Article Text

Abstract
Rationale The SenseWear armband (SAB) is designed to measure energy expenditure (EE). In people with chronic obstructive pulmonary disease (COPD), EE estimated using the SAB (EESAB) is a popular outcome measure. However, a detailed analysis of the measurement properties of the SAB in COPD is lacking.
Objective To examine the sensitivity of EESAB, agreement between EESAB and EE measured via indirect calorimetry (EEIC), and its repeatability in COPD.
Methods 26 people with COPD (forced expiratory volume in 1 s (FEV1)=49±18% predicted; 15 males) spent 6 min in five standardised tasks that comprised supine, sitting, standing and two walking speeds. A subgroup (n=12) walked using a rollator. Throughout each task, measurements of EESAB and EEIC were collected. The protocol was repeated on a second day.
Results EESAB increased between standing and slow walking (2.4, metabolic equivalents (METs) 95% CI 2.2 to 2.7) as well as slow and fast walking (0.5 METs, 95% CI 0.3 to 0.7). Considering all tasks together, the difference between EESAB and EEIC was −0.2 METs (p=0.21) with a limit of agreement of 1.3 METs. The difference between days in EESAB was 0.0 METs with a coefficient of repeatability of 0.4 METs. Rollator use increased the variability in EESAB, compromising its repeatability and agreement with EEIC.
Conclusions EESAB was sensitive to small but important changes. There was fair agreement between EESAB and EEIC, and measurements of EESAB were repeatable. These observations suggest that the SAB is useful for the evaluation of EE in patients with COPD who walk without a rollator.
- COPD
- equipment evaluations
Statistics from Altmetric.com
Introduction
Physical activity confers important health benefits.1 2 The increased energy demands from physical activity require greater substrate delivery, utilisation and product removal from skeletal muscles. Adaptation to such chronic demands conditions the cardiovascular system and may reduce all-cause mortality.3 4 Physical activity is increasingly being used as an outcome measure of treatments for people with chronic obstructive pulmonary disease (COPD).5 6
Estimating energy expenditure (EE) during daily life is commonly achieved by measuring bodily movement.7 Inaccuracies associated with self-reports8 have resulted in triaxial accelerometers, which detect movement of the body or limbs and yield accurate measurements of physical activity, emerging as a popular choice.7 8 However, accelerometers cannot detect changes in EE associated with differences in load or efficiency such as from alterations in terrain or gradient, which change energy demands without impacting substantially on body movement. Measurements of EE will be optimised by an approach that does not rely solely on detecting body movement.
Bodymedia (Pittsburgh, Pennsylvania, USA) has developed a lightweight, small metabolic monitor called the SenseWear armband (SAB) which estimates EE (EESAB) using accelerometer and non-invasive physiological measures.9 Relative to healthy individuals, reduced movement efficiency10 11 and anxiety12 seen in people with COPD may increase oxygen consumption during activity. These differences limit the capacity to generalise measurement properties of the SAB in a healthy population to this patient group. Two studies in COPD have examined the agreement between EESAB and that derived via indirect calorimetry (EEIC) using a portable gas analysis unit.9 13 Both recruited small samples of subjects with COPD (n≤10) and did not report prospective power calculations, or precision of their estimates, thereby limiting confidence in their results.9 13 An assessment was lacking of the sensitivity of the SAB to detect the difference in EE associated with changing from standing to walking at slow speeds.14 Repeatability of measurements over 2 days was not examined. These properties are essential to the planning and interpretation of studies that use the SAB to evaluate EE in people with COPD.
The aim of this study was to examine the sensitivity of EESAB, defined as its capacity to detect small increases in EE in people with COPD, during tasks that mimicked daily living. Our protocol also allowed examination of: (1) the agreement between EESAB and EEIC to determine the capacity of the SAB to serve as an indirect calorimeter; (2) the repeatability of EESAB over two identical test sessions; and (3) the accuracy of the SAB to measure step rate. A secondary aim was to examine the measurement properties of the SAB during rollator-assisted walking as the benefits15 and satisfaction16 with rollators have made them popular among people with COPD. Methods and results pertaining to the secondary aim can be found in the online supplement.
Methods
Design and study subjects
A cross-sectional observational study was undertaken. Individuals with symptomatic, clinically stable COPD (ratio of postbronchodilator forced expiratory volume in 1 s (FEV1) to forced vital capacity <0.7)17 and a smoking history >10 pack-years were recruited from pulmonary rehabilitation programmes and Respirology clinics. Individuals were excluded if they: (1) had a co-morbid condition thought to compromise mobility such as musculoskeletal problems; (2) had a history of mastectomy for right-sided breast cancer; or (3) were using long-term continuous oxygen therapy. The study was approved by the Research Ethics Board at West Park Healthcare Centre. Subjects provided written informed consent before participation.
