Article Text

Abstract
Background: Oxidative stress is thought to have a major role in the pathogenesis of airway obstruction. A study was undertaken to determine whether subjects with low levels of antioxidants (serum β-carotene, α-carotene, vitamins A and E) would be at a higher risk of accelerated decline in forced expiratory volume in 1 second (FEV1) as their lungs would be less protected against oxidative stress.
Methods: 1194 French subjects aged 20–44 years were examined in 1992 as part of the European Community Respiratory Health Survey (ECRHS); 864 were followed up in 2000 and 535 (50% men, 40% lifelong non-smokers) had complete data for analysis.
Results: During the 8 year study period the mean annual decrease in FEV1 (adjusted for sex, centre, baseline FEV1, age, smoking, body mass index and low density lipoprotein cholesterol) was 29.8 ml/year. The rate of decrease was lower for the subjects in tertile I of β-carotene at baseline than for those in the two other tertiles (−36.5 v −27.6 ml/year; p = 0.004). An increase in β-carotene between the two surveys was associated with a slower decline in FEV1. No association was observed between α-carotene, vitamin A, or vitamin E and FEV1 decline. However, being a heavy smoker (⩾20 cigarettes/day) in combination with a low level of β-carotene or vitamin E was associated with the steepest decline in FEV1 (−52.5 ml/year, p = 0.0002 and −50.1 ml/year, p = 0.010, respectively).
Conclusions: These results strongly suggest that β-carotene protects against the decline in FEV1 over an 8 year period in the general population, and that β-carotene and vitamin E are protective in heavy smokers.
- BMI, body mass index
- FEV1, forced expiratory volume in 1 second
- FVC, forced vital capacity
- LDL, low density lipoprotein
- carotenoids
- antioxidants
- lung function decline
- epidemiology
Statistics from Altmetric.com
- BMI, body mass index
- FEV1, forced expiratory volume in 1 second
- FVC, forced vital capacity
- LDL, low density lipoprotein
Impaired lung function and a rapid decline in lung function are strong predictors of respiratory morbidity and mortality and of all cause and cardiovascular mortality in the general population.1,2 Oxidative stress—that is, oxidants in excess compared with the antioxidant capacity—is thought to impair lung function and to accelerate the decline in lung function.3 This can lead to airways obstruction and chronic obstructive pulmonary disease (COPD),3 particularly with exposure to cigarette smoke which is highly concentrated in oxidants.4
Antioxidants—either endogenous or in the diet—protect the lungs against serious damage by scavenging endogenous and exogenous oxidants. Vitamin E, a lipid soluble antioxidant, breaks the lipid peroxidation chain reaction and protects the lung against oxidative damage induced by the superoxide anion and hydroxyl radical.5 Lungs are also protected by additional lipid soluble antioxidants, the carotenoids, which directly scavenge the superoxide anion and free radicals such as peroxyl radical.6
Despite this evidence of biochemical lung protection by antioxidants, few studies have examined the relationship between serum antioxidant levels and lung function. Some large cross sectional population based studies reported that levels of β-carotene and other antioxidants were positively associated with the level of lung function.7,8,9,10,11,12 However, only a few longitudinal studies have investigated the effect of antioxidants on the decline in forced expiratory volume in 1 second (FEV1). In these longitudinal studies the levels of antioxidants were not measured in the serum but were assessed according to answers to dietary questionnaires. No association was found between carotenoids, vitamin A, or vitamin E and decline in lung function.11,13
The effect of serum antioxidant levels on the decline in FEV1 therefore remains unknown and needs to be explored. Blood samples taken in France in 1992 and 2000 as part of the international multicentre longitudinal European Community Respiratory Health Survey (ECRHS) provided the ideal opportunity to explore the relationships between lung function decline and serum levels of α-carotene, β-carotene, vitamin A, and vitamin E in a population of young adults.
