Article Text

Abstract
Background: Inhaled corticosteroids and leukotriene receptor antagonists reduce airway eosinophilia and have been used as first line anti-inflammatory therapy for mild persistent asthma.
Methods: A multicentre, randomised, placebo controlled, parallel group study was performed to compare the anti-inflammatory effects of fluticasone propionate and montelukast as measured by sputum eosinophils in 50 adults with symptomatic steroid naive asthma and sputum eosinophilia of ⩾3.5%.
Results: Eighteen patients received low dose fluticasone (250 μg/day), 19 received montelukast (10 mg/day), and 13 were given placebo for 8 weeks. Fluticasone treatment resulted in a greater reduction in sputum eosinophils (geometric mean (SD) 11.9 (2.3)% to 1.7 (5.1)%) than montelukast (10.7 (2.3)% to 6.9 (3.8)%; p = 0.04) or placebo (15.4 (2.4)% to 7.8 (4.2)%; p = 0.002), and improvement in FEV1 (mean (SD) 2.6 (0.9) l to 3.0 (0.9) l) than montelukast (2.8 (0.7) l to 2.8 (0.9) l; p = 0.02) or placebo (2.4 (0.8) l to 2.4 (0.9) l; p = 0.01). Treatment with fluticasone suppressed sputum eosinophilia within a week while montelukast only attenuated it. The effect of montelukast was maximal at 1 week and was maintained over 4 weeks. The effect of fluticasone was maintained over 8 weeks while that of montelukast was not.
Conclusions: Montelukast is not as effective as low dose fluticasone in reducing or maintaining an anti-inflammatory effect in steroid naïve eosinophilic asthma.
- asthma
- eosinophilic asthma
- montelukast
- fluticasone
- anti-inflammatory effect
Statistics from Altmetric.com
Anti-inflammatory treatment is critical in the management of asthma1,2 because airway inflammation is regarded as the primary cause of asthma symptoms, exacerbations, reversible airflow limitation, airway hyperresponsiveness (AHR), and remodelling. The latter is thought to contribute to the AHR and development of chronic airflow limitation.3,4 Airway inflammation can be easily measured in induced sputum cell counts. Normal values are well documented5 and the measurements are reliable, valid, and responsive.6
Sputum cell counts demonstrate different types of inflammation due to different causes. These are eosinophilic (due to inhaled allergens or chemical sensitisers to which the patient is allergic or sensitised, or to inadequate steroid treatment), neutrophilic (which can be trivial and non-specific or more intense due to viral or bacterial infections), eosinophilic and neutrophilic, or neither.7 Differentiating these types is important for refining treatment. For example, eosinophilia responds to adequate steroid treatment while current evidence suggests that, if there is no eosinophilia, steroid treatment is ineffective.8
Inhaled corticosteroids such as fluticasone propionate are the gold standard anti-eosinophilic inflammatory therapy.1,2 They reduce symptoms,9 airflow limitation,10,11 AHR,12,13 exacerbations,14 hospital admissions,15,16 and mortality15–17 due to asthma. Leukotriene receptor antagonists such as montelukast also have anti-inflammatory properties, reducing18,19 or preventing20 airway eosinophilia in asthma. When compared with placebo they also improve asthma symptoms,21 airway function,22 and reduce asthma exacerbations.23,24 As a result, leukotriene antagonists have been acknowledged by some guidelines2 as acceptable first line anti-inflammatory treatment.
However, there is limited direct evidence to support the use of the leukotriene antagonists as first line anti-eosinophilic inflammatory treatment in comparison with an inhaled steroid. Two large randomised controlled trials compared the clinical efficacy of montelukast25 or zafirlukast26 with fluticasone propionate. They showed that the benefit from treatment with the leukotriene receptor antagonists was limited compared with low doses of fluticasone. One crossover study,27 not placebo controlled, compared the effects of inhaled fluticasone 200 μg/day with montelukast 10 mg/day on inflammatory markers in induced sputum. Fluticasone was shown to decrease sputum eosinophils significantly after 4 weeks. Montelukast also decreased eosinophils after 4 weeks, but not significantly. Although the authors claimed fluticasone treatment to be superior, the difference between the interventions was not significant.
