study entry as opposed to former studies where subjects underwent surgical procedures. Moreover, very restrictive inclusion and exclusion criteria were used to carefully select the study population. Another limitation encountered in our study was directly related to the methodology. As we chose quite a comprehensive exploratory approach to the study of levels of several cytokines in the quadriceps of our population, we were compelled to use those types of laboratory techniques that require relatively little amounts of sample because of their high sensitivity. It should also be mentioned that the results obtained using the antibody microarray on the one hand, and the ELISA on the other, showed some discrepancies with regard to protein expression of the cytokines interferon γ and TGFβ. The fact that the former is basically a qualitative exploratory technique whereas the latter is an accurate method to specifically quantify protein levels probably account for such discrepancies. Moreover, the ELISA results were confirmed and verified by repetition of some of the experiments as well as by the use of triplicates in all cases.
Quadriceps muscle structure and function
Quadriceps muscle dysfunction has been well established in the past decade16 20–22 Among several mechanisms, decreased proportions of type I fibres have been observed in association with quadriceps muscle dysfunction of patients with COPD.22 In the present study, compared with controls, both quadriceps strength and proportions of type I fibres were reduced in patients. These findings are indeed consistent with the current literature20–24 and suggest that our cohort was typical of patients with advanced disease.
Cytokines in the vastus lateralis
TNFα is a pleotropic cytokine that has long been considered to be involved in the muscle loss of patients with chronic wasting conditions, such as cancer and COPD. In fact, it has been shown that systemic inflammatory cytokines such as TNFα, its soluble receptors I and II, IL6 and IL8, along with acute phase reactants, are increased in the blood of patients with severe COPD and muscle wasting compared with healthy controls.2–6 25 In line with this, other studies have also demonstrated an increase in various blood inflammatory cells, which might be involved in the release of systemic inflammatory cytokines in COPD patients.6 26 27 Furthermore, systemic TNFα has been proposed to exert catabolic actions in muscles as well as to induce contractile dysfunction in chronic inflammatory conditions, including COPD.28 In keeping with this, TNFα has been shown to inhibit myogenesis through several mechanisms in in-vitro studies.29 30 However, the argument has been put forward that TNFα may also promote skeletal muscle regeneration and remodelling, as demonstrated in animal and in-vitro studies.31 32
In the present study, refuting our initial hypothesis, ELISA protein levels of both TNFα and its receptor II were reduced by approximately 45% in the quadriceps of our COPD patients compared with levels detected in controls. Furthermore, among all patients, significant positive correlations were found between quadriceps force and muscle TNFα levels, suggesting that this cytokine is somehow involved in the muscle contractile performance of these patients. Recent observations from some of us,33 34 however, have shown increased mRNA and protein levels of TNFα in the diaphragms and external intercostals of patients with COPD compared with controls. This is also consistent with former studies where expression of TNFα, IL6, IL1β and interferon γ was increased in the diaphragms of rats exposed to resistive breathing35 as well as in the myocardium of rodents subjected to mechanical loading.36 Collectively, these results raise the hypothesis that the expression of proinflammatory cytokines within muscle fibres is likely to be differentially regulated on the basis of the activity of each muscle.
In line with our findings, a recent study has also shown the absence of immunohistochemical TNFα expression as well as very low levels of neutrophils in the quadriceps of patients with severe COPD with and without hypoxaemia either at rest or after local exercise.8 Montes de Oca et al,7 however, have recently shown a large increase in TNFα levels and other inflammatory parameters, as well as in leucocyte counts in the quadriceps of patients with severe COPD with normal and low BMI. To explain the discrepancy, we note that patients in our study were more severely malnourished, that body composition, as assessed by the FFMI, was not explored in the study of Montes de Oca et al and that inflammatory cell counts were only performed in four patients,7 and not in the whole population of their study. Clearly, the design of future studies is required in order to unravel these important questions. We suggest that examining levels of inflammatory cells, which we now predict are probably very low in the limb muscles of our patients, would be worthwhile as well as prestratification of COPD patients by muscle atrophy profile. Data thus far suggest an absence of inflammatory cells in the quadriceps of patients with severe COPD compared with control muscles.24 On the other hand, the possible contribution of increased circulating blood cytokines to muscle dysfunction in COPD patients cannot be ruled out in our study as no blood analyses were performed. We believe this factor should also be taken into consideration in future studies.
