Article Text

Abstract
Background Rates of mortality and readmission are high in patients hospitalised with acute exacerbations of chronic obstructive pulmonary disease (AECOPD). In this population, the prognostic value of the Medical Research Council Dyspnoea Scale (MRCD) is uncertain, and an extended MRCD (eMRCD) scale has been proposed to improve its utility. Coexistent pneumonia is common and, although the CURB-65 prediction tool is used, its discriminatory value has not been reported.
Methods Clinical and demographic data were collected on consecutive patients hospitalised with AECOPD. The relationship of stable-state dyspnoea severity to in-hospital mortality and 28-day readmission was assessed. The discriminatory value of CURB-65, MRCD and eMRCD, in the prediction of in-hospital mortality, was assessed and compared.
Results 920 patients were recruited. 10.4% died in-hospital and 19.1% of the 824 survivors were readmitted within 28 days of discharge. During their stable state prior to admission, 34.2% of patients were too breathless to leave the house. Mortality was significantly higher in pneumonic than in non-pneumonic exacerbations (20.1% vs 5.8%, p<0.001). eMRCD was a significantly better discriminator than either CURB-65 or the traditional MRCD scale for predicting in-hospital mortality, and was a stronger prognostic tool than CURB-65 in the subgroup of patients with pneumonic AECOPD.
Conclusions The severity of dyspnoea in the stable state predicts important clinical outcomes in patients hospitalised with AECOPD. The eMRCD scale identifies a subgroup of patients at a particularly high risk of in-hospital mortality and is a better predictor of mortality risk than CURB-65 in exacerbations complicated by pneumonia.
- Chronic obstructive pulmonary disease
- breathlessness
- pneumonia
- hospital admission
- mortality
- readmission
- COPD mechanisms
- COPD exacerbations
- long-term oxygen therapy (LTOT)
- lung physiology
- non-invasive ventilation
- respiratory muscles
- sleep apnoea
- systemic disease and lungs
- allergic alveolitis
- bronchiectasis
- COPD epidemiology
- cystic fibrosis
Statistics from Altmetric.com
- Chronic obstructive pulmonary disease
- breathlessness
- pneumonia
- hospital admission
- mortality
- readmission
- COPD mechanisms
- COPD exacerbations
- long-term oxygen therapy (LTOT)
- lung physiology
- non-invasive ventilation
- respiratory muscles
- sleep apnoea
- systemic disease and lungs
- allergic alveolitis
- bronchiectasis
- COPD epidemiology
- cystic fibrosis
Key messages
What is the key question?
What is the impact of stable-state dyspnoea and coexistent pneumonia on outcome in patients hospitalised with acute exacerbations of COPD?
What is the bottom line?
A novel extended version of the Medical Research Council Dyspnoea Scale (eMRCD) and the presence of pneumonia are both strongly associated with mortality and readmission; in patients with pneumonic exacerbations, eMRCD is a stronger predictor of mortality than CURB-65.
Why read on?
These findings should help clinicians identify patients at high risk of death who may benefit from either early escalation of care or early discussion of end-of-life care.
Background
Acute exacerbations of chronic obstructive pulmonary disease (AECOPD) requiring hospitalisation are responsible for a substantial proportion of the morbidity and mortality associated with the disease. The 2008 National UK COPD audit showed that 7.7% of patients hospitalised with exacerbations died during admission and about one-third of those discharged from hospital were readmitted within 90 days.1 As disease severity worsens, the frequency of hospital admission increases,2 and hospitalisation provides a potential window to identify and intervene in patients at risk of adverse outcome. The ability to accurately risk stratify patients presenting to hospital with exacerbations would help to prevent unnecessary admission in those deemed low risk and facilitate earlier intervention to reduce morbidity and mortality in those at high risk.
