Article Text

Abstract
Background: Physical exercise is an important component of respiratory rehabilitation because it reverses skeletal muscle dysfunction, a clinically important manifestation of COPD associated with reduced health-related quality of life (HRQL) and survival. However, there is controversy regarding the components of the optimal exercise protocol. A study was undertaken to systematically evaluate and summarise randomised controlled trials (RCTs) comparing different exercise protocols for COPD patients.
Methods: Six electronic databases, congress proceedings and bibliographies of included studies were searched without imposing language restrictions. Two reviewers independently screened all records and extracted data on study samples, interventions and methodological characteristics of included studies.
Results: The methodological quality of the 15 included RCTs was low to moderate. Strength exercise led to larger improvements of HRQL than endurance exercise (weighted mean difference for Chronic Respiratory Questionnaire 0.27, 95% CI 0.02 to 0.52). Interval exercise seems to be of similar effectiveness as continuous exercise, but there are few data on clinically relevant outcomes. One small RCT which included patients with mild COPD compared the effect of high and low intensity exercise (at 80% and 40% of the maximum exercise capacity, respectively) and found larger physiological training effects from high intensity exercise.
Conclusions: Strength exercise should be routinely incorporated in respiratory rehabilitation. There is insufficient evidence to recommend high intensity exercise for COPD patients and investigators should conduct larger high quality trials to evaluate exercise intensities in patients with moderate to severe COPD.
- chronic obstructive pulmonary disease
- rehabilitation
- exercise
- skeletal muscle dysfunction
Statistics from Altmetric.com
Chronic obstructive pulmonary disease (COPD) is the only cause of death from chronic disease that will increase worldwide until 2020,1 and it represents a big burden for patients2 and society.3–5 Respiratory rehabilitation combining interventions on the respiratory system (smoking cessation), psychological support (coping strategies), and physical exercise improves exercise capacity and health-related quality of life (HRQL)6 and is cost effective.7
Over recent years, investigators and clinicians have increasingly recognised the role of skeletal muscle dysfunction as an indicator of advanced stages of COPD.8–12 The physical exercise component has therefore become a cornerstone of respiratory rehabilitation.13–17 Several studies have shown that physical exercise reverses COPD induced skeletal muscle dysfunction as well as the morphological and metabolic changes of skeletal muscles.18,19 There is, however, substantial variation in exercise protocols used in clinical trials.20–23 This variation feeds an ongoing debate on the optimal exercise protocol13,19,24 and on how the general effect modifying principles, training intensity, specificity, and reversibility known from healthy subjects25 apply to COPD patients. Trial results are conflicting with regard to the intensity at which COPD patients should exercise, how intensity should be determined, and whether continuous or interval exercise is most appropriate. In addition, although most investigators agree that endurance exercise for lower extremities should be the main exercise modality,14,24 the role of strength and upper body exercise remains unclear.
Previous reviews have focused on the question of whether respiratory rehabilitation (including physical exercise) has any effect in improving exercise capacity and HRQL. Trials addressing this question have compared the intervention against groups without any exercise programme.6 These studies did not provide answers on the relative benefits and disadvantages of different exercise protocols. The aim of this systematic review is therefore to analyse all available randomised controlled trials (RCTs) with head to head comparisons of at least two exercise protocols (different exercise modalities and intensities or combinations thereof) to improve exercise capacity and HRQL in patients with COPD.
METHODS
Identification of studies
We searched MEDLINE (Ovid version, New York, from inception to May 2004), EMBASE (DataStar version, Cary, NC from inception to November 2003), PEDRO (online version, University of Sydney, Australia, November 2003) and the Cochrane Central Register of Controlled Trials (Oxford, UK, 2004, Issue 1) to identify relevant articles. We also searched the Science Citation Index database (Web of Science, Thomson ISI, Philadelphia, PA, USA) and PubMed using its “related articles” function (National Library of Medicine, Bethesda, MD, USA) by entering all included studies. The detailed search strategy is available on request.
Hand searches of the proceedings of the International Conferences of the American Thoracic Society and the congress of the European Respiratory Society, reference checks of bibliographies of all included studies and of reviews on respiratory rehabilitation or physical exercise in patients with COPD that we identified in the literature search, and contacts with authors complemented our searches.