Another factor that might be implicated in the regulation of the expression of muscle cytokines in severe COPD is hypoxia. We do not believe, however, that chronic hypoxia has taken place in the limb muscles of our COPD patients because their hypoxaemia was relatively mild (mean Pao2 9.2 kPa) and we saw no correlation between TNFα and Pao2. On the other hand, quadriceps muscle vascular remodelling and angiogenesis have been suggested to be reduced in COPD.23 37 38 Hence, the decreased VEGF protein expression observed in the quadriceps of our severe COPD patients could partially account for the proposed reduced remodelling of these muscles.
Muscle oxidative stress and its relationships with muscle cytokines
We and other investigators6 8 10–12 39–43 have already shown that protein oxidation is increased in the muscles of patients with COPD. Indeed, oxidative stress has widely been proposed as one of the most important mechanisms involved in the aetiology of peripheral muscle dysfunction in COPD. In the current study, we confirmed once more that lower limb muscle proteins undergo severe oxidation. Moreover, two novel findings are being reported: among all COPD patients, protein carbonylation was negatively associated with both quadriceps muscle function and TGFβ levels in these muscles. These results support the concept that oxidation of target muscle proteins likely to be involved in muscle force generation contributes to peripheral muscle dysfunction in severe COPD. In line with this, we have recently demonstrated11 that creatine kinase is more oxidised in the quadriceps of patients with severe COPD and that the activity of such an enzyme was inversely related to its levels of oxidation.
In our study, increased protein oxidation was inversely related to cytokine expression in the quadriceps of patients with very severe COPD and relative muscle loss. The molecular sources of oxidants in the quadriceps of COPD patients remain to be elucidated. On the basis of studies conducted on models of disuse and atrophy, it could be speculated that xanthine oxidase, reactive iron and probably NADPH oxidase would produce reactive oxygen species that may further react with nitric oxide to form the highly reactive species peroxynitrite, which, in turn, would lead to the formation of 3-nitrotyrosine. On the other hand, growing evidence shows that nitric oxide may also inhibit cytokine production in skeletal muscles.44 Therefore, it would be possible to conclude that excessive reactive nitrogen species production, as shown to occur in the quadriceps of patients with COPD,10 might partly account for the reduced cytokine protein levels encountered in the current study. Clearly, the design of future studies targeted to explore the specific roles of oxidative stress, molecular sources of reactive oxygen species and cytokine expression as well as the potential links among them in the COPD associated peripheral muscle dysfunction is of paramount importance.
CONCLUSIONS
Our findings do not support the presence of a proinflammatory environment within the quadriceps muscles of patients with severe COPD, despite evidence for increased oxidative stress and the presence of muscle weakness.
Acknowledgments
This study was supported by the European Network for Investigating the Global Mechanisms of Muscle Abnormalities in patients with Chronic Obstructive Pulmonary Disease (ENIGMA in COPD) (QLK6-CT-2002-02285) (European Union), and both RESPIRA (RTIC C03/11) and FIS 05/2486 (Spain). Dr Esther Barreiro is a scholar of the Fondo de Investigación Sanitaria (FIS) of the Spanish Health Ministry. We gratefully acknowledge Mr Francesc Sanchez and Ms Sandra Mas for their technical assistance in the laboratory, Dr Rafael Marcos for his technical assistance with the statistical analyses and Mr Roger Marshall for his editing aid.
REFERENCES
Supplementary materials
Web Only Data thx.2007.078030
Files in this Data Supplement:
Footnotes
-
Competing interests: None.
-
Ethics approval: Yes.