COPD exacerbations are commonly complicated by radiographic consolidation.3 There is debate over whether people with AECOPD and coexistent pneumonia should be included in the definition of AECOPD, with varying practice in the UK. However, pulmonary consolidation was not an exclusion in the major UK national audits of COPD exacerbations1 and non-invasive ventilation (NIV),4 in which patients with coexistent radiographic consolidation comprised 16% and 34.2% respectively. Furthermore, plain chest radiography is relatively insensitive for identifying pulmonary consolidation, with a number of patients with initially negative radiography found to have consolidation on subsequent more detailed imaging.5 6 In addition, Lieberman et al3 showed that, compared with patients with non-pneumonic exacerbations, those with coexistent radiographic consolidation were similar in terms of sociodemographic details and severity of the underlying COPD, although they had more abnormal markers of acute clinical and physiological derangement, suggesting that coexistent consolidation identifies patients with a more severe acute illness, but does not signify a different disease process. For these reasons we elected to include patients with coexistent consolidation in the present study.
In community-acquired pneumonia the CURB-65 prognostic tool7 is effective and widely used as a guide to clinical management, but its utility in patients with pneumonia-complicating AECOPD (pAECOPD) is less clear. CURB-65 is also sometimes used to guide clinical decisions in non-pneumonic AECOPD (npAECOPD) and a single prospective study supports this.8
In stable COPD, the severity of dyspnoea, measured by the Medical Research Council Dyspnoea Score (MRCD), is a stronger predictor of mortality than forced expiratory volume in 1 s (FEV1) alone.9 Its prognostic value in AECOPD requiring hospitalisation has, however, been infrequently studied, with single reports suggesting that higher MRCD scores are predictive of in-hospital10 and 3-year mortality.11 A small retrospective study from our department described a novel extended version of the MRCD scale (the extended MRC Dyspnoea Score, eMRCD), which had better discrimination than the traditional MRCD scale for the identification of patients at risk of frequent hospital admission,12 but this, and the relationship between eMRCD and in-hospital mortality, have not been further investigated.
We have undertaken a prospective observational study in a large population of patients with AECOPD, to compare the predictive ability of both the MRCD and eMRCD scores in relation to both in-hospital mortality and early rehospitalisation. We also assessed the impact of complicating pneumonia on outcome and the utility of CURB-65 in this population.
Methods
As part of a large prospective observational study, consecutive patients admitted with a primary diagnosis of AECOPD to one of two neighbouring acute general hospitals between December 2008 and June 2010 were recruited. Patients were identified primarily by screening the records of patients admitted with a clinical diagnosis of AECOPD on a daily basis. To ensure maximal data capture, hospital coding records were reviewed in order to identify patients who died or were rapidly discharged prior to identification by the research team, and data were gathered on all eligible patients not previously identified.
Inclusion criteria were admission with AECOPD; a clinical diagnosis of COPD supported by spirometric evidence of airflow obstruction (FEV1/forced vital capacity <0.70) during a period of clinical stability; age at least 35 years; smoking history of at least 10 cigarette pack years; and admission from the primary place of residence. Patients were not eligible for inclusion if they had previously been included in the study; they were being treated with domiciliary ventilation; they had life-threatening comorbidity that was expected to limit their life to less than 12 months; or if they had a primary admission diagnosis other than AECOPD.
Sociodemographic details, FEV1 and body mass index (BMI) on admission were recorded. Only FEV1 results obtained within 2 years of admission were used in data analysis. During their hospital stay, patients were asked to report their level of dyspnoea during their stable state in the preceding 3 months. The eMRCD12 categorises patients with traditional MRCD scores of 5 as either 5a or 5b depending on their ability to manage personal care (washing and dressing). This was documented routinely and recorded along with the traditional MRCD score (table 1). The presence of consolidation on the admission chest radiograph, as documented by the admitting medical team, and the CURB-65 score were recorded. The admission was labelled as pAECOPD or npAECOPD depending on whether consolidation was present or absent. Length of stay, need for ventilatory support (non-invasive or invasive ventilation), in-hospital and 30-day mortality, and readmission to hospital within 28 and 90 days of discharge were gathered by reviewing the hospital records. The local NHS Research Ethics Committee approved the project and advised that formal consent from individual patients was not required.