METHODS
Subjects
The protocol of the multicentre longitudinal ECRHS study has been published elsewhere.14,15 For our analysis we included the 535 subjects in the Paris and Grenoble centres for whom spirometric data and serum levels of β-carotene, α-carotene, vitamin A, and vitamin E had been determined in both 1992 (ECRHS I) and 2000 (ECHRS II) (fig 1). We found no differences with regard to sex, body mass index (BMI), current asthma, chronic cough, chronic sputum, FEV1/FVC <70% or FEV1 between the baseline characteristics of the analysed subjects and those of the subjects not included in the analyses (either because they did not participate in ECHRS II or because they had missing data). Analysed subjects were slightly older (2 years on average), had finished education at a slightly older age (0.5 years on average), had less often worked in a job in which they were exposed to vapours, dust, gas or fumes (25% v 32%), and were more likely to have never been smokers and less likely to be heavy smokers (⩾20 cigarettes/day) (42% v 37% and 12% v 18%, respectively, p = 0.02). However, the number of pack years was not significantly different between included and excluded subjects.

Loss to follow up at ECRHS II (in 2000) and participation in the study.
Written informed consent was obtained from each subject before inclusion and the protocol of ECRHS was approved by the French Ethics Committee for Human Research and also by the National Committee for Data Processing and Freedom.
Lung function and antioxidant levels
Lung function was determined using a water sealed bell spirometer (Biomedin Srl, Padova, Italy) and the best of five technically acceptable blows was used for the analysis.14,15 Antioxidant levels were determined by high pressure liquid chromatography (HPLC). The coefficient of variation of the HPLC measurement was 9.8%, 12.0%, 2.4% and 2.2% for serum β-carotene, α-carotene, vitamin A, and vitamin E, respectively, which is comparable to that found in the study by Grievink et al.7 Non-fasting total serum cholesterol and low density lipoprotein (LDL) cholesterol levels were determined by standard methods.
Statistical analysis
All analyses were carried out using SAS software (SAS Institute, Cary NC, USA). All p values were two sided and values less than 0.05 were considered statistically significant.
The decline in FEV1 was expressed in ml/year (value at follow up minus value at baseline divided by length of follow up). In bivariate analyses, the relationships between antioxidants were assessed by calculating Pearson’s correlation coefficient (r). The associations of both antioxidant levels and FEV1 decline with potential confounders (sex, age, smoking status, BMI and LDL cholesterol levels, coded as categorical variables) were tested using Wilcoxon or Kruskal-Wallis tests according to the number of groups compared. The results were expressed as mean values with standard deviation (SD).
Baseline antioxidant levels were used to predict the decline in FEV1. As we were interested in subjects having the lowest antioxidant levels (the lungs of these subjects may be less protected against oxidative stress and they would thus be at higher risk of accelerated FEV1 decline), we classified serum antioxidant levels into tertiles and compared subjects with antioxidant levels in the lowest tertile (tertile I) with those in the higher tertiles (tertiles II + III). The results of these comparisons were expressed as adjusted means and their 95% confidence interval (95% CIs) in the tertiles or as mean differences between the tertiles, all estimated by analysis of covariance.
The effect of changes in antioxidant levels on lung function decline was analysed by including the mean annual change in antioxidant concentration (in μmol/l/year) as a continuous variable in the model. As the preliminary analysis revealed no differences except for smoking status between subjects recruited in Paris and Grenoble, subjects from the two centres were analysed together. Nevertheless, the centre was taken into account. Confounding factors were sex and baseline values of FEV1, age, BMI, and LDL cholesterol concentration. Baseline FEV1, age, BMI, and LDL cholesterol were introduced as quantitative variables. We paid special attention to tobacco smoking, a major risk factor for FEV1 decline, which may be an effect modifier as well as a confounder. Baseline smoking status was classified into four categories: never-smokers, ex-smokers (stopped for ⩾1 year), moderate smokers (<20 cigarettes/day), and heavy smokers (⩾ 20 cigarettes/day).16 In the analyses of the interactions between antioxidant levels and smoking, we coded baseline smoking status as heavy smoking compared with any other status. Smoking between the two time points was assessed as either pack years (product of the number of packs smoked per day and the number of years of smoking) or as the change in smoking status (start or increase, retain, and stop or cut down).
RESULTS
Characteristics of the study population and associations between antioxidants
The characteristics of the study population are shown in table 1. Half the participants were male. The mean (SD) age at baseline (1992) was 36.9 (7.1) years. As expected in this population of young adults, FEV1 levels were in the normal range.