Protocol
Subjects attended two sessions, each ∼3 h, separated by ≥24 h. Height and weight were measured. Gender and hand dominance were recorded. The most recent measurements of resting lung function and 6 min walk distance (6MWD) were retrieved from the medical records. During both sessions, subjects undertook identical tasks in the same sequence while wearing the SAB and a portable gas analysis system (Cosmed K4b2; COSMED, Rome, Italy).
Stationary tasks
Subjects spent 6 min in: (1) supine; (2) unsupported sitting; and (3) upright standing. In supine, a maximum of two pillows were permitted for comfort.
Active tasks
At the beginning of the first session, before data collection, subjects were asked to walk 60 m at a speed that they considered to be ‘slow’ and thereafter at a speed they considered to be ‘faster’, but one that they could maintain for 6 min. In contrast to selecting two arbitrary speeds for all subjects, these self-selected speeds made them relevant to daily life. The time taken to complete these tasks was recorded and average walking speeds were calculated. Pilot data indicated that occasionally subjects were unable to maintain ‘fast’ walking for 6 min. Therefore, to optimise the likelihood of all subjects completing the ‘fast’ task, where necessary, the ‘fast’ speed was reduced to 90% of the average speed achieved during the most recent 6 min walk test. For each subject, the speeds determined at the first session were used for both test sessions.
During each session, subjects completed two separate 6 min walking tasks, separated by 15 min, on a 30 m level, enclosed, temperature-controlled corridor. Speed during the tasks was kept constant using a methodology adapted from the endurance shuttle walk test.18 First, the corridor was marked at 5 m intervals using orange cones. Then an audio signal of constant periodic beeps was selected. Each beep corresponded to when the first investigator needed to pass a cone in order to maintain the predetermined speed. For example, the audio signal corresponding to a speed of 50 m/min emitted a beep every 6 s. The subject followed 2.5 m behind the first investigator and a second investigator supervised each task to ensure this distance remained constant. If a subject was unable to maintain the required speed, the task was terminated. On completion of both walks, dyspnoea was measured using the Borg category ratio scale (0–10).
Equipment and measurements
SenseWear armband (SAB)
The SAB was worn on the triceps brachii bulk of the right arm. It estimates EESAB using measurements from a biaxial accelerometer and sensors that quantify galvanic skin response, heat flux and skin temperature in a proprietary algorithm (version 6.1). A total of seven SAB devices were used during this study.
Cosmed K4b2
The Cosmed K4b2 is a portable telemetric gas analysis unit in which the face mask, tubing, battery pack and transmitting unit are lightweight (0.8 kg) and attach via a chest harness. The gas analysers and turbine were calibrated before every use. Measurements of EEIC were estimated from measurements of oxygen uptake where 1 metabolic equivalent (MET) was equal to 3.5 ml/kg/min.
Step rate
During the walking tasks, the second investigator counted the number of steps taken by each subject over three separate 10 m segments of the corridor. A step was defined as any heel strike between the cones delineating a 10 m segment. The average number of steps was used to derive the step rate.
Data management and statistical analyses
Analyses were performed using SAS (version 8; SAS, Cary, North Carolina, USA). p Values <0.05 were considered significant. Data are expressed as mean±SD and 95% CIs unless otherwise stated.
Analyses
Additional details are provided in the online supplement. The average EEIC expressed in METs measured during each minute of each task was calculated and plotted to examine the profile. Only data averaged over the last 3 min of each task (ie, during steady state) were included in the analyses as oxygen uptake best estimates total EE during steady state.19
To determine if the SAB could detect a significant difference among tasks, we used a repeated measures analysis of covariance (ANCOVA) to examine the effect of day, task and the interaction between the two on the dependent variable, EESAB, corrected for FEV1 (% predicted).
Before calculating agreement, we used ANCOVA to examine the effect of day, task and the interaction between the two on the dependent variable, difference in EE between devices (EESAB–EEIC) corrected for FEV1 (% predicted). In the absence of significant F ratios, we proceeded with analysis for agreement using methods described by Bland and Altman.20 A similar procedure was used to examine repeatability.
