Article Text

Abstract
Background Two distinct, stable inflammatory phenotypes have been described in adults with asthma: eosinophilic and non-eosinophilic. Treatment strategies based on these phenotypes have been successful. This study evaluated sputum cytology in children with asthma to classify sputum inflammatory phenotypes and to assess their stability over time.
Methods Sputum induction was performed in 51 children with severe asthma and 28 with mild to moderate asthma. Samples were classified as eosinophilic (>2.5% eosinophils), neutrophilic (>54% neutrophils); mixed granulocytic (>2.5% eosinophils, >54% neutrophils); or paucigranulocytic (≤2.5% eosinophils, ≤54% neutrophils). Sputum induction was repeated every 3 months in children with severe asthma (n=42) over a 1-year period and twice in mild to moderate asthma (n=17) over 3–6 months.
Results 62 children (78%) had raised levels of inflammatory cells in at least one sputum sample. In the longitudinal analysis 37 of 59 children (63%) demonstrated two or more phenotypes. Variability in sputum inflammatory phenotype was observed in both the severe and the mild to moderate asthma groups. Change in phenotype was not related to change in inhaled corticosteroid (ICS) dose or asthma control, nor was it reflected in a change in exhaled nitric oxide (FENO). 24 children (41%) fulfilled the criteria for non-eosinophilic asthma on one occasion and eosinophilic on another. There were no differences in severity, asthma control, atopy, ICS dose or forced expiratory volume in 1 s between those who were always non-eosinophilic and those always eosinophilic.
Conclusion Raised levels of inflammatory cells were frequently found in children with asthma of all severities. Sputum inflammatory phenotype was not stable in children with asthma.
- Sputum eosinophil counts
- inflammatory phenotype
- eosinophilic
- non-eosinophilic
- children
- COPD mechanisms
- cough/mechanisms/pharmacology
- allergic lung disease
- respiratory measurement
- lung physiology
- asthma pharmacology
- asthma
- exhaled airway markers
- paediatric asthma
- bronchoscopy
- cystic fibrosis
- innate immunity
- paediatric lung disease
- paediatric physician
- respiratory infection
- viral infection
- asthma guidelines
- lung physiology
Statistics from Altmetric.com
- Sputum eosinophil counts
- inflammatory phenotype
- eosinophilic
- non-eosinophilic
- children
- COPD mechanisms
- cough/mechanisms/pharmacology
- allergic lung disease
- respiratory measurement
- lung physiology
- asthma pharmacology
- asthma
- exhaled airway markers
- paediatric asthma
- bronchoscopy
- cystic fibrosis
- innate immunity
- paediatric lung disease
- paediatric physician
- respiratory infection
- viral infection
- asthma guidelines
- lung physiology
Key messages
What is the key question?
Are eosinophilic and non-eosinophilic sputum inflammatory phenotypes, as described in adults with asthma, stable in children with a range of asthma severity?
What is the bottom line?
Sputum inflammatory phenotype was not stable in 61% of children in this study
Why read on?
This is the first study to assess sputum inflammatory phenotype longitudinally in children with asthma using accepted definitions of eosinophilic and non-eosinophilic asthma.
Introduction
The term ‘asthma’ encompasses a spectrum of disorders which may be managed very differently. It is increasingly recognised that a single therapeutic approach for all children with asthma is unlikely to be successful.1 ,2 Phenotyping children with asthma has the potential to provide therapeutic targets and a more individualised management approach.
The emergence and increasing availability of validated, feasible non-invasive measures of inflammation has led to a greater understanding of inflammatory phenotypes, particularly in adults. Two distinct and apparently stable sputum inflammatory phenotypes have been described, eosinophilic and non-eosinophilic,3–6 which have a differential treatment response, particularly to steroids.6 ,7 The classification has been further refined as eosinophilic, neutrophilic, mixed granulocytic (raised eosinophils and neutrophils) and paucigranulocytic (normal levels of eosinophils and neutrophils).8 There are limited data on phenotype stability, however short-term and long-term (up to 5 years) stability of sputum inflammatory phenotype has been reported in two adult studies.8 ,9
It has been suggested that phenotype driven treatment in childhood asthma may be beneficial.10–12 Most of the work that has been published on sputum inflammatory phenotypes in paediatric asthma is based on cross-sectional data13–15 and there are few longitudinal data, particularly in severe asthma, the group most likely to benefit from phenotyping.16 We hypothesised that evidence of inflammation would be found more frequently in children with severe asthma compared with those with mild to moderate asthma and that paediatric sputum inflammatory phenotypes, as described in adults with asthma would be stable. We studied sputum cellular phenotypes in children with severe asthma and compared the findings with a group of children with mild to moderate asthma.
