Article Text

Abstract
Background Although women with severe non-allergic asthma may represent a substantial proportion of adults with asthma in clinical practice, gender differences in the incidence of allergic and non-allergic asthma have been little investigated in the general population.
Methods Gender differences in asthma prevalence, reported diagnosis and incidence were investigated in 9091 men and women randomly selected from the general population and followed up after 8–10 years as part of the European Community Respiratory Health Survey. The protocol included assessment of bronchial responsiveness, IgE specific to four common allergens and skin tests to nine allergens.
Results Asthma was 20% more frequent in women than in men over the age of 35 years. Possible under-diagnosis of asthma appeared to be particularly frequent among non-atopic individuals, but was as frequent in women as in men. The follow-up of subjects without asthma at baseline showed a higher incidence of asthma in women than in men (HR 1.94; 95% CI 1.40 to 2.68), which was not explained by differences in smoking, obesity or lung function. More than 60% of women and 30% of men with new-onset asthma were non-atopic. The incidence of non-allergic asthma was higher in women than in men throughout all the reproductive years (HR 3.51; 95% CI 2.21 to 5.58), whereas no gender difference was observed for the incidence of allergic asthma.
Conclusions This study shows that female sex is an independent risk factor for non-allergic asthma, and stresses the need for more careful assessment of possible non-allergic asthma in clinical practice, in men and women.
- Sex
- asthma
- atopy
- diagnosis
Statistics from Altmetric.com
Key messages
What is the key question?
Are women really at increased risk of asthma, and what could explain this difference?
What is the bottom line?
Women were found to be at increased risk of developing non-allergic asthma (no difference was found for allergic asthma), and this increased risk was not explained by differences in diagnosis, lung function (as a surrogate of airway calibre), obesity or smoking.
Why read on?
Our data provide evidence that non-allergic asthma is still poorly recognised in men and women, and that women are at increased risk of developing non-allergic asthma compared with men. We suggest that sex hormones or other biological markers that significantly differ between men and women (such as adipocytes) may be involved in the development of non-allergic asthma.
Introduction
The prevalence of asthma shows a sex reversal around puberty from a higher risk in boys early in life to a higher risk in girls after adolescence.1–6 This pattern has raised several hypotheses about the susceptibility to asthma of men and women, such as an effect of sex hormones, airway calibre, obesity, differences in exposure or diagnosis.1–6 Further studies are needed to appraise how much these determinants could explain the higher risk of asthma in women. Data are lacking on whether women remain at increased risk of asthma throughout all the reproductive years, and few studies have investigated the possibility of a differential diagnosis.2–8 Furthermore, most studies are not of a prospective nature that allows separating new-onset asthma from persistent asthma or relapse. In addition, new-onset of non-allergic asthma appears to be relatively frequent in adulthood.9 Clinical studies suggest that non-allergic (or ‘intrinsic’) asthma may be more severe and difficult to control than allergic asthma, and that women might be at increased risk of non-allergic asthma.10–14 However, most of our knowledge on non-allergic asthma comes from clinical studies which often include patients with more severe asthma, and little is known on non-allergic asthma in the general population.14
We used data collected as part of the European Community Respiratory Health Survey (ECRHS) to estimate gender differences in the prevalence of asthma according to age; appraise possible differences in asthma diagnosis; prospectively investigate gender differences in the remission/persistence of asthma; and assess gender differences in the risk of new-onset asthma, accounting for potential confounders and considering allergic and non-allergic asthma separately, within the age range 20–55 years.
Methods
Study design
The analysis is based on data collected in 29 centres from 14 countries as part of the ECRHS. The protocol and participation rates have been described elsewhere.15–17 Briefly, between 1991 and 1993, each participating centre randomly selected about 1500 men and 1500 women, representative of the age group 20–44 years, to answer a postal questionnaire (European Community Respiratory Health Survey I [ECHRS-I] stage 1; ‘screening’). A 20% random sample of respondents was then invited to a clinical investigation (ECHRS-I stage 2). Participants in stage 2 were eligible for the follow-up survey in 1998–2002 (ECRHS-II). At ECHRS-I stage 2 (‘baseline’) and follow-up, the protocol included assessment of respiratory symptoms via questionnaire and measurements of bronchial responsiveness and IgE specific to four common allergens. In each centre, the protocol was approved from the appropriate ethics committee, and written consent was obtained from each participant.
