Article Text

Abstract
A review of the most relevant evidence based therapeutic options currently available for the management of exacerbations of COPD
- COPD, chronic obstructive pulmonary disease
- CRP, C-reactive protein
- FEV1, forced expiratory volume in 1 second
- LABA, long acting inhaled β2 agonist
- LABD, long acting bronchodilator
- MDI, metered dose inhaler
- NIV, non-invasive ventilation
- PEFR, peak expiratory flow rate
- SABA, short acting β2 agonist
- SABD, short acting bronchodilator
- SAMA, short acting muscarinic antagonist
- Sao2, arterial oxygen saturation
- chronic obstructive pulmonary disease
- exacerbations
- management
Statistics from Altmetric.com
- COPD, chronic obstructive pulmonary disease
- CRP, C-reactive protein
- FEV1, forced expiratory volume in 1 second
- LABA, long acting inhaled β2 agonist
- LABD, long acting bronchodilator
- MDI, metered dose inhaler
- NIV, non-invasive ventilation
- PEFR, peak expiratory flow rate
- SABA, short acting β2 agonist
- SABD, short acting bronchodilator
- SAMA, short acting muscarinic antagonist
- Sao2, arterial oxygen saturation
Exacerbations of chronic obstructive pulmonary disease (COPD) have a negative effect on patients in terms of mortality,1,2 health related quality of life, and decline in lung function including huge socioeconomic costs on healthcare resources. Exacerbations commonly result in worsening of gas exchange3 and pulmonary haemodynamics,4 and are also predictive of admission to hospital. A British Thoracic Society audit5 of the hospital care of patients admitted for exacerbations of COPD revealed that 50% of them did not have a documented diagnosis of COPD, standard diagnostic investigations were often not performed, and subsequent interventions known to have a favourable influence on the outcome were not given. A study of the risk of hospital admissions for exacerbations showed a moderate to high prevalence of potentially amenable factors, suggesting that care is currently unsatisfactory.6 Unsurprisingly, the management and care of many patients with exacerbations follows a “shotgun” approach with all available treatments being used. The “domino” effect of a hospital admission for acute COPD goes beyond the emergency department and creates seasonally major disruptions in hospital management making COPD the “Cinderella” of medicine.7 Exacerbations of COPD represent one of the major contributors to the clinical load of physicians who, in addition, have access to only a limited therapeutic armamentarium.8 The poor recognition of COPD exacerbations and insufficient treatment reflects the multidisciplinary heterogeneity of the pathophysiology of exacerbations.
This paper reviews the most relevant evidence based therapeutic options currently available for the appropriate management of exacerbations of COPD. Over the last year the American Thoracic Society (ATS) and the European Respiratory Society (ERS)9 have reviewed their own guidelines, and the Global Initiative for Chronic Obstructive Lung Disease (GOLD) has released its annual update on management.10 Likewise, the continuing efforts of national respiratory societies to update their recommendations,11,12 some using robust evidence based tools,12 and some extensive reviews13,14 have to be acknowledged. The reader is encouraged to study these documents which offer a more comprehensive insight into the management of COPD exacerbations, a field that is continually evolving.15
Early recognition of exacerbations and prompt treatment ameliorate their clinical progress while improving health related quality of life and reducing the risk of hospital admission.16 By optimising patient-physician understanding of the nature of exacerbations of COPD and the effects of early treatment, the negative influence of the current morbidity and mortality of exacerbations will be minimised.
DIAGNOSTIC ASSESSMENT AND PATHOPHYSIOLOGY
Irrespective of the definition of exacerbation used,17 the clinical diagnosis points to an acute clinical worsening that may necessitate a change in regular treatment.18,19 However, since there is no objective confirmation of the diagnosis of COPD in 50% of patients,5 one common problem is to know whether the patient has underlying COPD. A typical history of smoking and the presence of cough, sputum, and breathlessness with reduction in breath sounds and wheezing are the usual pointers to a diagnosis of COPD.20
A stepwise approach with four components forms the diagnostic assessment. The first step is an appropriate medical history which identifies one or more of the three cardinal symptoms: increased shortness of breath, increased sputum volume, and increased sputum purulence. These symptoms have to be interpreted in the context of other clinical conditions such as disease severity, frequency of previous acute episodes, the presence of co-morbidities (cardiovascular, diabetes, skeletal muscle), and the socioeconomic environment. The second step is a physical examination to identify the principal respiratory signs (rapid and shallow breathing, use of accessory respiratory muscles, paradoxical chest wall motion, wheezing, attenuated or absent breath sounds, hyperresonance on percussion, purse lip breathing), cardiovascular signs (increased and/or abnormal pulse heart rate, right heart failure, peripheral oedema, haemodynamic instability), and general signs (altered mental status, central cyanosis). The third step involves the recognition of clinical conditions that are often associated with COPD—for example, pulmonary conditions (pneumonia, pneumothorax, pleural effusion, lung cancer, upper airway obstruction, rib fracture), cardiovascular conditions (pulmonary embolism, right/left heart failure), and drug related causes (sedatives, narcotics). All the latter are considered complications that easily mimic exacerbations.18,21 The fourth step includes several standard diagnostic procedures such as arterial blood gas analysis, chest radiography, routine blood tests, ECG, and Gram stain and culture when sputum is purulent. The use of pulse oximetry alone to measure arterial oxygen saturation (Sao2) is only recommended for mild exacerbations. Forced spirometry is of limited usefulness for the management of exacerbations22 but is mandatory during the recovery or follow up period to confirm the diagnosis of COPD or to monitor further slow improvement. Peak expiratory flow rate (PEFR), used as an alternative measurement of airflow limitation,23 correlates well with forced expiratory volume in 1 second (FEV1),24 although the clinical implications of this correlation remain unclear.22
Pathologically, exacerbations of COPD are characterised by enhanced airway inflammation and oedema25–,27 and systemic inflammation,25,28 resulting in more airflow limitation and gas exchange defects due to further lung mechanical abnormalities and ventilation-perfusion worsening, along with increased oxygen consumption, altered hypoxic vasoconstriction, and systemic (increased cardiac output) and pulmonary (increased pulmonary artery pressure) haemodynamic abnormalities.3,29a,29b Interestingly, each of these pathophysiological factors that govern gas exchange can be modulated, at least in part, by the currently available pharmacological and non-pharmacological treatments available (fig 1⇓).3,30

Effect of currently available pharmacological and non-pharmacological options on the papthophysiological factors that govern gas exchange. +, beneficial effect; −, detrimental effect; ±, beneficial-detrimental effects. Reproduced from Rodriguez-Roisin et al30 with permission from Prous Science.