Methods
Subjects
Two groups of school-aged children with asthma were recruited. The first group were subjects recruited for a previously reported randomised controlled trial comparing a management strategy aimed at controlling sputum eosinophils with a conventional symptom-based strategy.17 These children had severe asthma, diagnosed after detailed evaluation by a paediatric respiratory physician and requiring treatment at step 4 or 5 of the British Thoracic Society/Scottish Intercollegiate Guidelines Network guidelines.18 Data from all children enrolled in the trial who produced at least one sputum sample are included in this study.
The second group were children with mild to moderate asthma, diagnosed by a paediatric respiratory physician, prescribed ≤400 μg fluticasone propionate or equivalent per day. They were recruited solely for the purposes of this study as a comparison group. Both groups were recruited from the Outpatient Department at the Royal Brompton Hospital between December 2005 and February 2008. Children were excluded if they were currently prescribed an immunomodulatory steroid sparing agent (ciclosporin, methotrexate or azathioprine) or a continuous infusion of subcutaneous terbutaline, or had received intramuscular triamcinolone in the previous 3 months, or had another significant chronic respiratory or medical condition.
Study design
Children with severe asthma were seen during four routine clinic visits every 3 months and children with mild–moderate asthma during two routine clinic visits 3–6 months apart.
The study was approved by the Royal Brompton Hospital Ethics Committee. Carers gave informed written consent and children gave age-appropriate assent.
Study procedures
Baseline spirometry was performed using a portable spirometer (Compact Vitalograph Ltd, Buckingham, UK) using at least three reproducible forced expiratory manoeuvres to measure first second forced expired volume in 1 s (FEV1) and forced vital capacity in accordance with American Thoracic Society (ATS)/European Respiratory Society (ERS) guidelines.19 Sputum induction was performed using a DeVilbiss 2000 Ultrasonic nebuliser (Somerset, Pennsylvania, USA), and inhalation of hypertonic (3.5%) saline as previously described.14 Prior to sputum induction a dose of 1000 μg of salbutamol (10 puffs) was administered by a metered dose inhaler through a spacer to ensure safety of the procedure.14 Subjects with a post-bronchodilator FEV1 <65% predicted or previous adverse event with hypertonic saline underwent induction with normal (0.9%) saline.
Selected sputum plugs were processed as previously reported.20 Differential cell counts were determined by assessment of 400 viable, non-squamous cells on Reastain Quick-Diff stained cytospins (Reastain Reagena Ltd. Toivala, Finland). The counts were performed by an investigator blind to the identity and clinical status of the subjects.
Asthma control at the time of each study visit was assessed using the asthma control test (ACT), which assesses control in the preceding 4 weeks. Scores of 5–25 may be attained, with higher scores indicating better control.21
Atopy was defined as one or more positive skin prick tests (wheal ≥3 mm) or serum specific IgE ≥0.34 kU/litre to a standard panel of six aeroallergens.