Selection criteria
We included RCTs comparing different exercise modalities and intensities or combinations thereof that followed standardised exercise protocols for patients with COPD. We focused on standardised exercise protocols because only these allow replication in clinical practice. We defined a standardised exercise protocol as the use of an identical exercise activity for all patients (such as treadmill walking, cycle ergometer training, or weight lifting) at measurable exercise intensity (such as Watts, number of repetitions, kg, or percentage of one repetition maximum). Studies were included if more than 90% of participants had COPD defined according to the following criteria: (1) a clinical diagnosis of COPD; (2) irreversible airways obstruction; and (3) one of the following: (a) best recorded FEV1/FVC ratio of individual patients <0.7; (b) best recorded FEV1 of individual patients <70% of predicted value. We considered the following outcome measures: HRQL as measured by generic (e.g. Short Form-36) or disease specific (e.g. Chronic Respiratory Questionnaire (CRQ)) questionnaires; symptom scales; functional exercise capacity as measured by 2, 4, 6, 12 minute walk test or a shuttle walk test; and maximum exercise capacity as measured by incremental or constant work rate exercise tests on cycle ergometers or treadmills. In addition, we extracted data on exercise tolerance (adherence to exercise protocols, completion of exercise programme, losses to follow up) and on physiological parameters documenting training effects (such as lactate, anaerobic threshold) for studies where no clinical outcomes were available. We did not impose language restrictions.
Data extraction and quality assessment
The bibliographic details of all retrieved articles were stored in a Reference Manager file (Professional Edition Version 10, ISI ResearchSoft, Berkeley, CA, USA) and duplicate records resulting from the various database searches were removed. Two members of the review team independently scrutinised the titles and abstracts of all identified citations (fig 1). The full text of any article that was deemed potentially eligible was ordered by one of the reviewers. The two reviewers evaluated the full text of all retrieved papers, made a decision on inclusion or exclusion, and discussed the decisions. Any disagreement was resolved by consensus with close attention to the inclusion/exclusion criteria. Final decisions on papers were recorded in the Reference Manager file and bibliographic details as well as the reasons for exclusion. We recorded the initial degree of discordance between the reviewers and corrected discordant scores based on obvious errors. Discordant scores were resolved based on real differences in interpretation through consensus or third party arbitration.

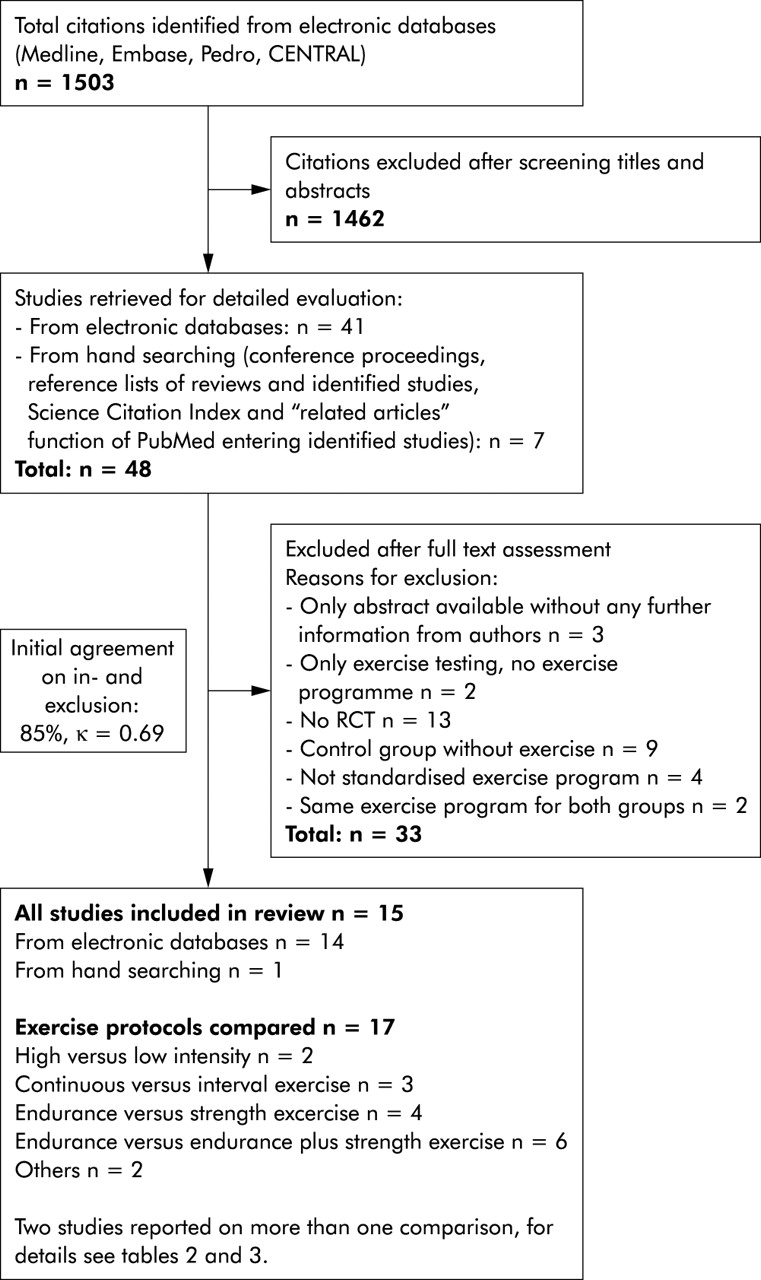
Study flow from identification to final inclusion of studies.
