Article Text

Abstract
Background: The cause of acute exacerbation of chronic obstructive pulmonary disease (COPD) is often difficult to determine. Pulmonary embolism may be a trigger of acute dyspnoea in patients with COPD.
Aim: To determine the prevalence of pulmonary embolism in patients with acute exacerbation of COPD.
Methods: 123 consecutive patients admitted to the emergency departments of two academic teaching hospitals for acute exacerbation of moderate to very severe COPD were included. Pulmonary embolism was investigated in all patients (whether or not clinically suspected) following a standardised algorithm based on d-dimer testing, lower-limb venous ultrasonography and multidetector helical computed tomography scan.
Results: Pulmonary embolism was ruled out by a d-dimer value <500 μg/l in 28 (23%) patients and a by negative chest computed tomography scan in 91 (74%). Computed tomography scan showed pulmonary embolism in four patients (3.3%, 95% confidence interval (CI), 1.2% to 8%), including three lobar and one sub-segmental embolisms. The prevalence of pulmonary embolism was 6.2% (n = 3; 95% CI, 2.3% to 16.9%) in the 48 patients who had a clinical suspicion of pulmonary embolism and 1.3% (n = 1; 95% CI, 0.3% to 7.1%) in those not suspected. In two cases with positive computed tomography scan, the venous ultrasonography also showed a proximal deep-vein thrombosis. No other patient was diagnosed with venous thrombosis.
Conclusions: The prevalence of unsuspected pulmonary embolism is very low in patients admitted in the emergency department for an acute exacerbation of their COPD. These results argue against a systematic examination for pulmonary embolism in this population.
- COPD, chronic obstructive pulmonary disease
Statistics from Altmetric.com
Chronic obstructive pulmonary disease (COPD) is a leading cause of morbidity and mortality worldwide, and represents a huge economical burden for the healthcare system.1,2 Acute exacerbation of COPD is a frequent reason for visit to the emergency department.3 The most common triggers of exacerbations are infections of the tracheobronchial tree4,5 and air pollution,6 but the cause of exacerbation is impossible to determine in up to 30% of cases.7
Clinical presentation of COPD exacerbation includes worsening of dyspnoea, increased cough and sputum, and changes in the aspect of expectorations. Although clinical criteria have been used to determine which patient should be treated with antibiotics,8 these criteria are neither sensitive nor specific enough to exclude other causes of dyspnoea in this population. Other frequent clinical conditions may mimic the symptoms of COPD exacerbation, including congestive heart failure, pneumonia, pneumothorax, pleural effusion and pulmonary embolism.7
On the other hand, COPD is often cited among the risk factors for acute venous thromboembolism and was recently identified as an independent predictor of pulmonary embolism.9 In a small series of patients, the prevalence of deep vein thrombosis in patients admitted with acute exacerbation of COPD was 31%.10,11 Similarly, on the basis of ventilation–perfusion lung scintigraphy, the prevalence of pulmonary embolism in patients admitted with acute exacerbation of COPD was as high as 20%.12,13 More recently, Tillie-Leblond et al14 explored the prevalence of pulmonary embolism in a cohort of patients with COPD with unexplained dyspnoea and found a rate of 25% in this population. However, that study was performed in a highly selected subgroup of patients, and does not resolve the dilemma that primary care and emergency doctors face when taking care of acute exacerbation of COPD.
Our prospective study aimed to determine the prevalence of pulmonary embolism in patients presenting to the emergency department with acute exacerbation of COPD, using a validated diagnostic strategy based on the use of d-dimer, lower limb ultrasonography and multidetector computed tomography.15
MATERIALS AND METHODS
Study design and setting
This was a cross-sectional study performed in the emergency departments of two general teaching hospitals in Geneva and Lausanne, Switzerland, admitting 60 000 and 35 000 patients/year, respectively.
Study population
All consecutive adult patients having moderate to very severe COPD according to the global initiative for chronic obstructive lung disease definition7 and admitted for an acute exacerbation of their COPD were eligible for the study. COPD had to be confirmed by pulmonary testing during the index admission. Exacerbation was defined as any worsening of dyspnoea sufficiently severe to warrant an admission to the emergency room. Patients with renal failure (plasma creatinin ⩾150 μmol/l), allergy to intravenous contrast medium, on long-term anticoagulation therapy at admission or in respiratory distress requiring intubation/non-invasive ventilation were excluded. Patients with an obvious alternative cause of dyspnoea (lobar pneumonia, pneumothorax, pulmonary oedema and other obvious causes) were also excluded.