Exhaled nitric oxide (FENO) was measured using an online single breath chemiluminescence analyser (NIOX, Aerocrine, Stockholm, Sweden) at a flow rate of 50 ml/s according to published ATS/ERS guidelines.22
Definition of sputum inflammatory phenotypes
The sputum inflammatory phenotype was categorised according to the classification described by Simpson et al8 and the cut points were based on previously published paediatric definitions and ranges for sputum differential cell counts (table 1).13 ,23
Definitions of inflammatory phenotype according to sputum differential eosinophil % and neutrophil %
Statistical analysis
A power calculation based on the proportion of subjects with severe asthma with elevated inflammatory cells at baseline showed that we needed 40 subjects in each group to show a 50% reduction in the proportion of children in the mild to moderate group with evidence of inflammation (α=0.05; β=0.2).24 Comparison of demographic data between the severe and mild to moderate groups was made using the Student t test or the Mann–Whitney U test for non-parametric values. Comparison of proportions between groups was performed using the Pearson χ2 test or Fischer's exact test. The analysis of variance (ANOVA) or the Kruskal–Wallis test for non-parametric values was used to compare the all eosinophilic, all non-eosinophilic and both eosinophilic and non-eosinophilic groups and the factors influencing phenotype change. If a significant difference was found a post-test comparison between each pair was made using the Bonferroni correction following the ANOVA and Dunn's test following the Kruskal–Wallis test. Stability of eosinophil and neutrophil counts was assessed using intraclass correlation coefficients (ICCs). An ICC was obtained for single measures (the stability of an individual measurement) and average measures (the stability of a measurement relative to all measures in that individual). Results were considered significant when p<0.05. All analyses were carried out using GraphPad Prism V.5 other than the ICC calculations, which were carried out using SPSS (V.18).
Results
Baseline data
Fifty-five children with severe asthma and 35 children with mild to moderate asthma were recruited (figure E1 in online supplement). Seventy-nine children produced at least one sputum sample (51 with severe asthma and 28 with mild to moderate asthma). Their demographics are shown in table 2.
Demographics of the severe asthma and mild to moderate asthma cohorts
At baseline, 49 children (62%) had raised levels of inflammatory cells (eosinophils or neutrophils). The inflammatory phenotype at baseline for subjects in each of the cohorts is shown in table 3. Neither the levels of eosinophils and neutrophils nor the distribution of phenotypes was significantly different between the groups. Over the course of the study 62 children (78%) had raised levels of inflammatory cells on at least one occasion. The distribution of phenotypes for all 197 samples is shown in table E1 of the online supplement.