Prospective sample size calculations
We were interested in determining the sensitivity of the SAB to accurately detect a difference in EE between standing and slow walking; estimated to be 1 MET.21 To do this, we required adequate precision around our estimates of agreement and repeatability; defined by the width of the 95% CI for the limits of agreement and coefficient of repeatability. We stated, a priori, that these 95% CI needed to span ≤1 MET so that the signal (difference between standing and slow walking) was not less than the precision afforded by our sample size. Using the formula provided by Bland and Altman20 we calculated that a sample size of 25 would allow a precision of 1 MET (SD of 0.7 METs).19
Results
The characteristics of the 26 subjects who consented to participate are summarised in table 1. One subject (4%) did not return on the second day of testing due to an acute exacerbation and one (4%) was unable to tolerate the face mask required for EEIC. On the first day of testing, all subjects completed the stationary tasks, with 21 (81%) and 17 (65%) completing the slow and fast walking tasks, respectively. On the second day of testing, 25 (96%) subjects completed the stationary tasks, with 21 (81%) and 16 (61%) completing the slow and fast walking tasks, respectively. The average speeds selected for the slow and fast walking tasks were 51.4±11.1 and 65.4±12.4 m/min, respectively. The slow and fast walking tasks elicited dyspnoea scores equal to 1.4±1.0 and 2.2±1.2, respectively. The average EE for each minute of each task measured using both devices on the first test day are plotted in figure 1A–F. The SAB was well tolerated by all subjects. There was no significant effect of FEV1 on sensitivity, agreement and repeatability analyses.
Subject characteristics (n=26; 15 males; 2 left-hand dominant)

Profile of energy expenditure (EE) in metabolic equivalents (METs) measured each minute during all tasks on day 1. Data are the mean and SD. Filled circles, SenseWear armband (SAB) data; open circles, indirect calorimetry data.
Sensitivity
There was no interaction (day×task; F4,75=0.83; p=0.51) or effect of day (F1,22=0.03; p=0.85) on the difference in EESAB among tasks. Using data collected over both days, there was a significant effect of task on EESAB (F4,82=270; p<0.01). The differences between tasks, averaged across both days, are summarised in table 2.
Mean energy expenditure (in metabolic equivalents) measured using the SenseWear armband (SAB) during each task and the difference between tasks
Agreement
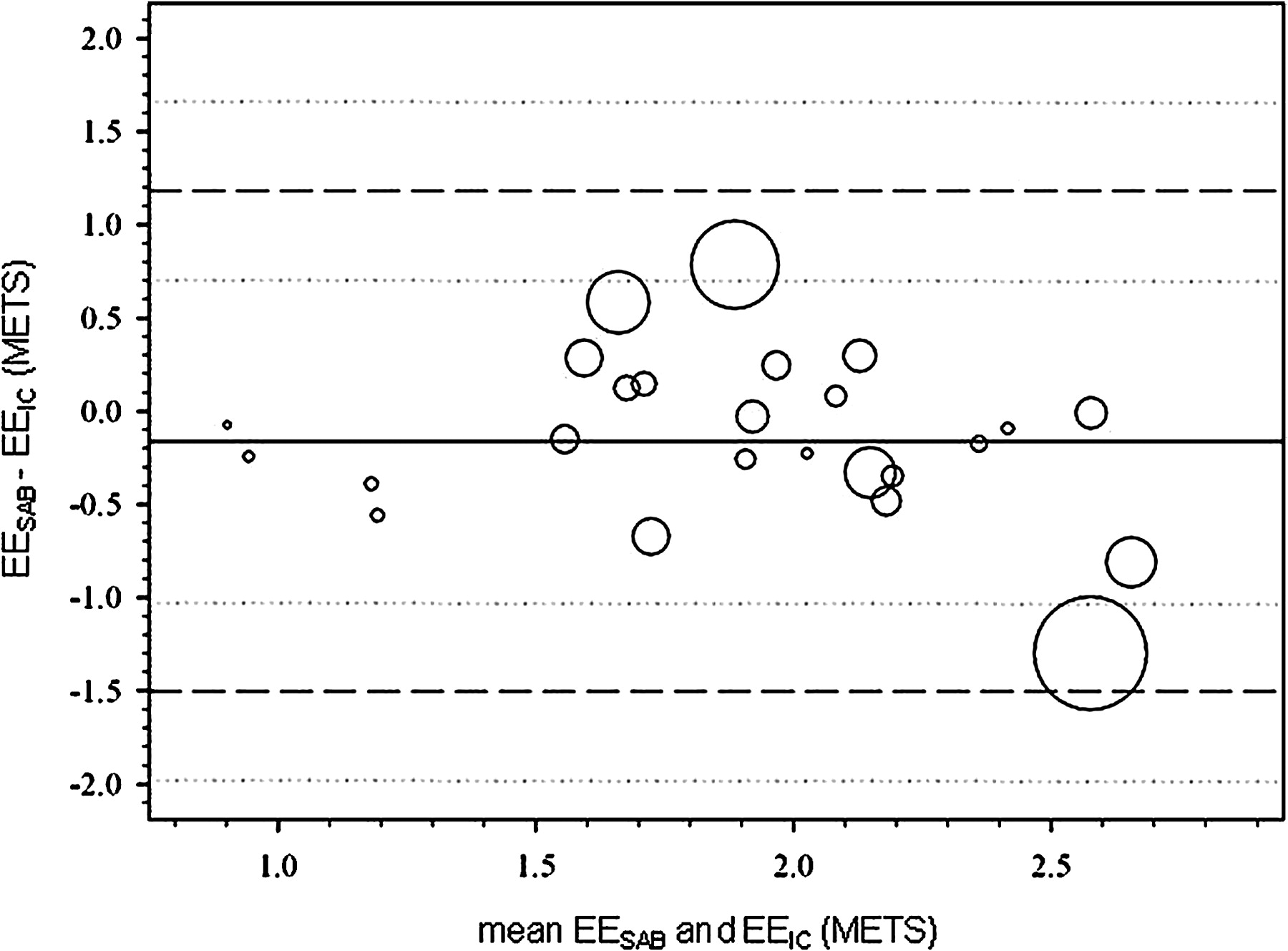
There was no interaction (day×task; F4,68=0.26; p=0.91), effect of day (F1,21=0.03; p=0.87) or task (F4,78=1.82; p=0.13) for the difference between EESAB and EEIC, indicating that the magnitude of difference between EESAB and EEIC did not differ among days or tasks. The Bland–Altman plot for agreement in EESAB and EEIC is displayed in figure 2. The overall difference between the devices was −0.2 METs (p=0.21) and the limit of agreement was 1.3 METs. Upper and lower limits of agreement occurred at 1.2 (95% CI 0.7 to 1.7) and −1.5 (−2.0 to −1.0), respectively.