Statistical analysis
For variables with missing data, cases were excluded analysis by analysis. Descriptive statistics were used to characterise the patient sample, using proportions, means with standard deviations, or medians with inter-quartile ranges (IQRs) if appropriate. Bivariate comparisons were performed for pneumonic and non-pneumonic AECOPD using the χ2 test (gender and need for assisted ventilation), Student t test (age, FEV1 % predicted and BMI) and Mann–Whitney U test (MRCD and length of stay). Differences in outcome between eMRCD 5a and 5b, and between pAECOPD and npAECOPD, were assessed using the χ2 test. The discriminatory value of MRCD, eMRCD and CURB-65 in relation to in-hospital mortality was determined by computing the area under the ROC curve (AUROC) with 95% CIs. AUROC was compared between MRCD, eMRCD and CURB-65 using the method of DeLong et al14 and was computed using SigmaPlot version 11. All other statistical analyses were performed using SPSS V.15.0 for Windows and a two-sided p value <0.05 was taken as statistically significant.
Results
Data were obtained from 920 patients. Data capture was complete for all variables apart from FEV1 within 2 years of admission (14.3% missing) and BMI on admission (4.3% missing). The mean age of the patients was 73.1 years (SD 10.0) and 53.9% were women (table 2). Most patients had severe airflow obstruction (mean FEV1 % predicted 44.1, SD 18.0). Mean BMI was normal (24.6 kg/m2, SD 6.4) and approximately one-third of patients had radiographic evidence of pulmonary consolidation. Compared with patients with no consolidation, they were older, had slightly better preserved FEV1, and were more likely to have required assisted ventilation. Almost all (98.0%) patients receiving assisted ventilation were initially treated with NIV, with only four being immediately intubated and ventilated. Of patients in whom NIV failed, only four further patients progressed to invasive ventilation. Of the 51 patients with severe dyspnoea (eMRCD 5b) who met the criteria for assisted ventilation (pH <7.35 and arterial carbon dioxide pressure >6 kPa), 44 received it and seven were not ventilated, but instead received end-of-life care.
Population characteristics
Ninety-six patients (10.4%) died during admission (86 from respiratory disease and 10 from non-respiratory disease) and 115 (12.5%) died within 30 day of admission (table 3). Of the 824 surviving to discharge, 157 (19.1%) were readmitted to hospital within 28 days and 16 (1.9%) died within 28 days of discharge without being rehospitalised. Overall, 275 patients (33.4%) were readmitted to hospital within 90 days of discharge (table 4). Median length of stay was 6 days (IQR 3–11) and pAECOPD was associated with a longer hospital stay than npAECOPD (7 days vs 6 days; p<0.001). The in-hospital mortality rate for npAECOPD was 5.8% (36/621), whereas 20.1% (60/299) with pAECOPD died in-hospital (p<0.001). Twenty-eight-day readmission rates of those initially presenting with pneumonic and non-pneumonic AECOPD were similar (19.5% and 18.0% respectively; p=0.62).
Relation of dyspnoea grade and presence or absence of consolidation to mortality
Relation of dyspnoea grade and presence or absence of consolidation to readmission
The distribution of patients within each dyspnoea grade and the frequency of outcomes for the total population and the pAECOPD and npAECOPD subgroups are shown in tables 3 and 4. Pre-admission, during a period of clinical stability, 315 (34.2%) patients were too breathless to leave the house (MRCD 5). Of these, 173 (54.9%) were independent in washing and dressing (eMRCD 5a) and 142 (45.1%) were dependent in washing and dressing (eMRCD 5b).
Of the 96 patients who died in hospital, 30 were eMRCD 5a (17.3% mortality) and 47 eMRCD 5b (33.1% mortality) (p=0.0012). In the npAECOPD group, patients with eMRCD 5b had a significantly higher in-hospital mortality rate than those with eMRCD 5a (p=0.048); in the pAECOPD group, there was a similar but non-significant association (p=0.069) (table 3).
The 28-day readmission rate was significantly higher for those with eMRCD 5b than those with eMRCD 5a for the total population (p=0.044) and for the subgroup with npAECOPD (p=0.0005) (table 4). In pAECOPD, the rate was non-significantly lower with eMRCD 5b than eMRCD 5a (p=0.13); this is likely to be due to a survivor effect given the high in-hospital mortality in the former group. Of the 16 patients who died within 28 days of discharge without being readmitted to hospital, three were eMRCD 3–4, eight were eMRCD 5a and five were eMRCD 5b (eMRCD 5a vs eMRCD 5b: p=0.91).