Inflammatory cells and phenotypes at baseline
Longitudinal data
Fifty-nine children produced two or more evaluable sputum samples and are included in the longitudinal analyses (42 children with severe asthma and 17 with mild to moderate asthma). In total, 177 samples were obtained. Eleven of the children with severe asthma produced three samples and 24 produced four samples.
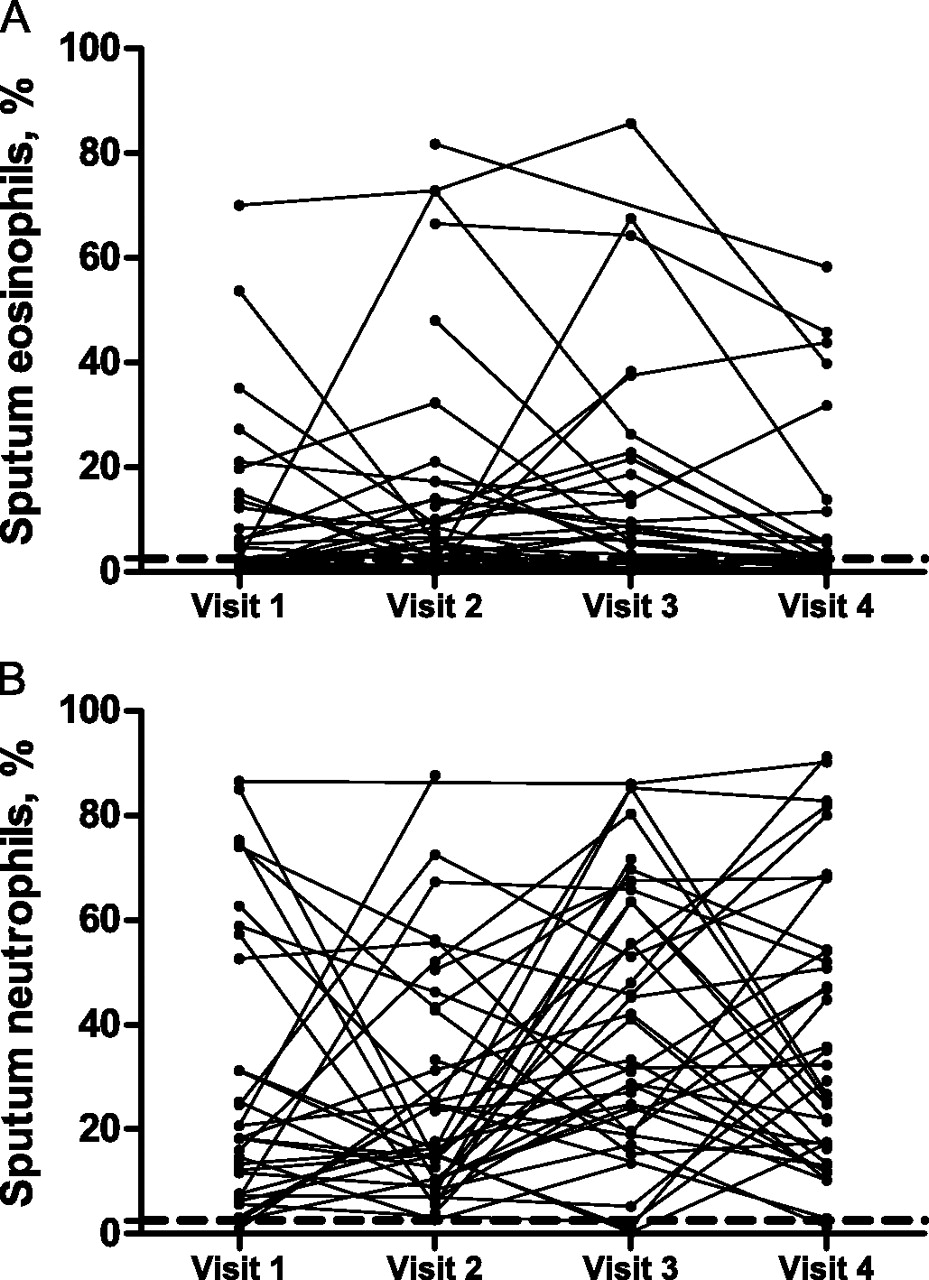
The changes in sputum eosinophil and neutrophil counts over the duration of the study for the severe and mild to moderate asthma cohorts are shown in figures 1 and 2. The ICC (95% CI) for eosinophils (single measures) was 0.183 (0.041 to 0.364), p=0.05 and for neutrophils 0.275 (0.082 to 0.515), p=0.02. The ICC for eosinophils (average measures) was 0.472 (0.145 to 0.696), p=0.05 and neutrophils 0.602 (0.262 to 0.810), p=0.02. These results indicate poor reliability of single measurements; however the reliability improves with repeated measures.

Changes in sputum eosinophils (A) and neutrophils (B) over the duration of the study in the severe asthma group. The dotted line denotes the 2.5% cut-off point for sputum eosinophils and the 54% cut-off point for neutrophils.

Changes in sputum eosinophils (A) and neutrophils (B) over the duration of the study in the mild to moderate asthma group. The dotted line denotes the 2.5% cut-off point for sputum eosinophils and the 54% cut-off point for neutrophils.
Eosinophilic and non-eosinophilic phenotypes
In the severe asthma cohort 10 of 42 (24%) children had elevated levels of sputum eosinophils in all sputum samples (eosinophilic or mixed phenotypes) and 12 (29%) always demonstrated one of the non-eosinophilic phenotypes (paucigranulocytic, n=8 or neutrophilic, n=1). The remaining 20 children (48%) demonstrated one of the eosinophilic phenotypes on at least one occasion and one of the non-eosinophilic phenotypes on another (see figure E2, of the online supplement). In the mild to moderate cohort 8 of 17 (47%) were always non-eosinophilic, 5 of 17 (29%) were always eosinophilic and 4 of 17 (24%) demonstrated an eosinophilic phenotype in one sample and non-eosinophilic in another. These proportions were not significantly different between the groups. A comparison between children who were always eosinophilic, always non-eosinophilic and those who showed both phenotypes is shown in table 4. Subjects in the non-eosinophilic group were significantly younger than those in the eosinophilic group. In post-test analysis there was no significant difference in FENO levels between the eosinophilic and non-eosinophilic groups. No other significant differences were found between these two groups in terms of asthma severity, inhaled corticosteroid (ICS) dose, atopic status, FEV1 and asthma control at baseline.