Study protocol
Every patient was evaluated by the emergency room physician with a standardised protocol including clinical evaluation, chest x ray, electrocardiogram and arterial blood gas analysis. For each patient, the clinician had to determine whether pulmonary embolism could be clinically suspected or not. No suspicion of pulmonary embolism was defined as a patient in whom the physician-in-charge would not have examined for a pulmonary embolism outside the study. After the initial clinical evaluation, pulmonary embolism was investigated in all included patients following a standardised validated algorithm based on d-dimer (rapid enzyme-linked immunosorbent assay, Vidas-DD Exclusion, BioMérieux, Marcy L’Etoile, France) measurement, lower-limb ultrasonography and multidetector helical computed tomography scan.15 A plasma d-dimer value <500 μg/l ruled out pulmonary embolism, and no further examination was performed.15,16 For patients with a d-dimer value >500 μg/l, both the lower-limb compression ultrasonography of the proximal veins and thoracic multidetector helical computed tomography scan were performed according to a previously published algorithm.15
Ultrasonographic criteria for deep-vein thrombosis were non-compressibility or incomplete compressibility of the vein.17 Computed tomography scans were obtained using a 16-slice multidetector-row computed tomography. These examinations were performed in breath hold, with the injection of 100 ml of non-ionic contrast material (iopromide; Ultravist-300R, Schering, Baas, Switzerland), with a power injector at 3 ml/s, using a slice thickness of 1.5 mm, tube voltage of 120 kV and tube current of 200 mA. In patients with a body mass index of >30 kg/m2, the volume of contrast material was increased to 120 ml and the tube voltage to 140 kV. Pulmonary embolism was diagnosed if contrast material outlined an intraluminal defect, or if a vessel was totally occluded by low-attenuation material.15
Outcomes
The main outcome measure was the proportion of patients diagnosed with pulmonary embolism, globally and in the subgroups of patients with or without clinical suspicion of pulmonary embolism. These groups were compared in terms of demographic characteristics and clinical presentation using χ2 or Fisher’s exact tests for categorical and t tests for continuous data (SPSS V.11.0 for windows).
The full study design was reported previously.18
Ethics
The protocol was approved by our institutional review board, and each patient gave his or her written informed consent to participate.
RESULTS
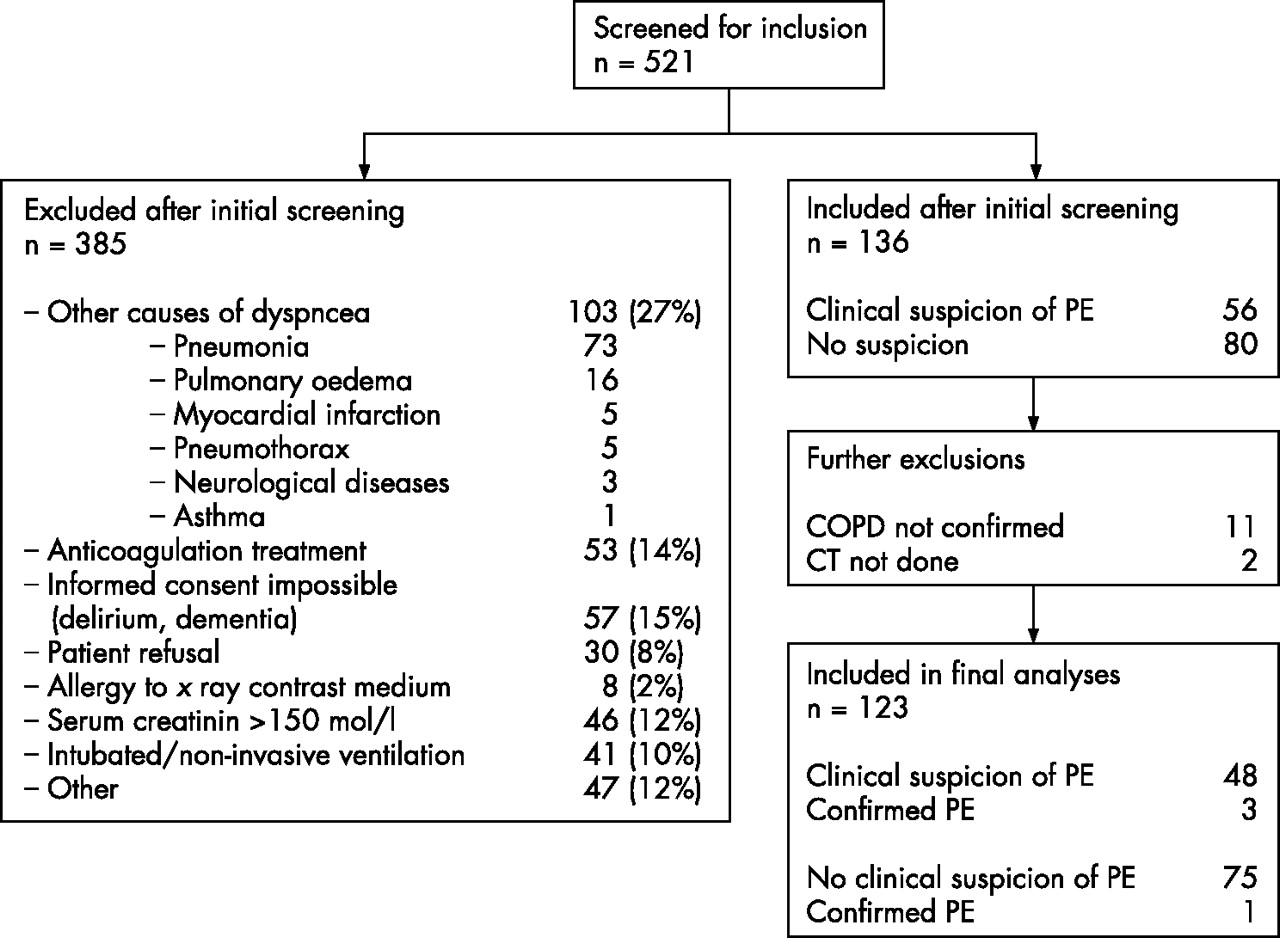
In all, 521 patients were screened for inclusion between 11 February 2003 and 17 December 2004. A total of 385 patients were excluded after the initial screening. Figure 1 summarises the reasons for exclusion. Thus, 136 patients were initially included. Thirteen patients were further excluded: eleven because COPD was not confirmed on spirometry and two because computed tomography scan was not performed. Table 1 shows the characteristics of the 123 included patients.