The primary objective of this study was therefore to compare the magnitude of anti-inflammatory effects of montelukast with fluticasone in subjects with asthma and sputum eosinophilia in a four centre, randomised, double blind, placebo controlled trial over 8 weeks. The anti-inflammatory effects were measured by induced sputum eosinophils.
METHODS
Participants
Adults with persistent symptomatic asthma who had only taken a short acting bronchodilator for at least 2 months were recruited from the chest clinics of three Canadian and one Brazilian research centre (table 1). Asthma was diagnosed by standard criteria2 or by AHR to methacholine with a PC20 of <8 mg/ml if the FEV1/SVC was >70% (fluticasone n = 4, montelukast n = 1, placebo n = 2). All subjects had induced sputum eosinophilia of ⩾3.5% (normal <2%).5 None had symptoms of a cold or flu during the month before the start of the study.
Characteristics of patients at baseline
The research ethics boards of the participating centres approved the study and each participant gave written informed consent.
Design of study
This was a four centre randomised, double blind, double dummy, parallel group placebo and active controlled trial over 8 weeks which was initiated, planned, performed, analysed and reported without influence from industry. The primary outcome was the effect of treatment on sputum eosinophils. Secondary outcomes were improvement in clinical variables (symptoms, bronchodilator use and pre-bronchodilator FEV1).
There were six visits to the clinic, each at the same time of day ±2 hours. At the initial visit inclusion and exclusion criteria were reviewed, pre and post salbutamol spirometric tests and sputum induction were performed, and peripheral blood was collected for liver function tests. Subjects who met the entry criteria returned on the following day for visit 2 when clinical characteristics were recorded, allergy skin prick tests and, if necessary a methacholine inhalation test was performed. Subjects were also instructed on how to complete a diary card of symptoms, peak expiratory flow (PEF) for safety, medication use, and adverse events. They were then randomly allocated to receive daily fluticasone 50 μg two puffs in the morning and three puffs in the evening (250 μg/day) and placebo tablet in the evening, montelukast 10 mg in the evening and placebo inhaler, or placebo inhaler and placebo tablet. Subsequent visits were on days 7, 14, 28 and 56 (visits 3, 4, 5 and 6). The procedures at these included symptom questionnaires and adverse events, review of diary cards, spirometry, induced sputum, and a compliance check. Blood for liver function tests was also taken at day 56.
Exacerbations were defined by a worsening of symptoms requiring treatment with four or more extra puffs/day of short acting β2 agonist from baseline over 48 hours, or by nocturnal or early morning waking two or more times over baseline, or by a fall in pre-bronchodilator FEV1 of ⩾15% from initial spirometry. If an exacerbation occurred, fluticasone 125 μg two puffs twice daily was added to the treatment; if patients continued to exacerbate they were withdrawn from the trial and treated appropriately.
Measurements
Questionnaires were used to document subject characteristics. Symptom severity (chest tightness, shortness of breath, wheezing, cough and nocturnal and/or early morning awakening) was graded on a validated 7 point Likert scale.28 Symptom scores ranged from 5 (most severe discomfort) to 35 (asymptomatic). Daily use of short acting β2 agonist was also recorded. Allergy skin prick tests, spirometric tests, and methacholine inhalation tests were carried out by standardised methods.29–32 Compliance with medications was checked by weighing inhaler canisters and counting tablets. PEF measurements were performed with a mini-Wright peak flow meter on waking and before bed. Sputum induction33 and processing6 for total and differential cell counts were performed by the methods described by Pizzichini et al. Liver function tests (bilirubin, alanine transaminase, aspartate transaminase, gamma glutamyl transaminase, and alkaline phosphatase) were performed by routine laboratory methods.