Analysis
Doctor-diagnosed asthma was defined as a positive answer to the questions ‘Have you ever had asthma?’ and ‘Was this confirmed by a doctor?’ Because only specific IgEs were assessed at follow-up, the main analysis was conducted with atopy defined as specific IgE≥0.35 kU/litre to any of the four common allergens tested. In a sensitivity analysis, atopic status was defined according to specific IgE and skin test reactivity measured at the baseline survey for nine common allergens. Atopic subjects with asthma were considered to have ‘allergic asthma’. Further details including cross tables are provided in the online supplement. All the analyses were conducted in Stata V.8 (StataCorp 2001).
Results
Gender differences in asthma prevalence and diagnosis
Participation of men and women at each step of the survey is described in the online supplement.
Prevalence
At ECRHS-I stage 1 (table 1, first column), large representative samples were screened to estimate asthma prevalence.15 There was no gender difference in the prevalence of asthma from age 20 to 35 years. However, women had a 20% higher risk of asthma than men after age 35 years. This pattern of results was consistent across the participating centres, despite large geographical variations in the prevalence of asthma.
Prevalence of asthma in representative samples of men and women screened for asthma at ECRHS-I, and in men and women participating in ECHRS-I, stage 2 (1991–1993) and ECHRS-II (1998–2002)
To assess whether the magnitude of the gender difference had changed over time, we considered prevalence at ECRHS-II. Although the prevalence of asthma was higher at ECRHS-II, within each age-group the ORs for the gender difference were remarkably similar at each survey, showing no difference before age 35 and a 20% higher risk of asthma in women in the age group 36–44 years (table 1, third column). The higher risk of asthma in women appears to be further marked after age 45 years (OR 1.68; 95% CI 1.24 to 2.29).
Investigating possible differential diagnosis
We considered data collected at ECRHS-I stage 2 (including bronchial hyperresponsiveness [BHR] assessment) to assess whether the higher prevalence of asthma in women could be explained by differences in diagnosis.
Besides diagnosed asthma, women were also more likely than men to have asthma-like symptoms or asthma-like symptoms and BHR (table 1 and online supplement).
Furthermore, among subjects with respiratory symptoms and BHR (table 2), the likelihood of having received a diagnosis of asthma decreased with increasing smoking and was higher in atopic than in non-atopic subjects. However, in each group, it was similar or even lower in women than in men. As shown in table 2, in non-atopic subjects, only 16% of those with asthma-like symptoms and BHR reported a diagnosis of asthma. However, this low rate of diagnosis was similar in women and in men.
Asthma diagnosis in men and women with asthma-like symptoms and bronchial hyperresponsiveness
No major gender difference was observed for asthma treatment, apart from a more frequent use of inhaled steroids in women (online supplement, table E2).
Gender differences in the natural history of asthma
Forty-three per cent of men and 63% of women with a current diagnosis of asthma from the doctor at follow-up reported asthma onset in adulthood (online supplement, table E2).
Asthma remission, persistence and relapse in subjects with asthma at baseline
Women with current asthma at baseline were as likely as men to still have asthma at follow-up (asthma persistence: 68.1% in 213 women vs 74.1% in 135 men; p>0.20).
In subjects who had ever had asthma before the baseline survey, but without ‘current’ asthma at baseline, women were as likely as men to have current asthma at follow-up (asthma relapse after remission: 21.2% in 189 women vs 18.0% in 178 men; p>0.30).
Asthma incidence
The risk of developing asthma over the follow-up was investigated in the 4281 women and 3956 men without asthma at baseline (figure 1). The asthma incidence rate was higher in women than in men (table 3). There was no interaction with age (p for interaction =0.13). At baseline, women more frequently reported rhinitis, respiratory infections in childhood and maternal asthma compared with men. Women less frequently had positive specific IgE to dust mites and grass, had lower total IgE and smoked less than men. Women had lower body mass index (BMI) than men at baseline and at follow-up, but the mean increase in BMI between the two surveys was slightly higher in women than in men. Adjustment for the subject's characteristics at baseline or follow-up had little effect on the gender difference in incidence (online supplement, table E3). The risk of developing asthma remained significantly higher in women than in men after adjustment for centre, maternal asthma, smoking, total IgE, atopic sensitisation, rhinitis, forced expiratory volume in 1 s (FEV1) and BMI at baseline (HR 1.94; 95% CI 1.40 to 2.68) as well as after additional adjustment for change in smoking status and change in BMI (HR 2.25; 95% CI 1.57 to 3.23). Further adjustment for occupational exposure over the follow-up to agents known to be related to occupational asthma did not change the estimate (HR 2.25; 95% CI 1.54 to 3.29).