Of the 299 patients with pAECOPD, median CURB-65 score was 2 (IQR 1–3) and 109 (36.5%) had CURB-65 scores of 3–5 and therefore a high risk of mortality (table 5). Mortality rates for each CURB-65 score were higher in pAECOPD than npAECOPD.
Distribution of patients, and rates of mortality, according to CURB-65 score
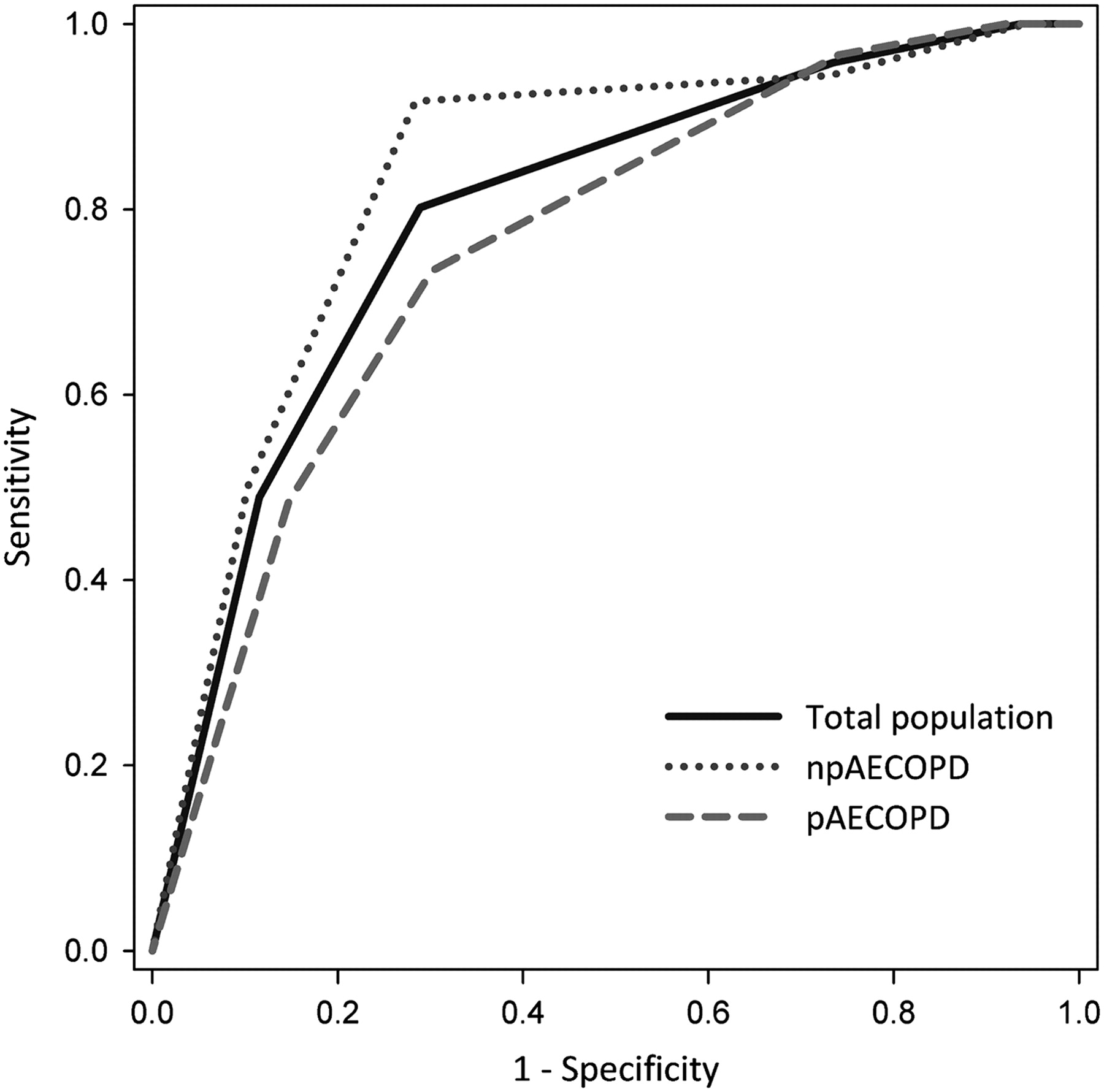
The discriminatory ability of MRCD, eMRCD and CURB-65 to predict in-hospital mortality was assessed and compared using areas under receiver operating characteristic curves (AUROC curves) (table 6). In the population as a whole, eMRCD had significantly better discrimination for in-hospital mortality than either MRCD (p=0.0012) or CURB-65 (p=0.019), and in the npAECOPD group there was a non-significant trend to better discrimination for eMRCD compared with both CURB-65 (p=0.053) and MRCD (p=0.057). In pAECOPD, eMRCD performed significantly better than CURB-65 for both in-hospital (AUROC=0.759 vs 0.661, p=0.017) and 30-day (AUROC=0.753 vs 0.640, p=0.040) mortality. The discriminative strength of eMRCD for in-hospital mortality is shown in figure 1.