Sample size
Sample size estimation was calculated for the study primary outcome measure—the difference in sputum eosinophil count between fluticasone and montelukast. In a previous study34 comparing beclomethasone (BDP) with placebo in mildly uncontrolled asthma, BDP 1000 μg daily reduced the baseline sputum eosinophil count from a mean (SD) of 22.5(17.9)% to 5.7(6.8)%. Montelukast has been shown to reduce the sputum eosinophil count in mild asthmatics from 7.5% to 3.9% (95% CI −16.6 to 0.4).18 Based on these data, a sample size of 16 in each active arm would have 80% power to detect an absolute difference of 13% in the reduction in the eosinophil count by fluticasone compared with montelukast at an alpha of 0.05 (two tailed) and a beta of 0.2.
Statistical analysis
Descriptive statistics were used to summarise the clinical characteristics of the participants. Variables with non-normal distribution (sputum total cell count and eosinophils) were log transformed before analysis. ANOVA with post hoc analysis adjusted for multiple comparisons were used to determine the comparability between groups at baseline. The effects of treatment on the primary and secondary outcomes were compared using a two factor repeated measures ANOVA adjusting for baseline differences. The within subject factor was repeated measures (or time) before and after treatment. The between subject factors were centre and treatment group. Change and percentage change from baseline were examined for each outcome. Significant variation between groups was identified by the Tukey test and the p value was adjusted for multiple comparisons. All statistical tests were two sided and significance was accepted at the 95% level. The end point was defined as the last value obtained before any added open label fluticasone. The least clinically important difference in sputum eosinophils after intervention was regarded as a 50% reduction35 and for FEV1 was a change of >12%.
RESULTS
Randomisation, withdrawals, exacerbations and compliance
Fifty eligible participants were randomised to the treatment groups: 19 to receive montelukast, 18 to receive fluticasone and 13 to receive placebo (fig 1). There were no significant differences in clinical or physiological parameters between the treatment groups at baseline (table 1). One patient in the placebo group was excluded from the study early after randomisation because of protocol violation and was not included in the analysis. Of the remaining 49 patients, one in each group was withdrawn before the end of the study: one on montelukast after 2 weeks and one on placebo after 4 weeks were lost to follow up, and one on fluticasone after 2 weeks had a rash, abdominal discomfort and dysuria. All the available results for these patients before withdrawal were analysed. Four patients exacerbated during the study, requiring open label fluticasone: one on placebo, two on montelukast, and one on fluticasone. One subject exacerbated at day 7 (placebo) and three at day 14; their results were analysed up to these visits. They then received open labelled fluticasone and were improved by the added treatment. Compliance was satisfactory (>96%).

Profile of trial.
Effects on sputum eosinophilia
The percentage of eosinophils did not differ significantly between the three groups at the pretreatment visit (table 1). After fluticasone treatment an important decrease in sputum eosinophilia was measured as early as 7 days from a geometric mean (SD) of 11.9 (2.3)% to 2.5 (5.1)% (fig 2). After 4 and 8 weeks fluticasone completely suppressed sputum eosinophilia to 1.7 (4.5)% and 1.7 (5.1)% (table 2, fig 2). Treatment with montelukast only attenuated sputum eosinophilia up to 4 weeks. After 7 days, 4 weeks and 8 weeks montelukast reduced sputum eosinophilia from 10.7 (2.3)% to 3.8 (3.8)%, 4.5 (3.5)% and 6.9 (3.8)% (p = 0.9 in comparison with placebo at the end of the study). Placebo treatment did not significantly affect sputum eosinophils after 7 days, 4 weeks or 8 weeks. The geometric mean difference between the effects of fluticasone and placebo on sputum eosinophils was −4.0% (95% CI −10.2 to −1.6), p = 0.002 and montelukast was −2.3% (95% CI −5.2 to −1.0), p = 0.04.