Cumulative hazard function for new-onset asthma in men and women. The figures show the cumulative expected number of men and women developing asthma over follow-up, based on the Nelson–Aalen estimator using age as the time scale.
Incidence of asthma in women and men who reported they never had asthma at baseline
Incidence of allergic and non-allergic asthma
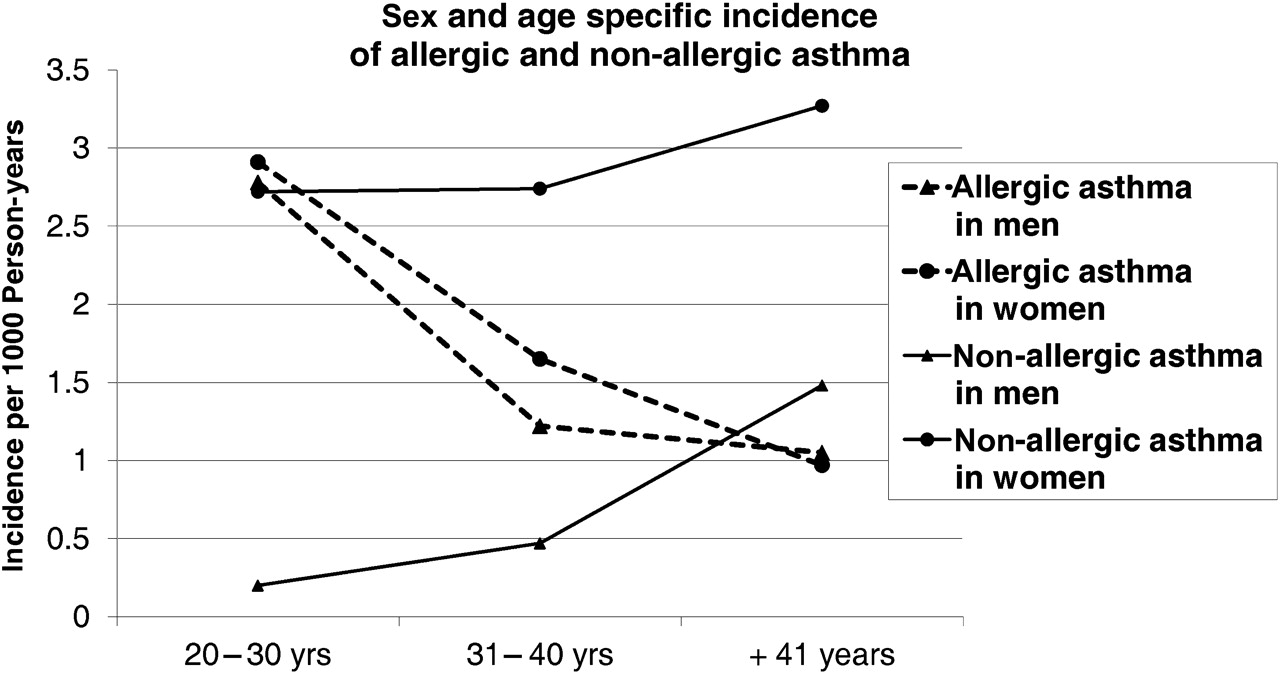
Women were at greater risk of developing non-allergic asthma than allergic asthma: 65% of the women with new-onset asthma had no atopic sensitisation at follow-up. In men, 37% of incident asthma cases were non-atopic. No gender difference was observed for the incidence of allergic asthma (p>0.60; table 3). In contrast, the incidence of non-allergic asthma was significantly higher in women than in men (HR 3.51; 95% CI 2.21 to 5.58; p<0.0001). In men, the incidence rate of non-allergic asthma remained very low until the age of 40 years and then increased to levels similar or slightly higher than that for allergic asthma (figure 2). In women, the incidence rate of non-allergic asthma was already relatively high between the ages of 20 and 30 years, and it remained high and significantly higher than that in men throughout all the reproductive years. A similar pattern of results was obtained in the sensitivity analyses, including the analysis using skin test results for the nine common allergens to define atopy (online supplement, tables E4–E6).
{kind=link}
{kind=link}
Sex and age-specific incidence rates for allergic and non-allergic asthma. The number of person-years at risk, within each age group, were respectively 5043, 10 696 and 11 451 in men, and 5152, 10 935 and 11 317 in women.