Characteristics of study participants (n = 535, 50% men)*
As expected, β-carotene and α-carotene concentrations in 1992 were positively correlated with each other (r = 0.76 at baseline, p<0.0001). The vitamin A concentration was negatively correlated with both β-carotene and α-carotene concentrations (r = −0.19, p<0.0001 and r = −0.11, p = 0.02, respectively). The vitamin E concentration was positively correlated with β-carotene and α-carotene concentrations in 1992 (r = 0.21, p<0.0001 and r = 0.20, p<0.0001, respectively). Vitamin A and vitamin E concentrations were positively correlated (r = 0.31, p<0.0001). Correlations were similar in 2000 except for vitamin E v carotenoids which were non-significant.
In 1992 men had lower β-carotene and α-carotene levels than women (0.34 (0.25) v 0.48 (0.36) μmol/l, p<0.0001 for β-carotene and 0.076 (0.081) v 0.11 (0.11) μmol/l, p<0.0001 for α-carotene) but higher levels of vitamin A (2.14 (0.49) v 1.68 (0.47) μmol/l, p<0.0001) and vitamin E (23.9 (7.8) v 22.0 (6.4) μmol/l, p = 0.01). BMI was strongly correlated with antioxidant levels: positively with α-carotene and β-carotene concentrations and negatively with vitamin A and vitamin E concentrations (all p<0.05). LDL cholesterol was positively associated with all antioxidants. Heavy smokers had lower levels of β-carotene (0.29 (0.21) v 0.42 (0.32) μmol/l, p<0.0001) and α-carotene (0.06 (0.06) v 0.10 (0.10) μmol/l, p = 0.0001) than other subjects. In 2000 we observed similar associations.
Changes between ECRHS I and ECRHS II
The mean annual decline in FEV1 was −29.8 (31.9) ml/year. Between 1992 and 2000, 81.8% of the subjects did not change their smoking habits, 7.5% (n = 40) began to smoke or increased their consumption, and 10.7% (n = 57) stopped or diminished. Almost 70% of subjects remained in the same class of BMI at both baseline and follow up (7% underweight, 47% normal, and 15% overweight or obese).
Mean levels of antioxidants increased between 1992 and 2000 (table 1). For each antioxidant, levels at baseline and follow up were highly correlated (r = 0.45–0.59, all p<0.0001).
Factors associated with lung function decline
The crude mean annual decline in FEV1 according to sex and age, smoking status, FEV1, BMI, and serum level of LDL cholesterol in 1992 are shown in table 2. The decline in FEV1 was significantly steeper in men than in women, and was positively associated with baseline FEV1, age, BMI, and LDL cholesterol levels. Socioeconomic status (age at completion of full time education), physical activity (exercise resulting in breathlessness or sweating more than once a week), and occupational exposure (having worked in a job in which there was exposure to vapours, gas, dust or fumes) were not associated with lung function decline.
Factors associated with mean annual decline in FEV1 (crude associations)
Association between lung function decline and antioxidant concentrations at baseline
After adjustment for potential confounding factors, only β-carotene concentration was associated with the decline in FEV1 and subjects in tertiles II and III had a very similar FEV1 decline (table 3). FEV1 declined significantly faster in subjects in tertile I of β-carotene concentration (−36.5 ml/year (95% CI −41.5 to −31.6)) than subjects pooled from tertiles II and III (−27.6 ml/year (95% CI −31.2 to −23.9), p = 0.004), which corresponds to a supplemental FEV1 decline of 9.0 ml/year on average (95% CI 2.9 to 15.1) for subjects in tertile I compared with subjects in tertiles II and III combined. Similar results were observed after excluding subjects with either current asthma (p = 0.024) or FEV1/FVC <70% (p = 0.06). The results did not change when baseline smoking status was replaced by the number of pack years between the two time points (FEV1 decline: −35.2 ml/year (95% CI −40.2 to −30.1) in tertile I v −26.7 ml/year (95% CI −29.9 to −23.4) in tertiles II and III combined, p = 0.007) or when the change in smoking status was added to the model (FEV1 decline: −35.3 ml/year (95% CI −41.2 to −29.3) in tertile I v −26.8 ml/year (95% CI −31.7 to −21.9) in tertiles II and III combined, p = 0.007). The interaction term between sex and tertiles of β-carotene was not significant (p = 0.28).
Mean (95% CI) adjusted* annual FEV1 decline (ml/year) in tertiles of antioxidants at baseline (ECRHS I, 1992)
When all antioxidants were included simultaneously in the same regression model, β-carotene remained significantly and independently associated with decline in lung function. The mean annual decline in FEV1 was −37.7 ml/year (95% CI −43.0 to −32.4) in tertile I v −25.2 ml/year (95% CI −29.6 to −20.8) in tertiles II and III combined (p = 0.0005).