Primary and secondary outcomes at baseline and 8 weeks after treatment

Effects of treatment on sputum eosinophils expressed as geometric mean and error. Fluticasone (stars) completely suppressed sputum eosinophilia after 4 and 8 weeks of treatment (p at 8 weeks = 0.04 and 0.002, respectively, v placebo (open circles) and montelukast (closed circles)). Treatment with montelukast attenuated sputum eosinophilia only up to 4 weeks (p = 0.9 after 8 weeks).
We also examined the effects of the study treatments on sputum eosinophilia as a percentage reduction. The median reduction in sputum eosinophilia after fluticasone on day 7 was 72.7% compared with 56.2% and 34.9% after montelukast and placebo. At 8 weeks the eosinophilia, in comparison with baseline, was reduced by 84.1% after fluticasone, 17.5% after montelukast, and 31.4% after placebo.
Effects on clinical variables
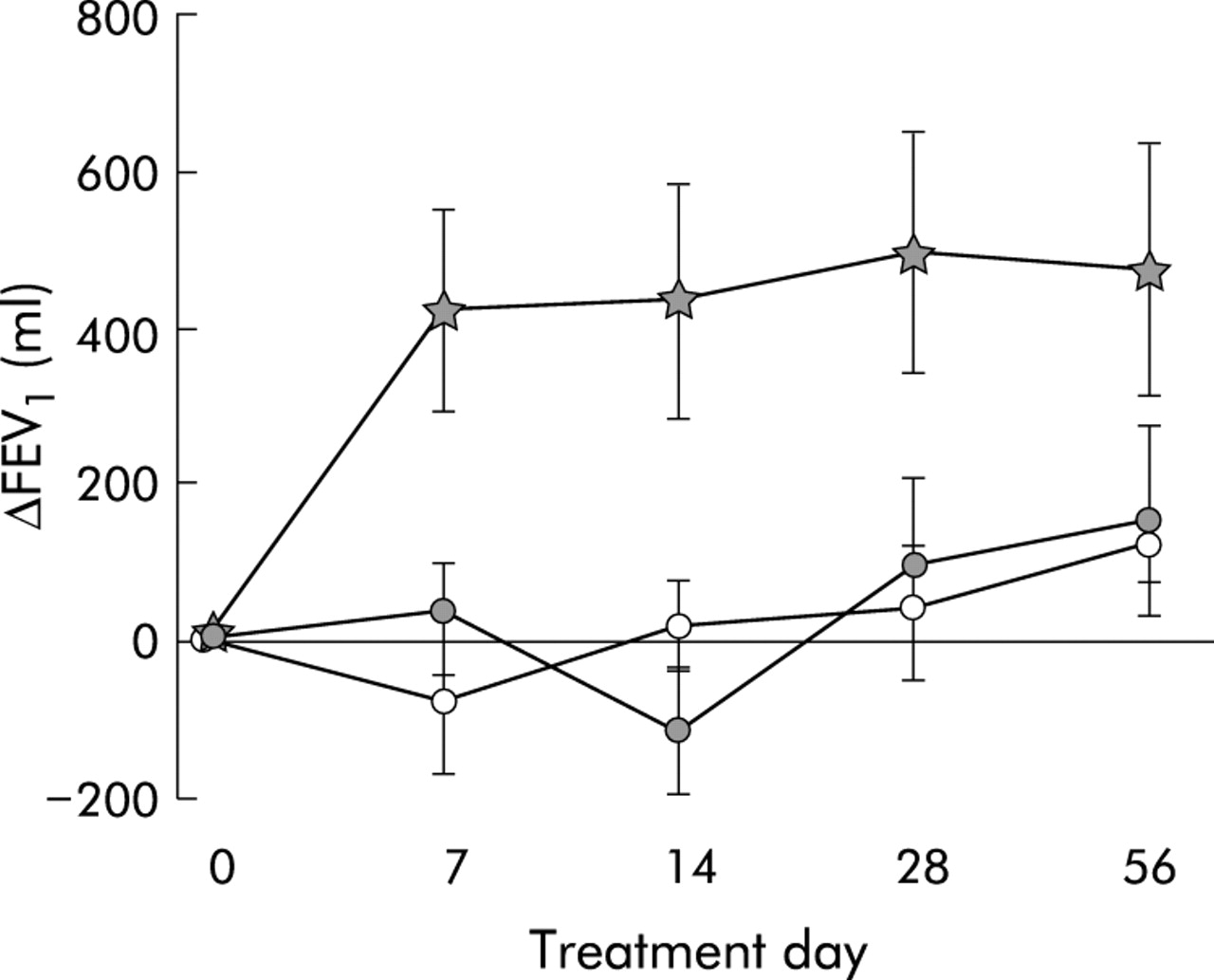
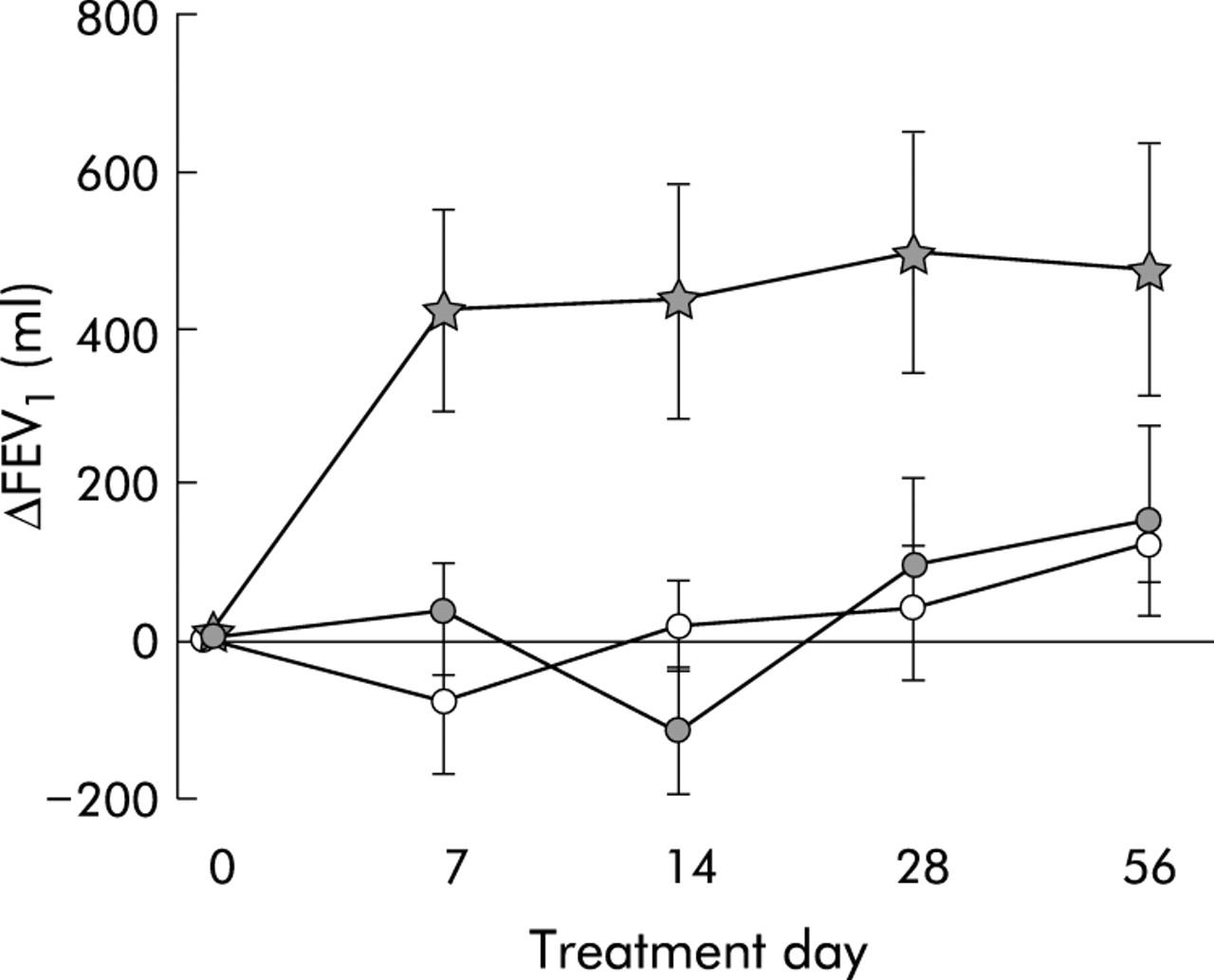
The effects of treatment on clinical variables are shown in table 2. Treatment with fluticasone produced a significant increase in pre-bronchodilator FEV1 by day 7 (fig 3) which was maintained (fig 4). The mean change in FEV1 on day 7 was 425 ml (95% CI 151.7 to 698.3) after fluticasone, 33 ml (95% CI −108 to 174) after montelukast, and −142 ml (95% CI −355 to 70) after placebo. By 