Area under receiver operating curve for prediction of in-hospital mortality
{kind=link}
The discrimination of eMRCD for in-hospital mortality for the total population, non-pneumonic and pneumonic exacerbations of COPD.
Discussion
Of our population of patients admitted with AECOPD, more than one-third were housebound (MRCD 5) in the stable state. We found that the severity of dyspnoea in the stable state was strongly associated with both in-hospital mortality and early readmission. We have also shown that extending the traditional MRCD scale to take account of a person's ability to manage personal care (eMRCD) improves the prognostic strength of the instrument for both in-hospital mortality and early rehospitalisation following discharge, and identifies a subgroup of patients at particularly high risk of in-hospital mortality (33.1% with eMRCD 5b). In addition, our results highlight the adverse prognostic effect of radiographic pulmonary consolidation complicating AECOPD (in-hospital mortality of 20.1% in the pAECOPD group compared with 5.8% in the npAECOPD group).
Our study has notable strengths. Great effort was made to ensure inclusion of, and complete data capture in, all patients hospitalised with AECOPD during the period of the study, including those in whom the diagnosis of COPD had not previously been made and patients with a very short length of stay who otherwise might not have been brought to our attention. Our study also has the major strength of a large population of patients with AECOPD admitted consecutively to one of two large general hospitals. Our entry criteria were developed to make the study as inclusive as possible, and to reflect the general population of patients hospitalised with AECOPD in the UK. We are also aware of certain limitations to the study. In 15% of patients no spirometric measurements were available within 2 years of admission; spirometric support for the diagnosis of COPD was, however, obtained for all these patients. Although clinical information was obtained by a number of nursing and medical staff, standard protocols for gathering and recording the data were in place for patients admitted with AECOPD. Finally, the presence or absence of radiographic consolidation was recorded by the admitting medical team and radiographs were not specifically reviewed for the purpose of the study.
In comparison to the 2008 UK National COPD Audit,1 the overall in-hospital mortality in our study is somewhat higher; this is attributable mainly to the higher prevalence of coexistent consolidation in our cohort (32.5% compared with 16% in the National COPD Audit) and the associated worse prognosis. Different centres vary as to whether they include cases with pneumonia; to allow valid comparison of relative mortality, we suggest future audits stratify outcome according to the presence of coexistent consolidation. The readmission rate at 90 days (33.4%) is almost identical to that reported in the National COPD Audit.1
The severity of stable-state dyspnoea in patients hospitalised with AECOPD has rarely been reported previously. Similarly to our finding, the 2008 UK National COPD Audit1 suggested that approximately 30% of admitted patients were too breathless to leave the house (MRCD 5), but the conclusion was limited by missing data in more than half of the patients audited. Other studies11 15 16 have recorded dyspnoea severity only in patients surviving to discharge, which underestimates its importance because of its strong association with mortality. Higher MRCD scores have previously been shown to be associated with greater in-hospital mortality in patients attending the emergency department with AECOPD,10 an association we have confirmed for all patients hospitalised with AECOPD. A recent study17 showed an association between the traditional MRCD score and hospital readmission in patients enrolled in an early supported discharge scheme, but to our knowledge a similar association between MRCD and hospital readmission in all patients hospitalised with AECOPD has not been reported.