Characteristics of patients (n = 123) with acute exacerbation of their chronic obstructive pulmonary disease

{kind=link}
Study flowchart summarising inclusion and exclusion processes and main outcomes. COPD, chronic obstructive pulmonary disease; CT, computed tomography; PE, pulmonary embolism.
On the basis of their initial clinical evaluation, the emergency department physicians suspected pulmonary embolism in 48 (39%) patients and did not suspect it in 75 (61%) patients. No statistically significant differences were seen between both groups of patients in terms of age groups, sex ratio, pulmonary embolism risk factors, chest x ray and electrocardiogram findings (data not shown). Few differences were observed in the clinical presentation: chest pain was present in 42% of the patients with a clinical suspicion of pulmonary embolism, compared with 19% of the patients without suspicion (p = 0.008), but the pain characteristics were similar in both groups. Cough was less frequent when pulmonary embolism was suspected (75% v 93%, p = 0.009). Similarly, sputum was less frequent when pulmonary embolism was suspected (54% v 77%, p = 0.016), but sputum characteristics were similar in both groups when sputum was present. Syncope was the presenting complaint in 3 (6%) patients with clinical suspicion of pulmonary embolism and in none of the remaining patients (p = 0.051). Finally, severe hypoxaemia was more frequent in patients suspected of having pulmonary embolism: 48% of the patients suspected of having pulmonary embolism had arterial partial pressure of oxygen values <8 kPa compared with 20% in the group of patients not suspected of having pulmonary embolism (p = 0.003).
d-dimer value was obtained for all patients. Pulmonary embolism was excluded on the basis of normal (<500 µg/l) d-dimer levels in 28 (23%) patients (table 2).
Results of d-dimer, lower-limb ultrasonography and chest computed tomography scan in 48 patients with a clinical suspicion of pulmonary embolism and in 75 patients without clinical suspicion of pulmonary embolism
The percentages of negative d-dimer (<500 µg/l) were similar in patients with and in those without a clinical suspicion of pulmonary embolism. Computed tomography scan of the lung was performed in 95 (77%) patients and lower-limb ultrasonography in 90 (73%) patients. In 5 (4%) patients, venous ultrasonography could not be performed for practical reasons.
Computed tomography scan of the lungs showed pulmonary embolism in 4 (3.3%) patients (95% CI 1.3% to 8.0%), including three lobar and one subsegmental pulmonary embolism. In two cases, the lower limb ultrasonography also showed a proximal deep-vein thrombosis. None of the patients with a negative computed tomography scan was diagnosed with deep-vein thrombosis in lower limb ultrasonography. Pulmonary embolism was diagnosed in 3 (6.2%) patients (95% CI 2.3% to 16.9%) who had a clinical suspicion of pulmonary embolism and in 1 (1.3%) patient (95% CI 0.3% to 7.1%) who had no suspicion (table 2).