Discussion
In this large population-based cohort, the gender difference in the prevalence of asthma increased with increasing age and showed an increased risk of more than 20% in women than in men after age 35 years. The findings were consistent across the centres and during the two survey periods. Possible under-diagnosis of asthma appeared to be particularly frequent in non-atopic subjects, but was not more frequent in men than in women. In subjects without asthma at baseline, the risk of new-onset asthma over the follow-up was twofold higher in women than in men, and this was not explained by differences in smoking, lung function or obesity. More than 60% of the women with new-onset asthma were not sensitised to any of the allergens tested. The incidence of non-allergic asthma was significantly higher in women than in men throughout all the reproductive years, whereas no gender difference was observed for the incidence of allergic asthma.
Gender differences in non-allergic asthma
To our knowledge, this is the first study to demonstrate that the incidence of non-allergic asthma is higher in women than in men throughout all the reproductive years. In the Tucson cohort, Dodge and Burrows reported that new diagnoses of asthma in subjects older than 40 years occurred almost entirely in women, and these subjects had no more allergic sensitisation than the remainder of the population.6 Following a group of children from age 10 to 20 years, Nicolai et al observed that most of the incident cases were female, and atopy at age 10 was not associated with subsequent asthma onset.18 More recently, Mandhane et al reported that in the Dunedin birth cohort, atopy was a risk factor for adolescent wheeze in boys but not in girls.19 However, none of these studies have assessed the magnitude and significance of the gender difference in the incidence of allergic and non-allergic asthma. To our knowledge, our study is also the first to report a lack of gender difference in the incidence rates of allergic asthma. The incidence of allergic asthma appears to decrease with age. This decrease has to be interpreted with caution because subjects from younger cohorts contributed to a greater extent to the incidence estimate at a younger age, and there might be a cohort effect.17 However, the magnitude of the gender difference in the incidence of allergic asthma is unlikely to be biased by a cohort effect because the same increase in atopic sensitisation with younger age is observed in men and women (online supplement, table E5).
Possible explanations for gender differences in asthma incidence
Although most prospective studies in adults show a higher incidence of asthma in women than in men, few studies have simultaneously tested the possible effects of other relevant factors.2–6 ,20 Gender differences in asthma diagnosis have been demonstrated in children, but there are few data in adults.7 ,8 We did not find any suggestion of a more frequent diagnosis in women. Gender differences in environmental exposure have been put forward.4 In our study, women were at increased risk of non-allergic asthma, suggesting that exposure to allergens is unlikely to account for the higher incidence of asthma in women. Higher exposure of women to other bronchial irritants at home21 or at work22 cannot be excluded. Another possibility might be a greater susceptibility of women at the same level of exposure,23 which might, in turn, be related to their lower airway calibre. However, the incidence of asthma remained significantly higher in women than in men after adjustment for smoking, occupational exposure and lung function. In addition, the higher risk of asthma in women is supported by their increased risk of BHR, which cannot be explained by gender differences in airway calibre.24 ,25 Other factors are likely to be involved in the gender difference in asthma risk. The fact that the gender differences in asthma prevalence were consistent during the two survey periods and across countries with different levels of exposure to environmental factors suggests an effect of genetic and biological factors rather than socio-cultural and environmental factors.
Obesity appears to be a potential major risk factor for asthma development in women.5 In some studies, but not all, obesity was found to be a risk factor for incident asthma in women but not in men.5 Furthermore, obesity has been found to be more strongly associated with non-allergic asthma than with allergic asthma.26 A detailed analysis of the ECRHS suggested a potential differential diagnosis linked to the presence of obesity in women.16 However, in the present analysis, the higher incidence of asthma in women could not be explained by differences in BMI or change in BMI. Although obesity, as such, seems unlikely to explain the higher risk of asthma in women, regulatory molecules secreted by the adipose tissues (such as leptin) might be involved in the gender differences in asthma.5
A role for sex hormones is frequently suggested, but no study has been able to relate the switch in asthma prevalence occurring around puberty to changes in hormonal levels. In particular, a recent cohort of adolescents does not show any relationship between the pubertal stages and the incidence of asthma.3 However, in a cohort of children with asthma, a marked decrease in bronchial responsiveness was observed after age 11 years in boys, but not in girls.27 A possible relaxing effect of testosterone on airway smooth muscle, and an anti-inflammatory and immune-modulatory activity of the major adrenal androgen dehydroepiandrosterone have been put forward.5 ,27–29 However further studies are needed to assess whether male sex hormones might have a protective effect in asthma. If the higher incidence of asthma in girls after adolescence is related to the rise in female sex hormones, one would expect a decrease in asthma incidence after the menopause. Such a decrease was reported in the Nurse's Health Study, but other studies found contrasting results.30 ,31 However, these studies have not considered allergic and non-allergic asthma separately, and most of the animal models that have been used to assess the effect of sex hormones in asthma were based on allergen-induced airway responsiveness. Interestingly, recent studies suggest a possible dual effect of female sex hormones.30 ,32 ,33 Data from a murine model suggested that oestrogen may have a pro-inflammatory effect in the process of antigen sensitisation per se, and an anti-inflammatory effect during the effector phase of the response to inhaled antigens.32 However, there are insufficient data to speculate on whether such an anti-inflammatory effect of oestrogen in women already sensitised to allergens might decrease their likelihood of developing symptoms.