PHARMACOLOGICAL TREATMENT: THE “ABC APPROACH”
This can be called the “ABC approach”, an acronym that reflects the three classes of drugs (antibiotics, bronchodilators and corticosteroids) commonly used for exacerbations of COPD (table 1⇓). However, if we consider only the highest levels of evidence,10 this is only valid for bronchodilators and systemic steroids (see table S1 available online only at http://www.thoraxjnl.com/supplemental).
What is known of pharmacological treatment
Bronchodilators
Inhaled bronchodilators
Short acting inhaled β2 agonists and anticholinergic agents remain the main treatment modality for exacerbations as they reduce symptoms and improve airflow obstruction. Short acting β2 agonists (SABAs) such as salbutamol and terbutaline act by increasing the concentration of cyclic adenosine monophosphate (cAMP),31 while anticholinergics such as ipratropium and oxitropium bromide are non-selective muscarinic antagonists (SAMAs).32,33 Although there are no trials of short acting bronchodilator (SABD) agents, their use in the treatment of exacerbations has not been questioned.33,34 There are three relevant issues related to the use of SABDs during exacerbations: efficacy of the drugs, drug combinations, and the delivery system for inhaled treatment (table 1⇑).12
There is no evidence of a difference between classes of SABDs in terms of bronchodilatation (increased FEV1 range 150–250 ml) at 90 minutes.35–,37 When inhaled, the effects of SABAs begin within 5 minutes with maximum peaks at 30 minutes; ipratropium begins to take effect after 10–15 minutes with a peak at 30–60 minutes. The effects of the two classes of SABDs decline after 2–3 hours and can last as long as 4–6 hours, depending on their individual properties.14 Compared with a 54 μg ipratropium bromide metered dose inhaler (MDI), a 1.95 mg MDI of metaproterenol sulfate decreased arterial oxygen tension (Pao2) by 0.8 kPa (6 mm Hg) at 20 minutes with minor clinical and functional consequences.35 Similarly, a 200 μg oxitropium bromide MDI did not induce oxygen desaturation at 30 minutes in a randomised controlled trial (RCT) in outpatients.38 Inspiratory capacity also increased significantly at 30 and 90 minutes after nebulised salbutamol 5.0 mg (approximately by 10% each) in inpatients,39 suggesting a complementary benefit on acute-on-chronic air trapping and lung hyperinflation,40,41 a finding with added value in lung function assessment.
By contrast, the efficacy of combinations of SABDs remains unsettled. Unlike stable COPD where the simultaneous concurrent administration of SABDs is more efficacious than either agent given alone,42 a combination of SABDs given sequentially in exacerbations does not provide additional benefit.35,43,44
A systematic review of the route of delivery of SABDs found no significant differences in FEV1 between the use of hand held MDIs with a good inhaler technique (with or without a spacer device) and nebulisers.45 A nebuliser with a mouthpiece to avoid nasal deposition or a face mask to avoid ocular side effects with SAMAs is more convenient for sicker patients who usually need admission to hospital and may be more beneficial due to their individual physical properties. However, its effects on mucus viscosity are unknown. As a rule of thumb, an MDI is more convenient for low doses of SABDs.
Increasing the dose and/or the frequency of existing SABD treatment with SABAs is the strategy recommended by the ATS/ERS9 and GOLD10 guidelines. The addition of a SAMA if the clinical response is not immediately favourable is also recommended, despite the uncertainties about combinations of SABDs in this setting.10 The ATS/ERS guidelines9 and NICE report12 recommend the use of SABAs and/or SAMAs. It is most likely, however, that the correct strategy for the physician remains, at least in part, empirical.