Greater functional dependence has been shown independently to predict hospital readmission,15 18 and performance status, which includes an assessment of a patient's ability to self care, has been shown to be predictive of 3-month mortality following admission.19 Also, in patients surviving to discharge, a high level of functional dependence is associated with long-term mortality.16 20 21 Most of the deaths (80%) in our study occurred in patients with severe stable-state dyspnoea (MRCD 5). We have shown that combining a measure of functional dependence with the assessment of dyspnoea severity (eMRCD) improves the predictive ability of the traditional MRCD scale, with a significantly higher risk of mortality in patients housebound and dependent in washing and dressing (eMRCD 5b) than in those housebound but independent in washing and/or dressing (eMRCD 5a).
Clinical decisions were in the hands of the admitting medical teams and uninfluenced by our study; however, we recognise that severe disability is likely to have been an important consideration in determining the management of individual patients. However, our finding does not appear to be explained by early introduction of palliative care, or limiting the level of care, in this population because even among patients with the most severe limitation (eMRCD 5b), most of those potentially eligible for assisted ventilation received it, and there was no difference in this regard between eMRCD 5a and eMRCD 5b.
Using the extended scale, each increase in dyspnoea severity was accompanied by a significantly higher mortality, and the prediction of in-hospital mortality was significantly better using eMRCD than MRCD (AUROC=0.794 vs 0.769; p=0.0012) (table 6). For the total population and for the npAECOPD group, eMRCD also improved identification of patients at risk of hospital readmission (table 4).
Our study shows that co-existent consolidation is common in patients with AECOPD and is associated with a high mortality rate. In community-acquired pneumonia, 30-day mortality rates according to CURB-65 have been previously reported to be: CURB-65 0–1=1.5%; CURB-65 2=9.2%; and CURB-65 3–5=22.4%.7 Our study shows that the combination of AECOPD and pneumonia is associated with higher mortality rates than pneumonia alone: pAECOPD and CURB-65 0–1=11.1% in-hospital mortality; pAECOPD and CURB-65 2=16%; and pAECOPD and CURB-65 3–5=31.2%. Therefore, although the CURB-65 risk stratification tool is frequently used to guide management in pAECOPD, our data show that it underestimates the risk of mortality in this population. The results of AUROC analysis (table 6) confirm that in pAECOPD, the performance of CURB-65 was only moderate (AUROC=0.661), and eMRCD (AUROC=0.759) was a significantly better discriminator for both in-hospital (p=0.017) and 30-day mortality (p=0.040). Our results concur with a recent study8 that showed CURB-65 to have good discrimination for in-hospital mortality in npAECOPD (AUROC=0.733), but in our study, the eMRCD outperformed CURB-65 for all patients and we suggest that it is the better predictive tool.
Previous studies to identify prognostic indices in AECOPD requiring hospitalisation have been performed infrequently and (with the exception of patients requiring intensive care) robust clinical tools to aid management of such patients have not been developed.22 The present study shows that the assessment of dyspnoea severity in patients hospitalised with AECOPD is simple to perform, is a strong predictor of outcome and may therefore provide valuable information which could influence management. For example, of the total population, no patients hospitalised with eMRCD grade 1 or 2 died either in hospital or at home shortly after discharge, and in the npAECOPD group with eMRCD 1–4, in-hospital mortality was very low and therefore many of these patients might have been safely managed in the community. Alternatively, one-third of all patients with eMRCD 5b, and almost a half of patients with coexistent pneumonia and eMRCD 5b, did not survive to discharge and such patients might benefit from either early escalation of care or, in some cases, early discussion of end-of-life care.
We conclude that severe dyspnoea is common in patients hospitalised with AECOPD and the severity of dyspnoea is a strong predictor of mortality and early rehospitalisation. A novel extension of the traditional scale, the eMRCD, improves its predictive ability for both mortality and readmission. Pneumonic exacerbations of COPD are an important and common clinical problem with overall worse outcome than primary community acquired pneumonia. The CURB-65 prediction tool for pneumonia performs less well in patients with pAECOPD. Further research is needed to develop practical prognostic tools in AECOPD in order to aid clinical management.
References
Footnotes
Correction notice This article has been corrected since it was published Online First. Tables 3 and 4 contained numbers which were not aligned in the columns correctly.
Competing interests None.
Ethics approval This study was conducted with the approval of NHS County Durham and Tees Valley 1 Research Ethics Committee.
Provenance and peer review Not commissioned; externally peer reviewed.