8 weeks the FEV1 was increased by 475 ml (95% CI 131 to 820) after fluticasone, 156 ml (95% CI −77.7 to 383) after montelukast, and 125 ml (95% CI −64 to 250) after placebo. The difference between the effects of fluticasone and placebo on FEV1 was 458 ml (95% CI 73 to 842) and between fluticasone and montelukast was 373 ml (95% CI 26 to 720); p = 0.02 and 0.03 for both comparisons.
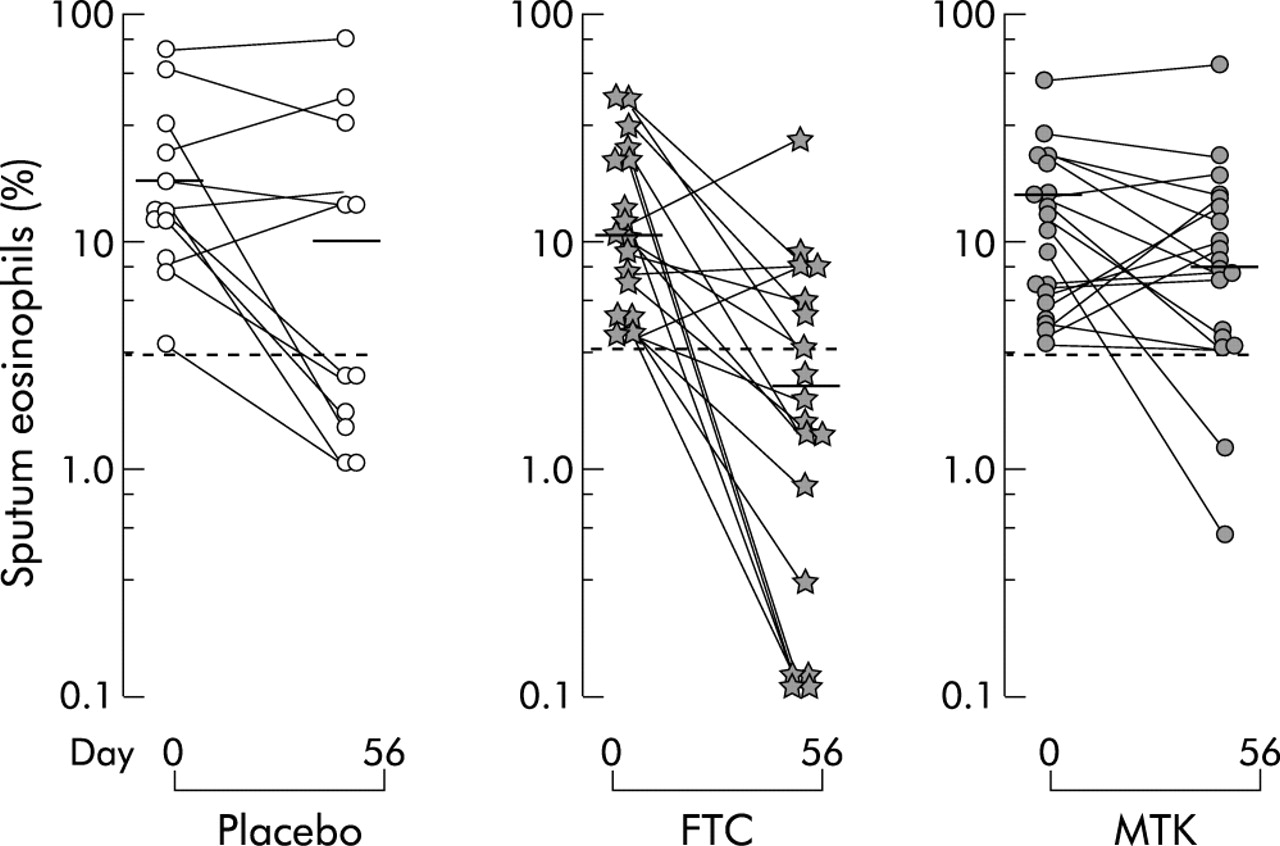
Individual plots of percentage sputum eosinophils at day 0 and at the end of the treatment period (day 56) with placebo, fluticasone (FTC) and montelukast (MTK). At the end of the study fluticasone treatment significantly reduced sputum eosinophils while treatment with placebo or montelukast did not.
{kind=link}
{kind=link}
{kind=link}
{kind=link}
Effects of treatment with fluticasone (stars), montelukast (closed circles), and placebo (open circles) on pre-bronchodilator FEV1. Fluticasone treatment produced a significant increase in FEV1 as early as day 7 which was maintained throughout the study. Montelukast treatment had no effect on FEV1.
Side effects
One subject who was previously well apart from asthma, and who had no alcohol intake and normal baseline serum liver function tests, developed evidence of a drug induced hepatitis after 2 months of treatment with montelukast. The bilirubin and aspartate transaminase, which were previously normal, rose to 30 mmol/l and 62 U/l, respectively, at the final visit and fell to normal levels 3 weeks after the drug was discontinued.