Formoterol, a rapid onset long acting inhaled β2 agonist (LABA), previously used as an as-needed reliever in both stable and acute asthma46 and in exacerbations of COPD without major adverse effects,47 has also been proposed in a cumulative manner for the management of exacerbations.48 Despite the fact that high doses of formoterol are well tolerated, it remains uncertain whether this dosage and agent can be used as an alternative to SABDs during exacerbations.49 Compared with placebo, the LABA salmeterol given via an MDI or dry powdered 50 μg twice daily had a similar cardiovascular safety profile in stable COPD.50
There is accumulating evidence that SABAs may increase the risk of adverse cardiovascular events in patients with obstructive airway disease, a finding of special concern for those patients with underlying cardiovascular co-morbidities.51 However, neither SABAs in any form nor at first time use increased the risk of acute myocardial infarction in a cohort of more than 10 000 patients newly diagnosed with COPD, with and without pre-existing concomitant cardiovascular disease.52 Troublesome muscular tremor, hypokalaemia, and increased oxygen consumption also occur. Subclinical mild deterioration in gas exchange within 30–90 minutes of nebulisation with further hypoxaemia and/or increased alveolar-to-arterial oxygen difference and moderately increased cardiac output are frequent events.39 The main adverse effect of SAMAs is mouth dryness, sometimes associated with a bitter taste and occasional prostatic symptoms.
The ATS/ERS guidelines9 recommend adding long acting bronchodilators (LABDs) and inhaled steroids as an adjunct to the treatment if patients were not using them, although there is no evidence for such a recommendation. Currently, the maintenance or addition of salmeterol during an exacerbation needs to be considered on an individual basis since, when taken in the recommended dosage, it can result in a small but significant decline in Sao2 in stable COPD.53 It is unknown whether there are additive side effects when LABAs are used in combination with high doses of SABAs. Alternatively, some of the non-bronchodilator effects of LABAs31—such as inhibition of inflammatory mediator release, stimulation of mucociliary transport, and attenuation of neutrophil recruitment and activation—could be beneficial for some of the pathobiological aspects of exacerbations. The recent observation of significant lung hyperinflation in patients with acute COPD40,41 may be important as LABDs reduce hyperinflation at rest54 and during exercise.55–,57 There is also emerging evidence that a combination of a LABA and tiotropium bromide may have complementary effects.48,58 Furthermore, there is some evidence that tiotropium bromide may have some anti-inflammatory effects.49,59,60
Methylxanthines (theophylline)
Theophylline has been relegated to second line intravenous treatment for the management of exacerbations in patients with an inadequate or insufficient response to SABDs.61 Compared with placebo, most studies with intravenous theophylline have shown marginal effects on symptoms, hospital admission rate, acid-base balance, and lung function (FEV1 and arterial blood gases) in non-acidotic patients.62,63 When used in the clinical setting, physicians have to be aware of its many unwanted effects and interactions with other metabolic factors.
Despite its bronchodilating effects through directly relaxing human airways smooth muscle cells possibly by phosphodiesterase inhibition, there is increasing evidence of anti-inflammatory effects at low serum concentrations.49 The recent finding that theophylline activates histone deacetylases—nuclear enzymes involved in the switching off of activated inflammatory genes—is of further pathogenic and therapeutic interest.64–,66
Systemic corticosteroids
The role of systemic corticosteroids in treating patients with exacerbations has remained contentious for almost 20 years. Since the original study in which significant improvements in pre and post bronchodilator FEV1 values were seen in hospital inpatients with exacerbations treated with intravenous methylprednisolone (0.5 mg/kg four times daily for 3 days) compared with placebo,67 five relevant RCTs in outpatients and inpatients with moderate to severe exacerbations of COPD68–,72 and three systematic reviews34,73,74 have led conclusively to the evidence based systemic use of corticosteroids for exacerbations of COPD (table 1⇑).
Two studies were carried out in outpatients. In the first,68 patients presenting with non-acidotic exacerbations were randomised to a 9 day course of either oral prednisone in a tapering dose (starting with 60 mg once daily for 3 days) or placebo. Compared with the placebo group, there was a more rapid improvement in FEV1 (by 18% and 37%) and in moderate hypoxaemia (by 23% and 26%) on days 3 and 10 compared with day 1 in the treatment group. The most important finding was that treatment failure was significantly more frequent in the placebo group. In the second study69 40 mg oral prednisone or placebo was given once daily for 10 days to a cohort of patients with severe exacerbations of COPD after discharge from an emergency department. Compared with placebo, the active treatment significantly reduced the overall relapse rate at 30 days (27% versus 43%), suggesting that for every six patients treated with steroids, one relapse in 30 days was avoided. Compared with placebo, post bronchodilator FEV1 improved (34% (300 ml) v 15% (160 ml) from baseline) and breathlessness improved significantly after prednisone without differences in hospital admission rates or mortality. The steroid group was, however, more likely to have insomnia, increased appetite, and weight gain with trends toward a higher incidence of depression and anxiety.
In the largest inpatient study of COPD exacerbations to date,70 patients received either 125 mg intravenous methylprednisolone four times daily for 3 days followed by 8 or 2 weeks of a tapering dose of oral prednisone (starting with 60 mg once daily), while the third group received placebo. Compared with placebo, the treatment failure rate was significantly less in the combined steroid group on days 30 (33% v 23%) and 90 (48% v 37%) but not at 6 months. The length of hospital stay was shortened by 1 day and FEV1 improved more rapidly in the steroid group (by approximately 100 ml) from day 1 but did not differ by 2 weeks. Adverse events were, however, more noticeable in the steroid treated group (67% patients had diabetes), including hyperglycaemia requiring treatment (15%) and a higher proportion of secondary infection in the group treated for 8 weeks. The duration of steroid treatment did not influence these outcomes.