Comparison of children with all eosinophilic sputum samples, all non-eosinophilic sputum samples and those with eosinophilic and non-eosinophilic samples
Table E2 of the online supplement shows the changes in phenotype for both cohorts. In total, 22 of 59 (37%) children always had the same phenotype, 17 of 59 (29%) varied between one of the inflammatory phenotypes and the paucigranulocytic phenotype and 20 of 59 (34%) demonstrated two or more inflammatory phenotypes. There was marked variability in eosinophils and particularly neutrophils leading to these changes (figure E3, online supplement).
The change in phenotype between two consecutive visits was compared to change in ICS dose between those visits (figure 3). The phenotype change did not appear to be influenced by changes in the prescribed doses. Changes in phenotype were not associated with changes in FENO nor were they reflected in changes in asthma control as measured by the ACT (figures E4 and E5, online supplement).

{kind=link}
{kind=link}
{kind=link}
Scatter plot showing the change in dose of fluticasone propionate (FP) (μg/day) for each phenotype change. The phenotype observed first is shown above the plots and the phenotype observed at the subsequent visit is shown below the x axis. The horizontal bar through each plot represents the group median. Comparison between the groups was made using the Kruskall–Wallis test. There was no significant difference between the groups. This figure is produced in colour in the online journal—please visit the website to view the colour figure.
Discussion
To our knowledge, this is the first study to report the findings of sequential sputum analysis in children across a range of asthma severity. There were no differences in sputum cellularity between the mild to moderate and severe asthma groups. Sputum cellularity was found to be highly variable in children with asthma and there were changes in sputum inflammatory phenotype in almost two-thirds of the children over the duration of the study. Phenotype variability did not differ by severity of asthma and did not relate to changes in asthma control or prescribed dose of ICS. Those who were persistently eosinophilic or non-eosinophilic did not differ in terms of severity, ICS dose, atopy, FEV1 or asthma control.
Short-term and long-term inflammatory phenotype stability has been reported in adult studies.8 ,9 However, these studies were based on only two sequential sputum samples, and more recently, variability in sputum eosinophil and neutrophil counts have been reported in adults with asthma undergoing frequent (up to monthly) sputum induction over a 1-year period as part of the Severe Asthma Programme.25 The lack of phenotype stability in our cohort of patients is a novel finding in children with asthma.
There are a number of potential confounding factors which need to be considered. During the observation period the children in this study experienced variation in clinical control and ICS dose, which could have accounted for some of the changes seen. Furthermore, it is also acknowledged that some of the children in the severe asthma cohort had treatment changes made on the basis of sputum cellularity. However, if only those managed according to conventional symptom-based management are analysed, the findings are the same. Sputum eosinophils are known to fall in response to an increase in ICS dose.26 ,27 Changes in ICS dose could therefore account for subjects varying between one of the eosinophilic phenotypes and the non-eosinophilic phenotypes. This was not found to be the case, and of note, changing from the paucigranulocytic to the eosinophilic phenotype was never associated with a decrease in ICS dose. A previous adult study reported changes in phenotype in subjects with asthma who restarted fluticasone following steroid withdrawal.28 The neutrophilic phenotype was absent after steroid withdrawal and the proportion of sputum neutrophils increased after restarting ICS. The authors suggested that inflammatory phenotypes may be misclassified in patients receiving ICS. It is interesting that those with mild to moderate asthma in our study were actually more likely to be neutrophilic and had higher neutrophil counts than those with severe asthma despite being prescribed significantly lower ICS doses. However, these observations need to be interpreted cautiously. We accept that adherence in children with asthma is poor29 and that these are the prescribed doses of ICS and may not be the actual dose taken. Prescription uptake in this study was <80% in over half of the severe asthma group for whom prescription records were available. This is a major limitation in determining the extent to which ICS influence phenotype. To determine whether changes in ICS dose influence phenotype change, future studies should include the use of an electronic device to record how much ICS is actually taken.