One reviewer extracted details about study patients, interventions, and outcome measures as well as the results in a predefined data form and the second reviewer checked the data extraction for accuracy. We pilot tested the data forms using five studies with a high likelihood for inclusion. We contacted the authors of the primary studies to obtain missing information. If only the abstract was available without any further information from the authors, the study was excluded from the analysis.
Two reviewers independently evaluated the quality of included trials using a detailed list of quality items assessing components of validity (see data available on the Thorax website at http://www.thoraxjnl.com/supplemental).26
Methods of analysis and synthesis
The results of the data extraction and assessment of study validity were summarised in structured tables to explore the variation in patient characteristics, interventions, outcome measures, study quality and results. Forest plots were used to compare results across the trials. If appropriate, we planned to explore sources of heterogeneity (that is, differences between studies) using multivariable regression models (meta-regression analysis) where a priori defined clinical and methodological items would serve as explanatory variables. A priori defined explanations for heterogeneity across trials were severity of disease, length of intervention (< or ⩾6 months), exercise modality (for example, endurance exercise on bicycle or treadmill), exercise intensity (for example, strength exercise with high work load and few repetitions versus low work load and numerous repetitions), exercise tests used to determine exercise load, and comprehensiveness of rehabilitation programme (patient education, psychosocial support, breathing exercises, relaxation therapies).
The trial results were pooled by calculating weighted mean differences. Since random and fixed effect models produced the same results, only the results from fixed effect models are presented. No pooling was undertaken in the presence of significant heterogeneity (p<0.1 for Q statistic).
Whenever possible, estimates and confidence limits were related to the minimal important difference (MID)27 for each outcome. We assessed whether the estimates and 95% confidence limits for the difference between study groups exceeded the MID (for the 6 minute walk distance the MID is ±53 m,28 CRQ ±0.5 on 7-point scales,29 and St George’s Respiratory Questionnaire ±4 points30).
All statistical analyses were done with STATA Version 8.2 (Stata Corp, College Station, TX, USA).
RESULTS
Study selection
Figure 1 shows the study selection process and agreement on study inclusion. Of the 18 trials fulfilling the inclusion criteria, three were excluded from further analysis because they were published as abstracts and the authors were unable to provide further details.31–33
Quality assessment
The table in the online supplement shows the methodological quality of the included trials. Agreement in the quality assessment was 90.7% for all items (κ = 0.72). In general, most included trials scored poorly on the checklist used. Just one trial34 described concealment of random allocation, another trial35 used stratification to control for prognostically important variables, and one trial34 reported blinding of outcome assessors.