In another study71 patients with severe COPD admitted to hospital for a non-acidotic exacerbation were assigned to oral prednisolone (30 mg once daily) or placebo for 2 weeks. Changes in post bronchodilator FEV1 were greater after steroids with increases of 90 ml daily up to day 5 of hospital stay and earlier plateaus compared with the placebo group. At discharge, pre bronchodilator and post bronchodilator FEV1 values rose significantly in the corticosteroid group (from 27% to 38% and from 28% to 42%, respectively), with no differences at 6 weeks. The spirometric changes were matched by improvements in symptoms during admission in the two groups, the greatest changes being seen in sleep quality, shortness of breath, mobility, and general well being. The median length of hospital stay was reduced by 2 days in the corticosteroid group. There was no difference in exacerbation or re-admission rates or in the treatment received between the two intervention groups. Transient glycosuria was the major adverse event observed in the active treatment group.
The third RCT in inpatients72 compared nebulised budesonide 0.5 mg/ml (2 mg four times daily for 3 days followed by 2 mg per day for 7 days) with oral prednisolone (30 mg twice daily for 3 days followed by 40 mg once daily for 7 days) and with placebo in patients with severe COPD hospitalised for moderate to severe non-acidotic exacerbations. Compared with the placebo group, post bronchodilator changes in FEV1 within the first 3 days of treatment were more rapid in both active treated groups (budesonide by 100 ml, prednisolone by 160 ml, no difference between them) but these had abated at 2 weeks. Pre bronchodilator FEV1 was higher in both active treatment groups than in the placebo group, but only significantly so (by 120 ml) in those who received prednisolone. Dyspnoea fell substantially in all the three groups, and there were small but significant increases in Pao2 in the prednisolone group together with a small decrease in arterial carbon dioxide tension (Paco2) which was significant in both active groups. Length of hospital stay and corticosteroid related adverse events were similar in the three groups, with disease deterioration as the most serious event in those receiving prednisolone. Hyperglycaemia was more common in the steroid group than in the other three subsets.
In another inpatient study75 no differences were seen between intravenous and oral steroid treatment and between aerosol and MDI SABD treatment of exacerbations and, in another study,76 patients with frequent severe exacerbations needing hospital admission showed greater improvements in pre bronchodilator FEV1 and Pao2 and in dyspnoea on exertion after a 10 day course of intravenous methylprednisolone than after a 3 day course.
The mechanisms for improving lung function and other outcomes and the patients most likely to benefit from steroid treatment during exacerbations remain contentious. No clinical, biochemical, or functional markers can clearly identify which patients will respond better to steroid treatment. Although no effects on airway cytokines have been found in patients with stable COPD,77 two studies have reported reductions in airway eosinophilic inflammatory markers78 and in serum C-reactive protein (CRP) after 2 weeks of treatment with oral steroids.27 The beneficial response to steroids during exacerbations suggests that enhanced airway inflammation and oedema25–,27 and systemic inflammation25,28 are reduced, or that the inflammatory pattern is sensitive to corticosteroids.49 An increased number of eosinophils has been found in patients with mild to moderate COPD exacerbations.79 Treatment with oral steroids for 10–14 days in an outpatient setting reduced some markers of sputum neutrophilic inflammation such as the chemoattractants interleukin-8 and tumour necrosis factor-α during the recovery phase, and these increased at the nadir of the exacerbation.25,80 In inpatients with exacerbations, steroid use for 7 days significantly reduced serum CRP and lipopolysaccharide binding protein levels, markers of systemic inflammation.28,81
These RCTs all have some limitations in common. Only a minority of many screened patients were eventually enrolled in the studies as patients taking systemic steroids regularly during the preceding month were excluded. This suggests that regular systemic steroid therapy is common, particularly among those with the most severe and unstable clinical profile who, in turn, may exhibit more frequent acute episodes. In addition, very few patients were receiving regular LABDs and/or fixed combination inhalers, hence ignoring the complementary effects of these agents as an adjunct therapy in exacerbations. A subgroup analysis suggested that the benefits of steroid treatment were associated with a more favourable outcome in patients with previous exacerbations who needed admission to hospital.70 It is possible that the response of these patients may be greater following repeat treatment with steroids than in those who had not previously received systemic treatment. Adverse events are not sufficiently known, particularly in the medium and long term—a serious drawback given the high prevalence of co-morbidities in most of these elderly patients. Although the optimum duration and dosage of steroid treatment has not been established, a starting dose of 30–40 mg/day and treatment duration of 7 days have been consistently recommended.