DISCUSSION
In this study we have examined repeatedly at different time points the anti-inflammatory effects of fluticasone and montelukast on the airway eosinophilic inflammation of subjects with steroid naive asthma. The results show that treatment with fluticasone suppresses sputum eosinophils and significantly improves FEV1. These effects of fluticasone were observed by 7 days and were maintained during the 8 weeks of the study. Treatment with montelukast attenuated and had its greatest effect on airway eosinophilia by day 7. However, in contrast to fluticasone, the effect only lasted 4 weeks. In addition, montelukast had no effect on FEV1. Placebo treatment did not affect sputum eosinophilia or improve FEV1. These results are relevant to the treatment of asthma with sputum eosinophilia in patients who are not receiving inhaled steroids, but not to similar patients without sputum eosinophilia.
This is the first study to compare repeatedly at several time points the anti-inflammatory effects of a low dose of fluticasone with montelukast in symptomatic steroid naive asthmatics with airway eosinophilia in a placebo controlled study. The results are consistent with other published observations that have shown that leukotriene modifiers, including montelukast, reduce eosinophilic airway inflammation18,19 and that inhaled steroids, including fluticasone, suppress it.34,36,37 The failure of fluticasone to completely suppress sputum eosinophilia during the 8 weeks of the study in six of 18 subjects indicates that some patients may require a higher steroid dose. The novel and unexpected finding was a non-sustained anti-inflammatory effect of montelukast at 8 weeks. This is intriguing and questions the use of montelukast as an alternative anti-inflammatory treatment to inhaled steroid in mild persistent asthma, as suggested by one asthma guideline.2 The inability of montelukast to maintain a clinically important attenuation of airway eosinophilia at 8 weeks of treatment in the present study does not seem to be due to compliance, nor does it seem to be due to a placebo response or to sample size since this was based on the results of an earlier study when montelukast had a sputum eosinophil lowering effect.18 The explanation is uncertain. The possibilities are that the anti-inflammatory effect is too selective or weak or that the dose used, although regarded to give maximal effects, is not enough to prevent further increases in airway eosinophilia due to various stimuli.