Interaction between baseline low levels of antioxidants and heavy smoking
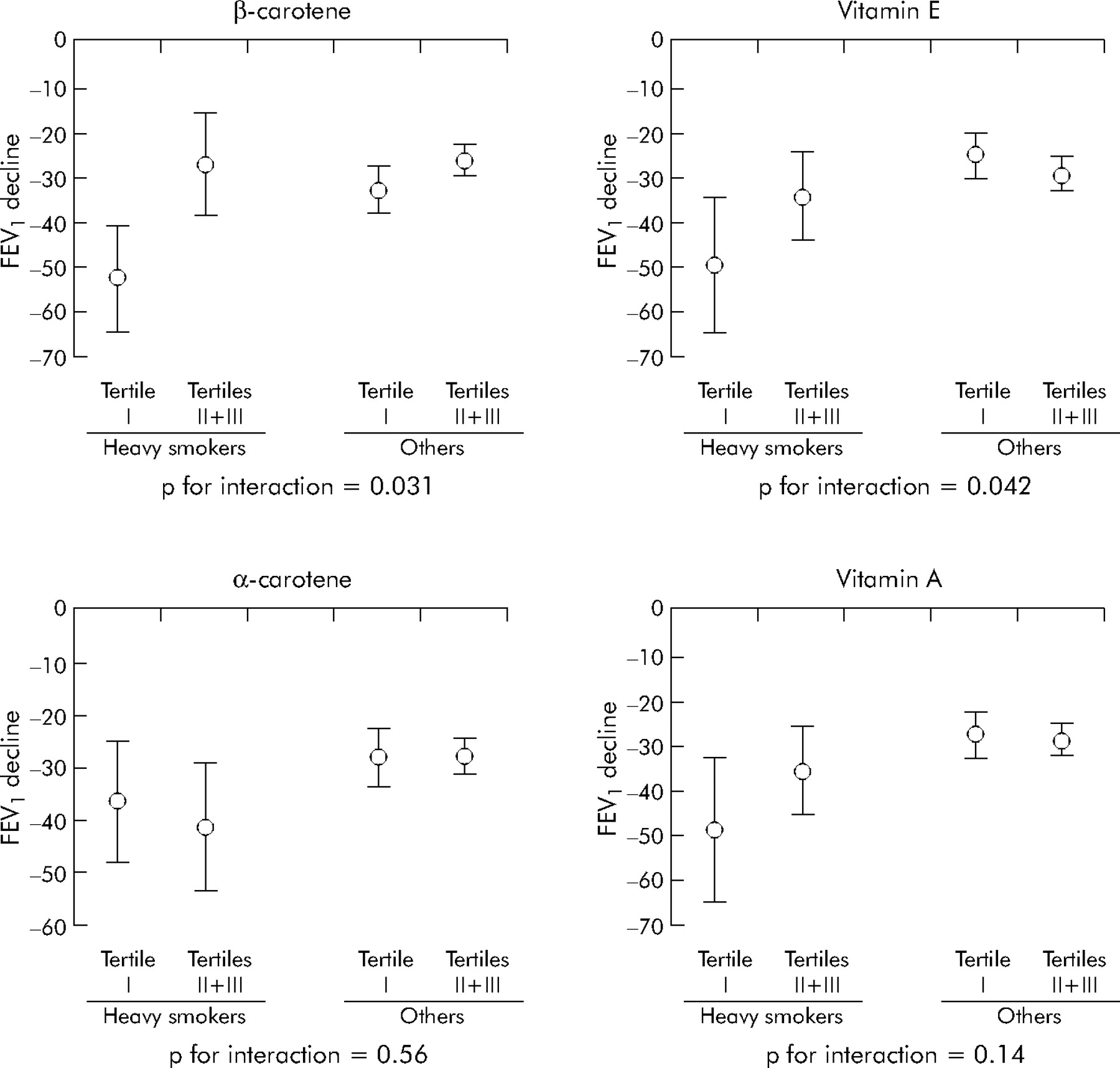
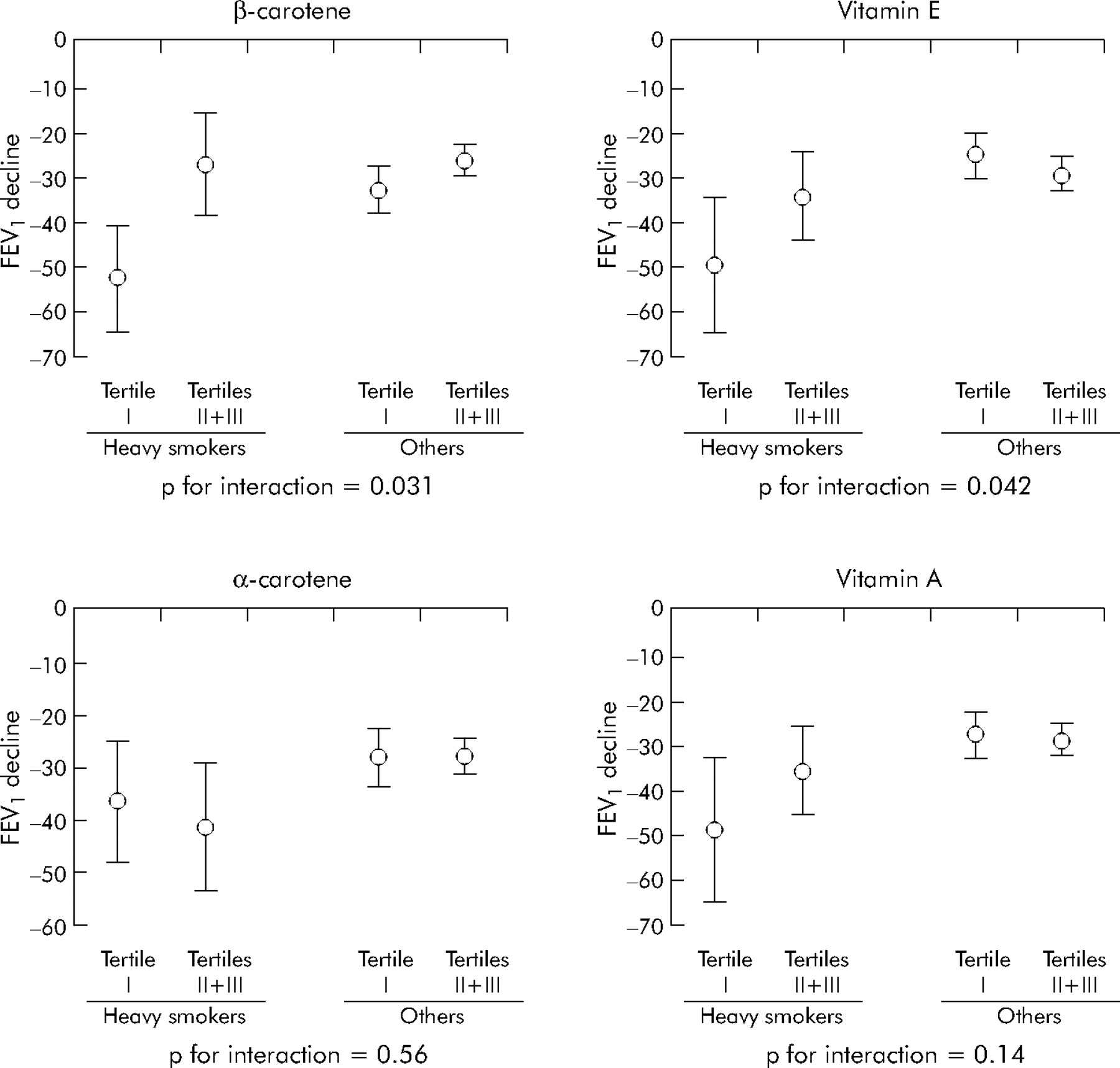
We explored the potential modification of the association between β-carotene and FEV1 decline by tobacco smoking. We first analysed lifelong non-smokers separately to discard any possible residual confounding by tobacco. The FEV1 of subjects in tertile I of β-carotene declined −37.8 ml/year (95% CI −46.1 to −21.9) whereas that of the subjects in tertiles II and III combined declined −25.6 ml/year (95% CI −30.0 to −21.0) (p = 0.013). We next analysed the effects of the interaction between heavy smoking and a low antioxidant level on FEV1 decline. We found that FEV1 declined at a rate of −52.5 ml/year (95% CI −64.4 to −40.6) (p for interaction = 0.031) in subjects who were heavy smokers in 1992 and had a low β-carotene level (tertile I) in 1992 (fig 2). The interaction with vitamin E was also significant (p = 0.042): FEV1 declined at a mean rate of −50.1 ml/year (95% CI −65.2 to −35.0) in heavy smokers with low vitamin E levels. Interactions with α-carotene and vitamin A were not significant.