DISCUSSION
In this prospective series of 123 patients with moderate to severe COPD admitted with worsened dyspnoea, we found that the prevalence of pulmonary embolism was very low. Indeed, a diagnostic procedure based on systematic d-dimer testing, lower-limb ultrasonography and computed tomography scan of the lungs identified pulmonary embolism in only 4 (3%) patients (95% CI 1% to 8%). This prevalence was even lower in the subgroup of patients without a clinical suspicion of pulmonary embolism in the emergency room. In this subgroup, only one pulmonary embolism was diagnosed by our systematic examination (prevalence 1.3%). The three remaining cases were suspected by the emergency doctor and would have been diagnosed outside the study.
These results contrast strikingly with studies suggesting that the prevalence of pulmonary embolism might be as high as 15–25%. These differences may have different explanations. First, the imaging method used for diagnosing pulmonary embolism is crucial in a population of patients with chronic lung diseases. Ventilation–perfusion scintigraphy was used in previous studies.12,13 Although scintigraphy is an acceptable tool for the diagnosis of pulmonary embolism in patients without underlying lung diseases, the interpretation of lung scintigraphy is difficult in patients with COPD, which might have led to an overestimation of the true prevalence of pulmonary embolism in that population.19 In contrast, the performance of computed tomography scan is not altered in patients with COPD.19,20 We used a validated algorithm based on multidetector computed tomography scan,15 which should have minimised the risk of false-positive findings.
Secondly, most studies exploring the relationship between COPD exacerbation and deep-vein thrombosis or pulmonary embolism were retrospective or were based on autopsy findings.9,21,22 Our prospective design and our inclusion criteria limited selection biases.
Thirdly and most importantly, we studied an unselected population of patients admitted to the emergency room of two general teaching hospitals with an acute exacerbation of their COPD. Some studies included only the most severely ill patients admitted to intensive care units.11 Others excluded patients with normal d-dimer values.13 In our study, 23% of the patients had d-dimer values <500 μg/l excluding pulmonary embolism. Excluding these patients would overestimate the true prevalence of pulmonary embolism in an unselected population of patients with COPD with acute exacerbation.
Nevertheless, none of those explanations account for the striking difference between our findings and the 25% prevalence of pulmonary embolism recently reported by Tillie-Leblond et al.14 That series was prospective and used multidetector computed tomography. The inclusion criteria seemed similar to those of our study and are summarised as exacerbation of COPD of unknown origin. However, their criteria for lower respiratory infection were broad, and they excluded patients with increased sputum volume and/or increased sputum purulence, fever, history of cold and sore throat. We included those patients, except when the initial x ray showed obvious signs of pneumonia. This might account for part of the difference in pulmonary embolism prevalence compared with our series. However, the gap remains large, and we feel that the main difference was truly the clinical setting and patient selection. The French study was conducted in a large referral inpatient respiratory disease department, whereas our population was representative of the patients treated by emergency physicians in general hospitals. Furthermore, 29% of the patients with COPD in the French study had cancer compared with only 5% in our series.
Our study has some limitations. Firstly, the number of excluded patients was relatively high. But 41% of those patients were excluded for reasons unlikely to have introduced bias (refusal or inability to consent, ongoing oral anticoagulant treatment, allergy or renal failure). Patients who were excluded because exacerbation of their dyspnoea was attributed to another cause had very clear alternative diagnoses. In particular, pneumonia was defined by both a consolidation on chest x ray and a compatible clinical presentation (fever and purulent sputum). Therefore, only 10% of the patients were excluded because they required non-invasive ventilation or intubation and who were not able to undergo a computed tomography scan. Whether the prevalence in this subgroup could be higher as suggested by Schonhofer and Kohler11 is unknown. Secondly, the small number of cases of pulmonary embolism did not allow us to explore whether clinical or biological characteristics could identify a subgroup of patients with a higher prevalence of pulmonary embolism. Despite this limitation and although this was not a primary objective of this study, we were able to identify some clinical characteristics that led the emergency physician to suspect pulmonary embolism. Pulmonary embolism was more frequently suspected in the presence of chest pain, in the absence of purulent sputum or in the presence of a severe hypoxaemia.
In conclusion, our results stand against a high prevalence of unsuspected pulmonary embolism in patients admitted for an acute exacerbation of their COPD and against a systematic examination for pulmonary embolism in these patients. However, further studies are needed to confirm our findings in similar groups of patients. When pulmonary embolism is clinically suspected, a diagnostic strategy based on d-dimer testing, lower-limb ultrasonography and multidetector computed tomography scan is appropriate.
Acknowledgments
We thank Louise Riberdy who collected the data in Geneva.
REFERENCES
Footnotes
-
Published Online First 13 November 2006
-
Funding: This project was supported by the Swiss National Fund for Scientific Research Grant # 3200-068146. The researchers are independent from funders.
-
Competing interests: None declared.