This study is also the first to show that low dose fluticasone is more effective than montelukast for controlling sputum eosinophilia in steroid naive asthma. The only other study to compare the effects did not select subjects with sputum eosinophilia or include a placebo control.27 It failed to show a difference in the effects of fluticasone and montelukast on sputum eosinophils and failed to show an anti-inflammatory effect of montelukast on eosinophils after 4 weeks of treatment. Possible explanations for the different results in the latter study include the lack of selection of asthmatics with airway eosinophilia so that there was not enough signal to demonstrate an anti-inflammatory effect,34 or the variable washout period of 3–6 weeks between treatment phases of a crossover design.
The design of the present study has several strengths. One of these is the placebo arm which excludes the regression to the mean as the cause of changes in airway inflammation.38 Another strength is the selection of a homogenous population of patients with eosinophilic inflammation to enable a clear signal of anti-inflammatory effects of the drugs to be shown on sputum eosinophils. However, by selecting our patients we decreased the generalisability of the results to patients with symptomatic asthma who have no eosinophilia. The prevalence of symptomatic non-eosinophilic asthma (sputum eosinophils <2%) in a large population of steroid naive asthma is uncertain. It has been reported to occur in approximately 35–40% of the patients presenting in tertiary clinics.39,40 On the other hand, the lack of selection of homogenous groups of subjects with asthma may help to explain the lack of the steroid response in clinical trials which has been reported to be as high as 40%.41
While there has been some recent controversy on the role of eosinophils in the pathogenesis of asthma,42,43 sputum eosinophilia is an important clinical marker of response to steroid treatment44,45 and the present results support this. The importance of suppressing airway eosinophilia has been further confirmed by two longitudinal studies which compared the monitoring of asthma treatment using sputum eosinophils with symptoms and FEV1.46,47 Both studies showed that the use of sputum cell counts decreased the exacerbation rates by at least 50% without the need for an increase in inhaled steroid treatment.
The present study also showed an improvement in clinical indices of asthma with fluticasone, as indicated by improvement in symptoms, rescue salbutamol, and FEV1. The same was not observed in the group of subjects on montelukast. Although these results differ from previous publications which show that montelukast has bronchodilator48 and bronchoprotective49 properties and, despite the sample size, had not been estimated for this outcome, the present results are in keeping with our previous publication.18 The greater improvement in FEV1 caused by inhaled steroid over antileukotriene receptor antagonists has been seen in other studies.25,26,31 In one of these, Busse et al25 found that the addition of low dose fluticasone 88 μg twice daily for 24 weeks to albuterol alone in 533 symptomatic patients improved FEV1, morning and evening PEF, symptom free days, and albuterol use more than montelukast. However, montelukast is an active drug and seems to be effective in some patients. The challenge is to identify how to predict which patients will receive treatment benefit.
We conclude that fluticasone treatment is more effective than montelukast in symptomatic steroid naive adults with asthma who have sputum eosinophilia and who would be expected to improve with steroid treatment. This should question the advisability of using montelukast as first line treatment in these patients. However, the effect of montelukast in symptomatic steroid non-eosinophilic asthma was not studied and still requires investigation.
Acknowledgments
The authors thank the subjects who participated in the study; A Efthimiadis, S Carruthers, S Weston, M Prodaniuk and S Ferreira for performing the sputum cell counts; and P Hussack, S Goodwin, S Chaboillez, M Langevin and Julie Cristina Nunes for performing the clinical procedures.
REFERENCES
Footnotes
-
This study was partially supported by a medical school grant from Glaxo Wellcome Inc; L Jayaram was supported by a Fellowship from Boehringer Ingelheim (Canada) Inc; F E Hargreave is supported by the Father Sean O’Sullivan Research Centre.
Linked Articles
- airwaves