Antibiotics
The use of antibiotics in exacerbations of COPD remains unsettled despite their extensive use. It is unlikely that the majority of patients will benefit from a short course of antibiotics during exacerbations (table 1⇑). The most frequent aetiology of an exacerbation is infection of the lower airways and/or air pollution, even though the cause of one third of exacerbations is still ignored.82 Patients with COPD have bacteria in high concentrations in their lower airways during both exacerbations and stable conditions (airway colonisation).83,84 This concept of the causative role of bacterial microorganisms has been reinforced by the isolation of new strains of a bacterial pathogen with development of specific immune responses.85,86 The predominant bacterial microorganisms recovered from the airways of patients with mild exacerbations are Haemophilus influenzae, Streptococcus pneumoniae and Moraxella catarrhalis83 while, in patients with severe COPD episodes, enteric Gram negative bacilli and Pseudomonas aeruginosa may be more important.84 Viral infections (picornaviruses, influenza A and respiratory syncytial virus) are likely to play a part in severe exacerbations.87,88
A seminal study by Anthonisen et al89 provided strong evidence that antibiotics have a significant effect on PEFR and lead to an earlier resolution of all three of the cardinal symptoms defining exacerbations (increased dyspnoea, increased sputum volume, and increased sputum purulence). Stockley et al90 showed a relationship between sputum purulence and the presence of bacteria, suggesting that these patients should be treated with antibiotics if they also have at least one of the other two symptoms (dyspnoea or increased sputum volume). Of the three systematic reviews of the use of antibiotic treatment in the presence of purulent sputum,34,91,92 the most recent 92 observed a reduction in the risk of mortality, treatment failure, and sputum purulence. However, these results need to be viewed with some caution, given the difference in patient selection, antibiotic choice, small number of trials, and lack of control for other therapeutic interventions that influence outcome. Compared with placebo, patients with exacerbations mechanically ventilated and treated with an oral antibiotic (ofloxacin) had reduced mortality, needed fewer additional antibiotics, and had a shorter duration of ventilator treatment and length of hospital stay.93
According to GOLD recommendations,10 antibiotics should be given to patients with exacerbations with the three major symptoms,89 to those with two symptoms provided increased sputum purulence is present, and to those who are critically ill and needing mechanical support. The oral route is preferred and is cheaper.10 Their administration should be based on the patterns of local bacterial resistance9 and their use should be maintained for a period of 3–10 days (table 2⇓).10 If an exacerbation responds poorly to empirical antibiotic treatment, the patient should be re-evaluated for complications with microbiological reassessment if necessary.
Antibiotic treatment in exacerbations (taken from GOLD10)
Respiratory stimulants
In the 1970s and 1980s both doxapram94 and almitrine bismesylate10,95 were in their heydays and were the two most recommended drugs for treating chronic and acute hypercapnic respiratory failure in patients with COPD. However, almitrine, a relatively specific peripheral chemoreceptor, was associated with serious adverse effects (peripheral neuropathy and weight loss) in stable COPD without significant effects on mortality or quality of life. Serious flaws in the design of the RCTs together with the robustness of evidence based effects of non-invasive ventilation (NIV) in patients with acute COPD have relegated the use of doxapram to those very unusual clinical situations in which NIV is not available or not indicated.12
Adjunct therapies
An appropriate fluid balance with special attention to the administration of diuretics,13 nutritional aspects, anticoagulants, and cardiovascular agents are the most complementary standard measures.10 At any time, physicians will strongly enforce stringent measures against active cigarette smoking.
NON-PHARMACOLOGICAL TREATMENT
Two major non-pharmacological approaches—namely, oxygen therapy and ventilatory support—are widely used in the most severe exacerbations of COPD.96–,99 These approaches are now complemented by the use of structured management programmes described as “hospital at home” (HaH)100,101 and pulmonary rehabilitation introduced in the recovery period after hospitalisation.102
A clinical condition characterised by decreased Pao2 with or without increased Paco2 can be a practical definition for acute (or acute-on-chronic) respiratory failure during an exacerbation of COPD. It occurs when the respiratory system cannot cope with adequate alveolar ventilation to pulmonary blood flow balance in the presence of severely abnormal lung mechanics. Both arterial hypoxaemia and hypercapnia are dominated in part by further ventilation-perfusion imbalance.3,29a Hypercapnia is, however, also greatly influenced by lung mechanical abnormalities due to the limitations of the respiratory pump in maintaining effective alveolar ventilation.29a Both increased airways obstruction and lung hyperinflation40,41,103 superimpose an excessive elastic and resistive load on the respiratory pump so that the respiratory muscles are overburdened and operate at a mechanical disadvantage.103,104 Moreover, there is an inspiratory threshold load due to increased inspiratory positive end expiratory pressure.29b,105 With this overload of the respiratory muscle pump, alveolar ventilation cannot be sustained effectively and hypercapnia, acidosis, and further hypoxaemia ensue. The capacity of the respiratory pump is further compromised by the detrimental effects of acidosis on the respiratory muscles106 which, in turn, results in superimposed muscle fatigue107 creating a vicious cycle that further aggravates the acid-base status and gas exchange. This is why arterial pH and blood gases are central physiological outcomes for assessing acute respiratory failure during exacerbations of COPD.