Changes in sputum cytology may also be as a consequence of changes in asthma control. Zacharasiewicz et al observed that children who remained stable during ICS reduction maintained low levels of eosinophils and those who experienced a loss of asthma control had an increase in sputum eosinophil level.30 However, in this study changes in phenotype were not reflected in changes in current symptoms as measured by the ACT score nor were they associated with a recent acute exacerbation requiring high-dose oral corticosteroids.
It is possible that other exogenous factors were responsible for phenotype changes, such as seasonal variation in allergen exposure or the presence of a viral infection. Although no associations were found with viral colds in the 2 weeks before sputum induction, the definition of a cold was based on self-report and this analysis would have been more robust if viral detection studies had been undertaken. Furthermore, an increase in allergen burden might be expected to lead to an elevation in FEno,31 but this was not associated with a phenotype change.
Multiple inflammatory phenotypes were more commonly observed in those with severe asthma. It could be speculated that these changes are part of what drives the asthma severity and why conventional therapy fails in this group of patients. However, it is more likely that the greater variability in those with severe asthma was due to the fact that more samples were collected in this group over a longer time period. When only the first two sputum samples were compared, the mild to moderate group were as likely to change phenotype as the severe group. Further comparison between the groups is made difficult by the different number of sputum samples and the frequency with which they were collected and the smaller numbers in the mild to moderate group. In the severe asthma cohort, the greater the number of sputum samples collected, the more likely the observation of phenotype change. It is possible that if four or more samples had been collected from every subject, even greater variability in sputum inflammatory phenotype may have been observed in both groups. It is possible that there is week by week or even day by day variability in sputum cytology. Regular sputum sampling would help to address some of these issues, although this is unlikely to be practical in children.
The levels of eosinophils and neutrophils used to determine the cut points for each of the phenotypes are based on those previously published to describe sputum inflammatory phenotypes in children.13 ,14 The cut point for sputum eosinophils (2.5%) is based on the 95% CI of the mean from a group of 72 normal controls23 and has been recommended as the upper limit of normal for sputum eosinophilia in children.32 ,33 Adult studies have used other cut points for defining sputum eosinophilia, including 1.9%3 ,34 and 3.0%.35 The normal range for sputum neutrophils in children is more difficult to establish due to the paucity of published data using normal controls. The 54% limit is based on a previously published definition of neutrophilic asthma in children13 and has been used in a subsequent paediatric study.14 In adult studies limits of 61%34 and 65.3%3 have been used to define the neutrophilic phenotype. However, the phenotype changes observed in our study were generally the result of large variations in inflammatory cells, rather than small changes around the cut points (figure E3, online supplement). Only nine samples (5%) would be reclassified if a neutrophil level of 61% was used and an additional four if the cut point was increased to 65.3%. However, it should be stressed that the aim of this study was not to re-define the cut points for inflammatory phenotypes but to assess whether accepted models for adults with asthma (ie, eosinophilic and non-eosinophilic phenotypes) are applicable to children with asthma.
Raised levels of sputum inflammatory cells, particularly eosinophils, were a more common finding than previously reported in cross-sectional paediatric asthma studies.14 ,36–38 and did not differ between the two groups. A surprising finding was that the mild to moderate group had higher sputum neutrophil levels at baseline despite significantly lower ICS doses. This is contrary to the previously discussed findings of Cowan and co-workers.28 However, further interpretation is made difficult without accurate adherence data. In adult asthma cohorts, patients with non-eosinophilic phenotypes, in particular neutrophilic asthma, are more likely to be non-atopic, women and have a poor response to ICS.3 ,39 Neutrophil levels in those studied longitudinally in our study were highly variable and only three children had persistently elevated neutrophils. There were some differences between children with eosinophilic and non-eosinophilic phenotypes but not in terms of atopy, sex or asthma severity. Those with persistent sputum eosinophilia had higher levels of FENO at baseline. Interestingly, those who were intermittently eosinophilic had the lowest FENO levels and the difference between the persistently eosinophilic and persistently non-eosinophilic groups was non-significant. Those who were consistently non-eosinophilic were younger, however this is in part due to the slight preponderance of children with mild to moderate asthma in this group and when only the severe asthma cohort was analysed there was no significant difference in age. However, the fact that 39% of all children in this study, and nearly half of the severe asthma cohort, fitted both definitions of eosinophilic and non-eosinophilic asthma at different time points, makes meaningful classification difficult. It is possible that clearer inflammatory phenotypes may emerge from a cluster or other mathematical analysis of a larger number of children with asthma and further work is needed to assess how these phenotypes relate to treatment response and outcome.