{kind=link}
{kind=link}
Adjusted* mean (95% CI) annual decline in FEV1 (ml/year) according to antioxidant levels (tertile I v tertiles II and III combined) and heavy smoking (heavy smokers v others) at baseline (ECRHS I, 1992). *Multiple linear regression including sex, centre and baseline data for FEV1, age, BMI, and LDL cholesterol.
Association between lung function decline and changes in levels of antioxidants between 1992 and 2000
We first assessed FEV1 decline according to the tertiles of β-carotene concentration in 1992 and 2000 (table 4). The subjects in tertile I at both time points had the steepest decline in FEV1 (−40.0 ml/year) whereas those in tertile II or III at both time points had the slowest decline (−26.7 ml/year).
Mean (95% CI) adjusted* annual FEV1 decline (ml/year) according to tertiles of β-carotene in 1992 and in 2000
We next analysed the association between the decline in FEV1 and changes in antioxidant levels treated as continuous variables (mean annual changes). In the whole study population, an increase in β-carotene of 0.5 μmol/l (corresponding to 1 SD of change in β-carotene level per year*10 years) reduced the decline in FEV1 by 25.5 ml (p = 0.048) over 10 years, which approximately counteracts the effect of 1 year of ageing. When this analysis was restricted to the 164 subjects in tertile I at baseline, for the same increase in β-carotene, FEV1 decline over 10 years was reduced by 104.7 ml (p = 0.028) which approximately counteracts the effect of 4 years of ageing.
For α-carotene, vitamin A or vitamin E, no association was found between FEV1 decline and either tertiles at the two time points or mean annual change in antioxidant levels.
DISCUSSION
This is the first longitudinal study to explore the relationships between decline in lung function and serum levels of β-carotene, α-carotene, vitamin A, and vitamin E. Serum levels are likely to be better markers of lung tissue concentrations than dietary intakes assessed by questionnaires.17 We found that the β-carotene concentration was independently associated with the decline in FEV1, with the steepest decline occurring in subjects with the lowest β-carotene levels at baseline. No such association was observed for α-carotene, vitamin A, or vitamin E concentrations. However, being a heavy smoker with a low level of β-carotene or vitamin E was associated with the steepest FEV1 decline. An increase in β-carotene concentration between the two surveys was associated with a slower decline in FEV1. These results strongly suggest that β-carotene protects lung function in the general population and that β-carotene and also vitamin E have a protective effect in heavy smokers.
Validity and possible limitations
The protocol of the ECRHS was highly standardised and the quality of data was strictly controlled.14 As in any longitudinal study, there was some loss to follow up. However, our response rate is comparable to a recent population study.18 Not having all data available for all subjects may have affected representativeness. The subjects who were analysed were less than 2 years older than those excluded. Such a small difference is unlikely to have biased the association between lung function decline and antioxidants due to the young age of the study population and the small range of values (20−44 years in 1992). Analysed subjects were more frequently non-smokers and less frequently heavy smokers. This can only have weakened the overall association between antioxidants and lung function decline, as the association was stronger in heavy smokers. Participants had also less frequently worked in jobs where they were exposed to vapours, dust, gas or fumes than excluded subjects. If antioxidants act against occupational noxious particles as against cigarette smoke, the possible bias would be the same as for smoking habits. Mean age at full time education in the analysed subjects was slightly higher than in the excluded subjects. This could mean that the analysed subjects had a more affluent lifestyle and thus a higher intake of antioxidants, which would weaken the association studied by decreasing the proportion of subjects at risk.
The delay between serum collection and measurements (8 years on average for the samples collected during ECRHS I) is unlikely to have affected our results because all serum samples were frozen at −80°C and carotenoids, vitamin A, and vitamin E all appear to be stable for at least 15 years at this temperature.19 Although vitamin C is considered to be one of the most powerful antioxidants, we were unable to analyse any interaction between vitamin C and vitamin E because the study protocol for serum sampling was not adequate.