Study strengths and limitations
One of the strengths of this study lies in the quality of the ECRHS data. Standardised data for lung function, BHR and specific IgE were available at baseline and follow-up, and for a relatively large population-based sample of subjects with different levels of exposure to environmental factors. As regards the study limitations, loss to follow-up is a problem in any longitudinal study. However, there was no suggestion of any gender differential selection bias among subjects. The definition of asthma was based on the subject's report of doctor-diagnosed asthma. This definition has been validated and found to be highly specific, but of rather low sensitivity.20 We cannot totally rule out a possible less frequent diagnosis of new-onset asthma in men than in women. Overlap of chronic obstructive pulmonary disease (COPD) and asthma is a concern in this type of analysis, particularly in non-atopic subjects. It has been suggested that COPD is more likely to be diagnosed as asthma in women than in men.34 However, only 12% of women with incident non-allergic asthma were heavy smokers, only 8% had a FEV1/forced vital capacity ratio lower than 0.70, 75% were younger than 50 years old, and a higher incidence of non-allergic asthma was found in women after excluding smokers at baseline (online supplement, table E4). Furthermore, our data suggest that asthma underdiagnosis is as frequent in women as in men. Because subjects were aged 20 years or more at inclusion, we cannot exclude the fact that a few subjects may have suffered from mild respiratory symptoms as early as childhood, and that these symptoms became severe enough in adulthood to be diagnosed as asthma. However, the results from a longitudinal birth cohort show that female sex is an independent predictor of adult-onset asthma after adjustment for wheeze in childhood.35 Furthermore, the higher incidence of asthma in women was still significant after excluding subjects with respiratory symptoms at baseline. As regards sensitisation, we cannot exclude that a few subjects with new-onset asthma classified as ‘non-atopic’ had ever been atopic and developed tolerance. Another possibility is that some subjects sensitised to other less common allergens may have been classified as ‘non-atopic’. However, similar findings were observed when baseline skin test sensitisation to any of nine common allergens was additionally used to classify incident cases as allergic and non-allergic asthma.
Implications and conclusion
Although women with severe non-allergic asthma may represent a substantial proportion of the adults with asthma in clinical practice, gender differences in the incidence of non-allergic asthma have been little investigated in the general population. In this large population-based cohort of adults, more than half the women with new-onset asthma and a third of the men with new-onset asthma were found to be non-atopic. This relatively high frequency emphasises the burden of non-allergic asthma in the adult population. However, our results also suggest that this form of asthma is still poorly recognised in men and women, and stress the need for more careful assessment of potential non-allergic asthma in clinical practice. Women were found to be at higher risk of developing non-allergic asthma throughout all the reproductive years, whereas no gender difference was observed for allergic asthma. Overall, our findings suggest that biological factors that significantly differ between men and women are likely to be involved in the development of non-allergic asthma. Further research in this direction is needed.
References
Supplementary materials
Supplementary Data
This web only file has been produced by the BMJ Publishing Group from an electronic file supplied by the author(s) and has not been edited for content.
Files in this Data Supplement:
- Download Supplementary Data (PDF) - Manuscript file of format pdf
Footnotes
Funding Several parties funded the study data collection. The complete list of funders is provided in the online supplement.
Competing interests None.
Patient consent The article does not contain personal medical information about identifiable subjects.
Ethics approval Local ethics committees and institutional review boards.
Provenance and peer review Not commissioned; externally peer reviewed.
Data sharing statement Researchers who wish to run analysis using the ECRHS data are invited to contact the coordinating centre in London. See the ECRHS website http://www.ecrhs.org.