Comparisons of training modalities
Endurance exercise v strength exercise
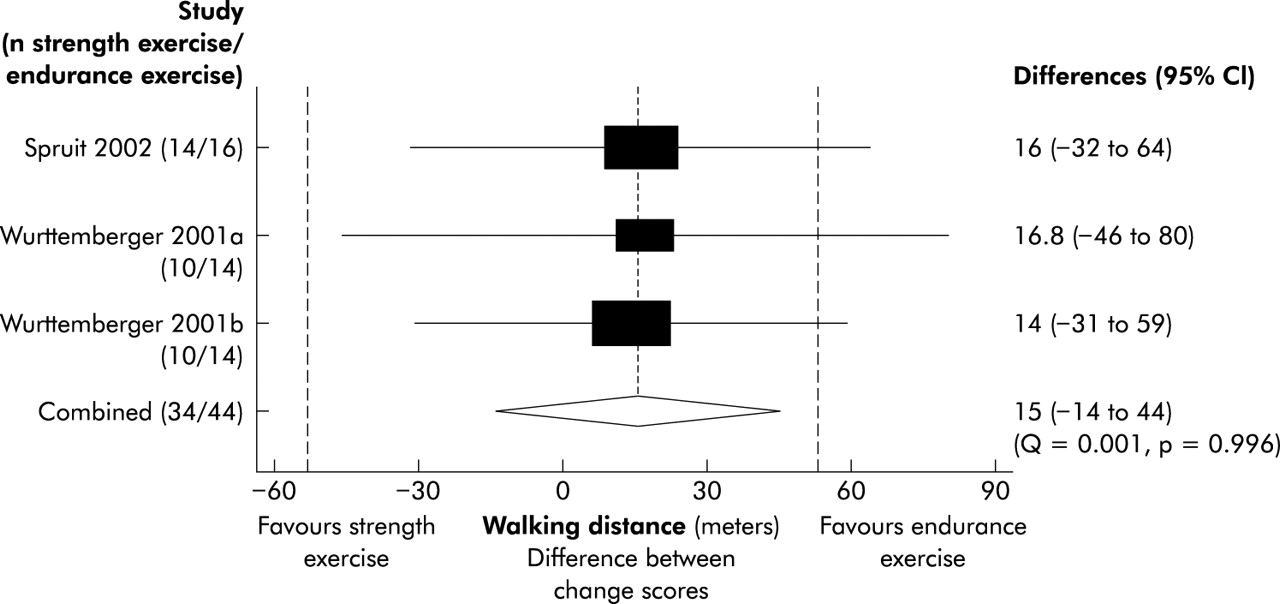
Four trials compared endurance and strength exercise (table 1).34,36–38 The weighted mean differences showed larger improvements with strength exercise for all CRQ domains (fig 2). The differences were statistically significant for the emotional function domain (−0.38, 95% CI −0.01 to −0.74) and for the CRQ total score (−0.27, 95% CI −0.02 to −0.52). One trial37 found larger improvements in functional exercise capacity using shuttle walk tests for the group with strength exercise (70 m, 95% CI −19 to 159), but the variability in the results was much larger than in the trials that used 6 minute walking tests. Three trials showed greater improvement in 6 minuts walking distance for patients with endurance exercise (fig 3), but the weighted mean difference did not reach statistical significance (15 m, 95% CI −14 to 44). The endurance exercise group showed larger improvements in maximum exercise capacity in one trial37 (mean difference between endurance and strength exercise groups of 6 Watt, 95% CI −2.2 to 14.2), while there were similar improvements for endurance and strength exercise in another trial34 (mean difference –1 Watt, 95% CI −11.5 to 9.5). Two trials showed significantly larger improvements in exercise time during constant work rate tests for the strength exercise group (5.7 minutes, 95% CI 3.0 to 8.4,36 and 25.3 minutes, 95% CI 12.7 to 37.937). Ortega et al37 and Normandin et al36 found significantly larger improvements in skeletal muscle strength in the strength exercise group while Spruit et al34 observed similar improvements in both groups. The exercise programmes of Spruit et al differed from those of Normandin et al and Ortega et al in that patients had two types of endurance training (table 1) which may have resulted in a crossover effect leading to an absence of differences between the strength and endurance exercise groups. However, the number of trials was too small to assess this source of heterogeneity statistically.
Characteristics of randomised controlled trials comparing strength and endurance exercise

Results from three trials in which the CRQ was used to compare strength exercise with endurance exercise. Boxes with 95% confidence intervals represent point estimates for the difference between the CRQ change scores (from baseline to follow up) of the study groups. A difference of 0 means that both study groups improved or deteriorated to the same amount. Results are presented per CRQ domain. Dashed lines at ±0.5 represent the minimal important difference of the CRQ.