We observed the expected associations between lung function decline and factors such as sex, age, BMI, and smoking status which confirms the validity of the data. These confounding factors were all taken into account. The relationship between BMI and lung function decline is well documented.20,21 Serum LDL cholesterol level was associated with both antioxidant levels and decline in FEV1, and it has been shown that β-carotene and vitamin E are transported by LDL lipoproteins.22 To our knowledge, the association between lung function and LDL cholesterol has been investigated in only one study using the data from the Third National Health and Nutrition Examination Survey.23 The results were only cross sectional. Of the 14 135 subjects analysed (⩾ 17 years), LDL levels were negatively associated with FEV1 despite adjustment for BMI, and the association was strengthened after further adjustment for serum antioxidants (vitamin E, β-carotene, vitamin C, selenium). These results may be explained by the oxidation of LDL contributing to endogenous oxidative stress.24 As BMI and LDL levels at baseline were only moderately correlated (r = 0.27, p<0.0001), we simultaneously included both serum LDL cholesterol levels and BMI in the models. Other demographic and lifestyle factors such as educational level, physical activity, and occupational exposure are potential confounders but were not associated with FEV1 decline in our study, and adjusting for these factors did not change the results (data not shown).
Levels of β-carotene, vitamin A, and vitamin E were similar to those reported in studies exploring cross sectional relationships between lung function and serum levels of antioxidants.9,10,12 Levels of α-carotene were similar to those described in a study comparing five European countries including France.25
Consistency of the findings
The relationships between FEV1 decline and serum levels of β-carotene and α-carotene have never been explored, so we cannot compare our results with other studies. However, the internal consistency of the results is supported by the fact that the results were identical in the whole study population, in lifelong non-smokers, and when regression models were adjusted for baseline smoking status, baseline smoking status plus change in smoking status, or cumulative exposure assessed by pack years. Our results are also consistent with the results from observational studies on lung cancer risk.26,27 However, interventional trials of β-carotene supplementation showed an unexpected negative effect28,29 or no beneficial effect30 on the risk of lung cancer. A biologically plausible explanation for these unlikely findings has yet to be found.31
Vitamin A and vitamin E have already been analysed in longitudinal studies, with data collected using dietary questionnaires. One study that followed 1346 adults aged 18–70 years for 9 years found no association between the decline in FEV1 and intakes of either vitamin A or vitamin E, even in interaction with smoking status (coded as never smokers, 1 month ex-smokers, and current smokers).11 In another study in which 2512 men aged 45–59 years were followed for 5 years, neither average intake nor change in vitamin E intake was found to be related to change in lung function.13 Our results are consistent with the findings of these two studies: we found no association between vitamin A or vitamin E concentrations and lung function decline in the whole study population. However, we found that the interaction between low levels of vitamin E and heavy smoking had a strong effect on lung function decline.
Two hypotheses have been proposed to explain the effect of smoking status:9 (1) some antioxidants may neutralise “general” oxidants (those naturally encountered by non-smokers) more efficiently than oxidants found in cigarettes; and (2) some antioxidants may be more efficient when the oxidative stress is high. Our results agree with both hypotheses to some extent. Firstly, we observed that in non-smokers (with normal oxidative stress) high levels of β-carotene were associated with a less rapid decline in FEV1, which suggests that β-carotene is able to scavenge environmental or endogenous oxidants. Secondly, when the oxidative stress increased, as is the case in heavy smokers, low levels of β-carotene and also of vitamin E were associated with a more rapid decline in FEV1 (exceeding −50 ml/year). These antioxidants therefore seem to be able to partly counteract the damage caused by oxidants associated with heavy smoking, because the mean rate of FEV1 decline in heavy smokers with high levels of antioxidants was similar to that in other subjects. The hypothesis of a threshold effect of oxidative stress may explain why antioxidant levels did not interact with smoking in general when moderate and heavy smokers were pooled together versus the other smoking status (data not shown). In fact, the oxidant burden due to tobacco smoking in moderate smokers may have been too low. In our study sample the amount of tobacco smoked by heavy smokers was much greater than that smoked by moderate smokers with mean (SD) pack years at baseline in heavy smokers almost three times higher than in moderate smokers (29.0 (14.5) v 10.0 (8.9) pack years, p<0.0001). Moreover, heavy smokers started smoking at a younger age than moderate smokers (16.8 (2.6) v 18.6 (4.6) years, p = 0.002).