It is clear that a single sputum sample does not necessarily determine the phenotype of subsequent samples. It has been suggested in adults that a low sputum eosinophil count on at least two occasions is reasonable for defining non-eosinophilic asthma.40 In two recent therapeutic studies of anti-interleukin (IL)-5 only adults with severe, eosinophilic asthma were enrolled.41 ,42 Haldar and co-workers included all those who had ever had raised sputum eosinophils in the previous 2 years41 whereas Nair and co-workers included those with sputum eosinophilia at the baseline visit.42 Both studies demonstrated a reduction in exacerbations, suggesting that for adults with asthma a single sputum sample in those with refractory asthma is a good reflection of the baseline inflammatory phenotype. Interestingly, the benefit appeared to be greater in the study which required sputum eosinophilia at entry,42 ,38 and one could speculate that some of Haldar et al's patients had in fact undergone a phenotype change.41 However, in children it is clear that a single sputum sample provides only limited information and a child's eligibility for this sort of study would vary greatly if based only on a sputum sample collected at the screening visit.
It is possible that in childhood asthma sputum eosinophils, even if present, are not reflective of the true underlying inflammatory phenotype. The absence of sputum eosinophils does not preclude the presence of distal airway inflammation.43 ,44 Furthermore, it has been demonstrated in children that sputum eosinophils relate to broncho-alveolar lavage eosinophils but not mucosal eosinophils.37 There are a number of other biomarkers which may be of greater utility, for example the pattern of broncho-alveolar lavage inflammatory cytokines has been used to identify phenotypes of severe asthma in adults.45 There are a number of lines of evidence for different underlying mechanisms for adults with eosinophilic and non-eosinophilic asthma. Differential proteolytic enzyme activity has been described in eosinophilic asthma compared with neutrophilic asthma, suggesting that there could be different levels of repair and remodelling between phenotypes leading to different clinical and physiological manifestations.46 Those with high levels of neutrophils have been found to have increased expression of innate immune receptors and IL-8, suggesting activation of the innate immune system.34 Viral infections, bacteria and pollutants are important in activating these mechanisms.47 ,48 Furthermore, confounding factors such as corticosteroid treatment may lead to phenotype misclassification. Future studies investigating inflammatory phenotypes need to control for the possible exogenous factors influencing phenotype. Further work is needed to evaluate possible mechanisms and their influence on inflammatory phenotype.
In summary, the data reported demonstrate that inflammation in induced sputum is a frequent but by no means invariable finding in children across a range of asthma severity and that patterns of inflammation are not stable. This study also highlights the complexity of defining inflammatory phenotypes in children with asthma. These findings need to be considered when designing future paediatric studies targeting airway inflammation.
Acknowledgments
We would like to thank all the children and their parents who participated in the study and the staff in the Paediatric Respiratory Department at the Royal Brompton Hospital who supported this study, in particular Drs Ian Balfour-Lynn, Mark Rosenthal and Claire Hogg.
References
Supplementary materials
Supplementary Data
This web only file has been produced by the BMJ Publishing Group from an electronic file supplied by the author(s) and has not been edited for content.
Files in this Data Supplement:
- Download Supplementary Data (PDF) - Manuscript file of format pdf
- Download Supplementary Data (PDF) - Manuscript file of format pdf
Footnotes
LF and LT are joint first authors.
Funding The study was funded by a grant from the British Lung Foundation.
Competing interests None.
Patient consent Obtained.
Ethics approval Ethics approval was approved by Royal Brompton Hospital Ethics Committee.
Provenance and peer review Not commissioned; externally peer reviewed.
Linked Articles
- Editorial
- Airwaves