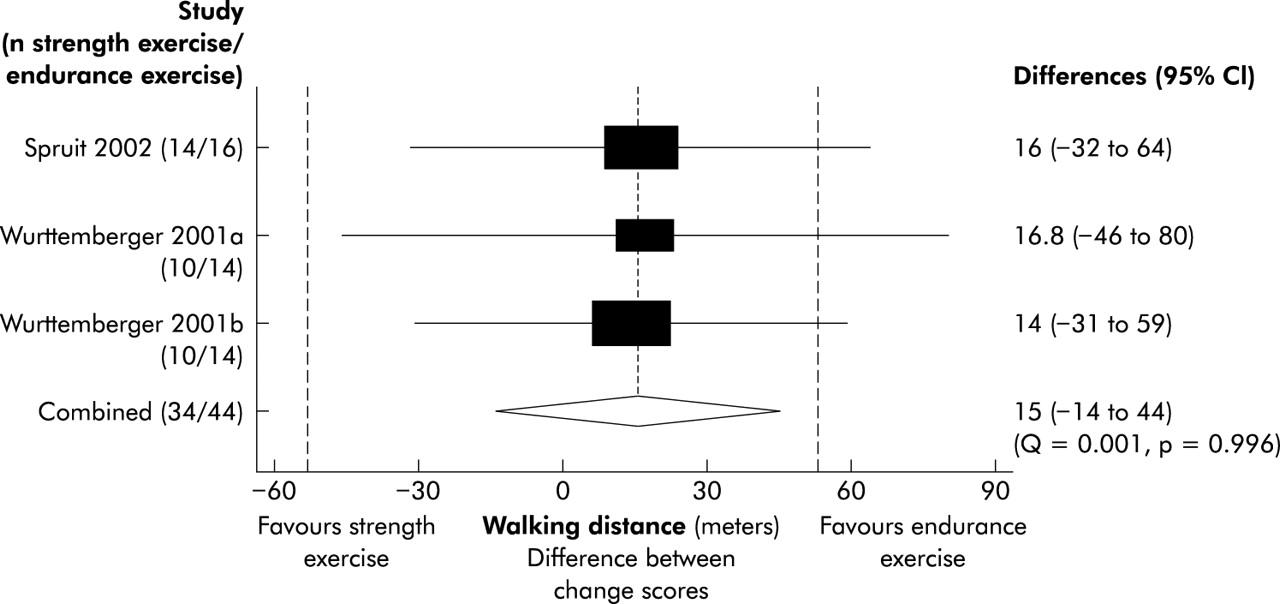
Results from three trials in which walking tests were used to compare strength exercise with endurance exercise. Boxes with 95% confidence intervals represent point estimates for the difference between the walking distances (from baseline to follow up) of the study groups. A difference of 0 means that both study groups improved or deteriorated to the same amount. Dashed lines at ±53 metres represent the minimal important difference of the 6 minute walk test.
The number of patients not completing the exercise programme was similar in groups with endurance (Normandin, n = 7; Ortega, n = 2; and Spruit, n = 8) and strength exercise (Normandin, n = 7; Ortega, n = 1; and Spruit, n = 10).
Endurance exercise v endurance + strength exercise
Six articles37–42 reported on seven RCTs comparing endurance exercise only with endurance plus strength exercise (table 1). Wurttemberger presented the results of patients with and without oxygen desaturation during exercise separately in one article.38 Five trials37–40 had similar exercise protocols for the study groups with endurance only or combined endurance plus strength exercise. There were no differences between groups in terms of HRQL or functional and maximum exercise capacity improvements (figs 4 and 5). Improvements in exercise endurance were similar in both groups in one trial40 (mean difference between endurance exercise alone and combined endurance and strength exercise group −0.3, 95% CI −8.1 to 7.5), while another trial37 showed larger, although statistically not significant, improvements in the endurance exercise group (mean difference 9.6 minutes, 95% CI −3.9 to 23.1). The larger improvements in muscle strength in the groups with endurance plus strength exercise as reported in three trials37,39,40 did not therefore translate into additional benefits in terms of HRQL or exercise capacity.