Controlled oxygen therapy
Oxygen therapy is of great beneficial value in acute respiratory failure during exacerbations. Its primary objective is to raise Pao2 to prevent life threatening hypoxaemia in order to optimise oxygen delivery to peripheral tissues and alleviate symptoms, mostly dyspnoea (table 3⇓). In clinical practice, physicians administer controlled low inspired oxygen concentrations (either 24% or 28%) through high flow (Venturi) masks at flow rates of 2–4 l/min. This strategy increases Pao2 sufficiently (1.3–2.0 kPa or 10–15 mg) to maintain optimal values above 8.0 kPa (60 mm Hg) and to ensure adequate Sao2 levels (⩾90%) without risking detrimental carbon dioxide retention and acidosis. Low flow devices such as nasal prongs or cannulae are less accurate as they deliver a variable and higher inspired oxygen concentration which can result in suppression of respiratory drive, carbon dioxide narcosis, and eventually respiratory arrest108 if the patient is not appropriately monitored. Although these concepts are clearly established, well designed trials in this field are lacking.109 Ideally, arterial blood gas analysis from radial stabs (or from another peripheral artery) provides the most accurate assessment. Ear lobe gases are of more limited use as they accurately reflect Paco2 only.110,111 Pulse oximetry is a non-invasive alternative which is useful for trending and/or adjusting oxygen therapy settings. The optimal strategy for oxygen therapy during exacerbations is shown in fig S1 available online only at http://www.thoraxjnl.com/supplemental. During moderate to severe exacerbations, arterial pH and blood gas tensions should always be measured before and 1 hour after starting oxygen therapy.
What is known of non-pharmacological treatment
When 100% oxygen is breathed in clinical practice during invasive ventilation only, there is a further ventilation-perfusion mismatch which indicates the release of hypoxic pulmonary vasoconstriction without development of reabsorption atelectasis (that is, increased intrapulmonary shunt).112 The administration of 100% oxygen, either by spontaneous breathing or via ventilatory support, results in further hypercapnia mainly attributed to increased dead space.112–,114
Assisted mechanical support
The primary therapeutic goal of ventilatory support in patients with exacerbations with acute respiratory failure is to decrease both mortality and morbidity and to relieve symptoms, despite optimal medical treatment.9,10,12 Mechanical ventilation can be delivered non-invasively or invasively (conventionally) using different modes that are, in essence, positive pressure devices (negative ventilation is currently not recommended) for non-invasive ventilation using either a nasal or facial mask, or via an endotracheal tube or a tracheostomy for invasive ventilation.
When assessing the suitability of patients with advanced COPD for mechanical ventilation, many factors must be taken into account including the patient’s age, disease severity, co-morbidities, prior functional status, and experience during previous exacerbations, especially where ventilatory support has been required. Patients with end stage COPD with at least one hospital admission for hypercapnic respiratory failure have a worse health status and emotional well being than patients with unresectable non-small cell lung cancer and receive less holistic care appropriate to their needs.115 These findings are even more important if we consider that the quality of the patient-physician communication regarding end of life care from the patient’s perspective—such as talking about the prognosis, dying and spirituality—is rated poorly by oxygen dependent patients with advanced COPD.116 Patients with severe exacerbations requiring ventilatory support may find the treatment more burdensome than the benefit in terms of prolonged life that it offers, and there are no predictive features to identify this. In principle, autonomy of the patient should be the key ethical principle to guide physicians, patients, and relatives in choosing the most suitable end of life decision making process.9,10
Non-invasive ventilation (NIV)
This treatment is now widely used in acidotic hypercapnic exacerbations of COPD. The criteria to identify patients who will benefit are straightforward and are shown in table 3⇑ (see also table S2 and fig S1 available online only at http://www.thoraxjnl.com/supplemental). It can be delivered using air, with or without mixed oxygen. The improvement in gas exchange and acid-base effects by NIV reflects improved alveolar ventilation which results from a change in breathing pattern to a slower, deeper, more physiological pattern with no change in the underlying ventilation-perfusion imbalance.117,118 A systematic review119 based on several RCTs120–,126 provided evidence that NIV—as an adjunct to standard medical care—decreased mortality, the need for endotracheal intubation (for every five patients treated with NIV one patient would avoid intubation), and treatment failure. Moreover, NIV increased pH, reduced hypercapnia and the respiratory rate within 1 hour of its institution, shortened the length of hospital stay by more than 3 days irrespective of environment (high dependency/intensive care unit versus medical ward), and decreased complications associated with treatment. NIV is cost effective compared with usual therapeutic care alone.127,128 The current recommendation is to deliver NIV in a controlled environment with a dedicated setting led by experienced and well trained personnel.9,10,12
Invasive ventilation
The most life threatening episodes of acute respiratory failure exacerbations can benefit from the use of invasive ventilation (see table 3⇑ and table S2 and fig S1 available in the online supplement at http://www.thoraxjnl.com/supplemental). Despite the need for invasive ventilation, relatively good survival is achieved with mortality rates of 11–49%.1,97,99 These figures are, however, considerably lower than those observed in patients with respiratory failure from other aetiologies treated in general intensive care settings.129 Compared with acute respiratory distress syndrome (ARDS), the mean duration of ventilation in acute COPD was significantly shorter (9 v 5 days)129 or even lower (median 2 days), as was the length of stay in the intensive care unit (1 v 25 days).99
NIV has been used to shorten the period of invasive ventilation in cases of weaning failure and in those with a long stay in the intensive care unit.130,131 However, a large scale RCT in unselected patients needing mechanical ventilation found that NIV was not effective in avoiding the need for re-intubation and did not reduce mortality.132
Pulmonary rehabilitation (physiotherapy)
Pulmonary rehabilitation is a multidisciplinary programme particularly suited for all patients with COPD except those with stable stage I disease.9,10,13,133 However, other than manual chest percussion10 and physiotherapy using positive expiratory pressure masks for selected patients12 to help in clearing sputum, pulmonary rehabilitation has no indication in exacerbations of COPD. It can, however, have an adjunct therapeutic role in exacerbations. One study showed that a comprehensive home care intervention, which included a simple pulmonary rehabilitation programme together with standardised pharmacological treatment delivered by specialised nurses in selected non-acidotic patients with exacerbations admitted to emergency departments, could be used to treat exacerbations at home safely.100 An 8 week course of pulmonary rehabilitation using a multifaceted programme instituted shortly after admission to hospital for an exacerbation resulted in substantial improvements in exercise capacity and health related quality of life at 3 months.102
HOSPITAL AT HOME (HAH) AND SUPPORTED DISCHARGE SERVICES
HaH services represent a new healthcare model which are potentially appealing for the management of selected non-acidotic patients with exacerbations of COPD presenting to emergency departments.100 At first glance, patients with altered mental status or confusion, acute ECG or radiographic changes, serious co-morbidities, and/or poor social conditions should not be eligible for these healthcare schemes. There are three objectives for these patients to be safely cared for at home: (1) immediate or early discharge from the hospital to avoid or shorten length of hospital stay; (2) provision of a tailored individualised management programme; and (3) home support by a skilled specialised respiratory team. The major finding of the most recent meta-analysis101 including several robust RCTs134–,140 concluded that HaH services could be used as safely as hospital care. Compared with inpatient care, patients assigned to HaH generated substantial financial savings, mostly due to a shorter hospital stay.