The results for heavy smokers should be discussed further. Heavy smokers were more sensitive to low levels of antioxidants than other subjects and also had lower mean β-carotene levels. This lower level may be due to lower dietary intakes or to metabolic differences resulting in lower serum concentrations of β-carotene at similar dietary intakes to non-smokers. In some studies, smokers have been shown to have significantly lower dietary antioxidant intake than non-smokers.32–34 In a large study of 1483 subjects aged 16–64 years it was found that, for the same level of dietary intake, smokers were more likely to have lower circulating levels of β-carotene than non-smokers.34 Another study showed an increase in the plasma concentration of β-carotene, α-carotene, and vitamins A and E in 15 smokers after 4 weeks of smoking cessation.35 Nevertheless, as the strength of the correlation coefficients between serum antioxidant levels and dietary antioxidant intake was only moderate,32,36,37 we cannot exclude a possible genetic influence38 or gene–environment interaction in the relationships between lung function decline, smoking, and antioxidant levels.
Possible mechanisms for the associations between antioxidants and lung function decline
There may be at least two explanations for the association between lung function decline and β-carotene and vitamin E concentrations. The first is antioxidant storage in the lungs. Redlich and co-workers39 examined the relationships between serum and lung tissue levels of β-carotene, α-carotene, vitamin A and vitamin E in 21 subjects undergoing a lung biopsy and found that serum and lung tissue levels of β-carotene were highly correlated (r = 0.72, p<0.0001). Thus, in the case of attack by oxidants, β-carotene may come into direct contact with harmful molecules. Serum and lung tissue levels of vitamin E were also positively correlated, but not as strongly as for β-carotene (r = 0.47, p = 0.03). As we observed a correlation between lung function decline and vitamin E concentration only in heavy smokers, we suggest that vitamin E breaks the lipid peroxidation chain reaction only when oxidative stress increases. Redlich et al found that lung tissue levels of vitamin A were very low and did not correlate with serum levels. The lack of an association between the decline in FEV1 and α-carotene levels may be explained by the low level of α-carotene in the lung tissue. Moreover, α-carotene and β-carotene levels are strongly associated in the serum (in our study as in a previous study7) but not in the lung.39
The second possible explanation is the specificity of the oxidants converted by β-carotene and vitamin E to a less reactive form. These two molecules scavenge the superoxide anion (O2·−) which has been shown positively to modulate airway smooth muscle contractility and proliferation.40,41 β-carotene and vitamin E may therefore protect against excessive airway smooth muscle contractility and/or proliferation by neutralising O2·− and thus protect against accelerated lung function decline.
In conclusion, this is the first longitudinal study to show that β-carotene and vitamin E may protect against accelerated decline in lung function, especially in heavy smokers. The decline in FEV1 was twice as great in heavy smokers with low levels of β-carotene or vitamin E as in the general young adult population studied. Subjects who sustain heavy smoking and continue to have low antioxidant levels are probably at very high risk of developing chronic obstructive pulmonary disease (COPD). These powerful antioxidants may help to reduce oxidative stress—one of the factors thought to be involved in the pathogenesis of COPD—and thus may contribute to reducing the risk of morbidity and mortality related to this disease.
Acknowledgments
The authors acknowledge the contribution made, first, by the subjects participating in the study; second, by the ECRHS II Steering Committee; and third, by researchers in study centres in organising the examination of the subjects, collecting data, and measuring serum levels of antioxidants, in particular: Joane Ferran and Valerie Siroux (Grenoble), Monique Guilloud-Bataille, Sabine Kony, Myriam Korobaeff, Catherine Neukirch, Bibi Ramoly-Domun and David Soussan (Paris), Clotilde Harault and Nathalie Cherubin (Laboratory Biochimie A, Bichat Teaching Hospital, Paris), members of Laboratory Biochimie B (Bichat Teaching Hospital, Paris), and members of the Centre for Clinical Investigation (CIC, Bichat Teaching Hospital, Paris). Particular thanks to Renata Liard for her help in writing the paper.
REFERENCES
Footnotes
-
Data collection for the European Community Respiratory Health Survey follow up phase (ECRHS II) was supported by UCB Pharma, France and by the Programme Hospitalier de Recherche Clinique-DRC of Grenoble 2000 no. 2610.
-
Competing interests: none.