Results from three trials in which the CRQ was used to compare a combination of endurance and strength exercise with endurance exercise alone. Boxes with 95% confidence intervals represent point estimates for the difference between the CRQ change scores (from baseline to follow up) of the study groups. A difference of 0 means that both study groups improved or deteriorated to the same amount. Results are presented per CRQ domain. Dashed lines at ±0.5 represent the minimal important difference of the CRQ.

{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
Results from six trials in which walking tests and incremental exercise tests were used to compare a combination of endurance and strength exercise with endurance exercise alone. Boxes with 95% confidence intervals represent point estimates for the difference between the walking distances and maximum exercise capacity change scores (from baseline to follow up) of the study groups. A difference of 0 means that both study groups improved or deteriorated to the same amount. Dashed lines at ±53 meters represent the minimal important difference of the six-minute walk test.
Continuous v interval exercise
Three trials compared continuous and interval exercise (tables 2 and 3).35,43,44 One trial43 found a larger increase in peak oxygen consumption and lower lactate levels at sub-maximal exercise intensity with continuous exercise than with interval exercise. In contrast, only interval exercise led to significant increases in maximum exercise capacity and decrease of leg pain during exercise. 91% of patients with continuous exercise and 90% of patients with interval exercise completed the exercise programme. In another trial35 HRQL, maximum exercise capacity, and peak oxygen uptake improved significantly in both groups without significant differences between them. Attendance rate for exercise sessions was 88% for continuous exercise and 90% for interval exercise in this trial. Finally, in the third trial44 patients with interval exercise had a trend towards larger improvements in 6 minute walking distance compared with patients with continuous exercise.
Characteristics of randomised controlled trials comparing exercise modalities and intensities
Effect of different exercise intensities
Other comparisons
Rooyackers et al45 assessed the additional value of eccentric exercise (negative work) when added to interval exercise (table 2). Patients tolerated additional eccentric exercise for 15 minutes at moderate to high intensity (mean 69% of maximum exercise capacity) well (Borg dyspnoea score ⩽3), but this did not lead to improvements in HRQL or exercise capacity (table 3). The only significant difference favouring additional eccentric exercise existed for oxygen tension at maximum exercise capacity (7.9 v 6.9 kPa, p<0.05).
Martinez et al46 compared the effects of supported (arm ergometer exercise) and unsupported upper extremity exercises (dowel lifting exercises resembling daily activities) when added to a lower extremity endurance and respiratory muscle training (table 2). Both the group with and those without supported arm exercise significantly improved functional and maximum exercise capacity as well as respiratory muscle strength to a similar degree. Improvements in power output during arm ergometry were similar for both groups while patients with unsupported arm exercises had a significantly larger increase in unsupported arm endurance and a decrease in oxygen consumption.
Comparisons of training intensities
One small trial47 compared the effect of high and low intensity exercise in middle aged patients with mild COPD (table 2). The trial showed that high intensity exercise at 80% of maximum exercise capacity yielded a bigger physiological response in terms of reductions in exercise induced lactate acidosis and ventilation (table 3). The larger training effect after high intensity exercise led also to longer endurance time.
Vallet et al48 (table 2) assessed whether exercise at the individual anaerobic threshold was more effective than exercise at 50% of the maximal heart rate reserve (standardised protocol). Mean exercise intensities between the groups were not different. The authors reported a trend towards larger increases of peak oxygen uptake and anaerobic threshold with the individualised exercise protocol (table 3). There was a significantly greater training response in the group with the individualised protocol in terms of reductions in minute ventilation, lactate levels, and carbon dioxide output at given levels of pre-training oxygen uptake (data available only from figures).
DISCUSSION
There are three principal results from this systematic review. Firstly, strength exercise yielded larger improvements in HRQL than endurance exercise. Secondly, interval exercise may represent an alternative to continuous exercise but the methodological quality of the evidence is low and does not favour one or other exercise modality. Finally, there is only low quality evidence that high intensity exercise is superior to low intensity exercise.
In general, only few trials addressed important aspects of study design such as methods of randomisation and concealment of random allocation. While blinding of patients and therapists is hardly possible in respiratory rehabilitation programmes (items rated as not applicable), blinding of outcome assessors is feasible as in any other RCT. There are empirical data that lack of blinding is associated with significant bias.49,50 Only one trial,34 however, reported blinding of outcome assessors. Thus, one needs to bear in mind the limited methodological quality of included trials for the following discussion.