CONCLUSIONS
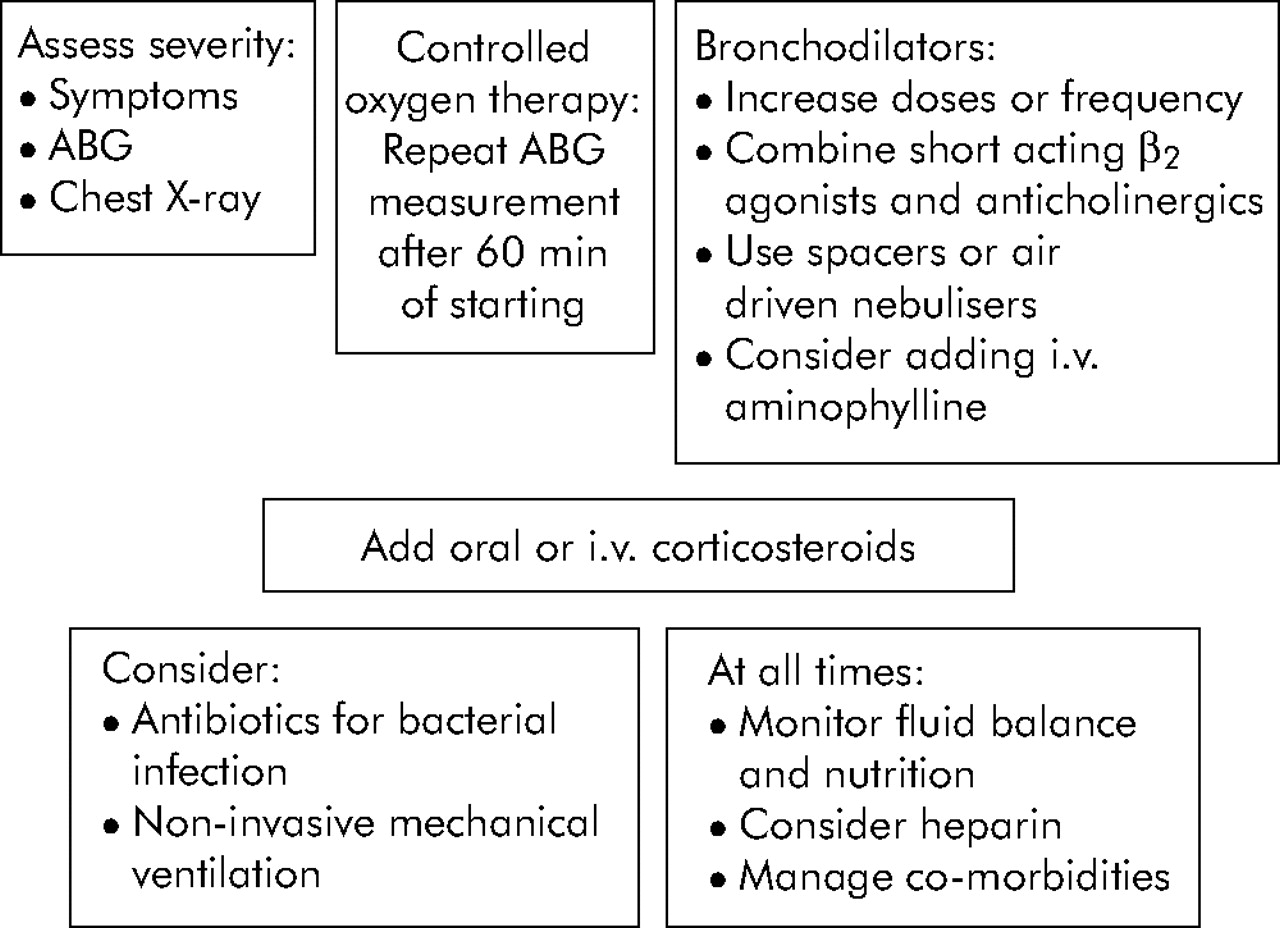
Exacerbations can be managed at home or in hospital, depending on factors and aspects considered in the diagnostic assessment (see table S3 available online only at http://www.thoraxjnl.com.supplemental). Nevertheless, with the exception of ventilatory support, most of the therapeutic approaches discussed are available at home and can be used safely. Accordingly, HaH and supported discharge programmes are likely to become more common and extensively applied in the future. Management schemes for patients with mild to moderate exacerbations and for those with moderate to severe exacerbations30 are shown in figs 2⇓ and 3⇓, respectively, and are dealt with in greater detail by GOLD10 and the ATS/ERS guidelines;9 both are based essentially on the clinical presentation of the patient. However, grading of the severity of mild to moderate exacerbations remains contentious19 since they can be categorised either on clinical presentation (essentially symptoms)89 or healthcare use resources.18 Detailed discharge from hospital and general follow up measures will be actively reinforced after exacerbations.9,10

Management scheme for patients with mild to moderate exacerbations of COPD. Reproduced from Rodriguez-Roisin et al30 with permission from Prous Science.