In clinical practice and in clinical trials, most rehabilitation programmes include endurance exercise, but not always strength exercise.6 Although investigators and clinicians have discussed the importance of peripheral muscle strength for daily activities repeatedly, there is no consensus on the role of strength exercise during respiratory rehabilitation.10,24,51,52 Data tend to suggest, however, that strength exercise should be considered likewise. Strength exercise led to larger improvements in HRQL than endurance exercise (fig 2). There is some evidence that muscle strength is associated with HRQL,53 which would explain the effect of strength exercise on the CRQ fatigue, emotional function and mastery domains (fig 2). However, more studies are needed to confirm this potential association.
The trials comparing endurance and a combination of endurance and strength exercise showed less clear results (figs 4 and 5). One could attribute this finding to the fact that patients in both intervention groups had the same intervention in most trials (endurance exercise), which led to similar effects. Specific strength training effects were also observed when strength exercise was added,37,39,40 but the contrast between groups appeared to be too small to show differences in terms of HRQL, even in pooled analyses.
Interval exercise is considered to be a promising approach to provide sustainable high intensity exercise for COPD patients because it allows for short periods of recovery preventing high lactate accumulation.24,54 There is some evidence of this from three RCTs35,43,44 comparing interval exercise and continuous exercise. The results indicate that both modalities improved exercise capacity, dyspnoea, and HRQL to a similar degree. However, the non-significant differences between treatment groups do not allow us to conclude that interval or continuous exercise are of clinically equivalent effectiveness.55 These trials were not designed to show clinical equivalence and they did not provide evidence that interval exercise is better tolerated. In one trial with an inpatient rehabilitation programme,43 patients in the interval exercise group had a mixed intervention (3 days of interval and 2 days of continuous exercise per week) so that differences cannot be attributed to different interventions even if they were detected. Although interval exercise may offer an attractive alternative for COPD patients, more trials are needed with rigorous methodology and outcomes which consider the relative effectiveness and tolerance of interval exercise compared with continuous exercise.
A surprising finding of this review is that evidence favouring high intensity over low intensity exercise is weak. High intensity exercise is usually defined as exercise at ⩾60–90% of the maximum exercise capacity, but there is no consensus on the lower or upper limit to define high intensity exercise.24 There is one frequently cited trial47 comparing high and low intensity exercise that was small and had several methodological limitations (see online data). The reductions in lactate acidosis and larger improvements in exercise endurance were not reproduced in later trials nor are any data available on the effect of high and low intensity exercise on HRQL and other patient outcomes. It is also uncertain whether the results from this single trial47 apply to patients with moderate to severe COPD, because these patients are often unable to sustain high intensity exercise even though they achieve significant improvements in exercise capacity with lower exercise intensities.56,57 Future research should therefore look at the intensity at which patients with COPD should and can exercise to achieve patient important training effects and explore the influence of baseline disease severity.
In conclusion, strength exercise tends to improve HRQL more than endurance exercise. More research is needed to assess the relative benefits and disadvantages of interval exercise compared with continuous exercise and to define optimal exercise intensity for patients with COPD. Future studies should be planned and executed with more care to allow assessment of the variability in response to exercise and to provide more robust estimates of differences between the effects of exercise protocols.
Acknowledgments
The authors thank Dr Pius Estermann, Information Officer, University Hospital of Zurich who designed and conducted the searches of electronic databases.
REFERENCES
Supplementary materials
The table and references are available as a downloadable PDF (printer friendly file).
If you do not have Adobe Reader installed on your computer,
you can download this free-of-charge, please Click hereFiles in this Data Supplement:
- [view PDF] - Internal validity of included studies
Footnotes
-
Funding: Helmut Horten Foundation Research Fellows and Swiss National Science Foundation (PROSPER programme) grant numbers 3233B0–103182 and 3233B0–103183, L M Bachmann.
-
Competing interests: none declared.
-
Contributors: Study concept and design (MAP, LMB); study retrieval and data extraction (MAP, LMB, MS); analysis and interpretation of data (MAP, LMB, MF, HJS); drafting of manuscript (MAP); critical revision of manuscript for important intellectual content (LMB, MF, HJS, MS).
Linked Articles
- Airwaves