{kind=link}
{kind=link}
{kind=link}
Management scheme for patients with moderate to severe exacerbations of COPD. ABG, arterial blood gases. Reproduced from Rodriguez-Roisin et al30 with permission from Prous Science.
Acknowledgments
The author thanks Laura Morte for her secretarial support. Figures 1⇑, 2⇑ and 3⇑ are reproduced from Rodriguez-Roisin et al30 with permission from Prous Science.
REFERENCES
- 1.↵
- 2.↵
- 3.↵
- 4.↵
- 5.↵
- 6.↵
- 7.↵
- 8.↵
- 9.↵
- 10.↵
- 11.↵
- 12.↵
- 13.↵
- 14.↵
- 15.↵
- 16.↵
- 17.↵
- 18.↵
- 19.↵
- 20.↵
- 21.↵
- 22.↵
- 23.↵
- 24.↵
- 25.↵
- 26.
- 27.↵
- 28.↵
- 29a.↵
- 29b.↵
- 30.↵
- 31.↵
- 32.↵
- 33.↵
- 34.↵
- 35.↵
- 36.
- 37.↵
- 38.↵
- 39.↵
- 40.↵
- 41.↵
- 42.↵
- 43.↵
- 44.↵
- 45.↵
- 46.↵
- 47.↵
- 48.↵
- 49.↵
- 50.↵
- 51.↵
- 52.↵
- 53.↵
- 54.↵
- 55.↵
- 56.
- 57.↵
- 58.↵
- 59.↵
- 60.↵
- 61.↵
- 62.↵
- 63.↵
- 64.↵
- 65.
- 66.↵
- 67.↵
- 68.↵
- 69.↵
- 70.↵
- 71.↵
- 72.↵
- 73.↵
- 74.↵
- 75.↵
- 76.↵
- 77.↵
- 78.↵
- 79.↵
- 80.↵
- 81.↵
- 82.↵
- 83.↵
- 84.↵
- 85.↵
- 86.↵
- 87.↵
- 88.↵
- 89.↵
- 90.↵
- 91.↵
- 92.↵
- 93.↵
- 94.↵
- 95.↵
- 96.↵
- 97.↵
- 98.
- 99.↵
- 100.↵
- 101.↵
- 102.↵
- 103.↵
- 104.↵
- 105.↵
- 106.↵
- 107.↵
- 108.↵
- 109.↵
- 110.↵
- 111.↵
- 112.↵
- 113.
- 114.↵
- 115.↵
- 116.↵
- 117.↵
- 118.↵
- 119.↵
- 120.↵
- 121.
- 122.
- 123.
- 124.
- 125.
- 126.↵
- 127.↵
- 128.↵
- 129.↵
- 130.↵
- 131.↵
- 132.↵
- 133.↵
- 134.↵
- 135.
- 136.
- 137.
- 138.
- 139.
- 140.↵
Supplementary materials
Files in this Data Supplement:
- view PDF - Supplemental tables 1-3 and supplemental figure 1.
Footnotes
Supported by the Red Respira-ISCIII-RTIC-03/11 and the Comissionat per a Universitats i Recerca de la Generalitat de Catalunya (2005 SGR-00822). Dr R R-R holds a career scientist award (2001-07) from the Generalitat de Catalunya.
Competing interests: The author has participated as a lecturer and speaker in scientific meetings and courses under the sponsorship of Almirall, AstraZeneca, Boehringer Ingelheim, GlaxoSmithKline, Laboratorios Dr Esteve SA and Pfizer; consulted with several pharmaceutical companies with relevance to the topics discussed in the present article (Almirall, Altana, AstraZeneca, Aventis, Boehringer Ingelheim, GlaxoSmithKline, Laboratorios Dr Esteve SA, Novartis, Pfizer, Viechi and Zambon); serves on advisory boards for Almirall, Boehringer Ingelheim, GlaxoSmithKline, Novartis, Pfizer, Procter & Gamble and Viechi; has been sponsored for several clinical trials; and has received laboratory research support from AstraZeneca, Boehringer Ingelheim, GlaxoSmithKline, Laboratorios Dr Esteve SA, Pfizer and Procter & Gamble Ltd.