Bland–Altman plots for agreement between energy expenditure (EE; metabolic equivalents (METs)) measured via a SenseWear armband (EESAB) and indirect calorimetry (EEIC). The size of the circle indicates the variability within each subject. The solid line represents mean difference (bias). The dashed line represents the limits of agreement and their CIs (dotted lines).
Repeatability
There was no significant effect of task on the difference in EESAB measured over the 2 days (F4,22=0.97; p=0.45). The Bland–Altman plot for repeatability of EESAB over the 2 days is displayed in figure 3A. The difference in EESAB between days was 0.0 METs and the coefficient of repeatability was 0.4 METs. Upper and lower limits occurred at 0.4 (0.3 to 0.6) and −0.5 (−0.6 to −0.3), respectively.

Bland–Altman plots for repeatability of energy expenditure (EE; metabolic equivalents (METs)) measured over two test days using (A) a SenseWear armband (EESAB) and, (B) indirect calorimetry (EEIC). The size of the circle indicates the variability within each subject. The solid line represents mean difference (bias). The dashed line represents the coefficient of repeatability and their CIs (dotted lines).
There was no significant effect of task on the difference in EEIC measured over the 2 days (F4,21=0.99; p=0.43). The Bland–Altman plot for repeatability in EEIC over the 2 days is displayed in figure 3B. The difference in EEIC between days was 0.0 METs and the coefficient of repeatability was 0.6 METs. Upper and lower limits occurred at 0.6 (0.4 to 0.8) and −0.6 (−0.9 to −0.4), respectively.
Step rate
The average step rate recorded by the SAB was referenced against those calculated via direct observation (figures 4A,B). Using data averaged over the 2 days, step rate measured via SAB was less than that by direct observation at the slow walking speed (77±26 vs 87±9 steps/min; p=0.04), but not the faster walking speed (93±22 vs 99±10 steps/min; p=0.22).

{kind=link}
{kind=link}
{kind=link}
{kind=link}
Step rate during (A) slow walk and, (B) fast walk averaged over the two test days. Data are mean and SD. Filled circles, SenseWear armband (SAB) data; open circles, data calculated via direct observation. *p<0.05 vs SAB.
Discussion
This is the first study to recruit a sample size of sufficient magnitude to examine whether the SAB is able to detect a small increase the EE during common activities of daily living in people with COPD. We have also reported the precision of our estimates. We note that: (1) the EESAB was sensitive to small but important changes; (2) the limit of agreement in EESAB and EEIC was 1.3 METs and the difference was not systematic; (3) the coefficient of repeatability for EESAB was 0.4 METs and the difference was not systematic; and (4) the SAB underestimated step rate at slow walking speeds. In a subgroup, we observed that walking with a rollator increased the variability of EESAB and compromised its agreement with EEIC and the capacity of the SAB accelerometer to detect steps (see online supplement).
Significant differences were demonstrated in EESAB between standing, slow and fast walking. Although earlier work reported that EESAB increased in response to large increases in walking speed,19 22 our finding is relevant to populations who walk very slowly. The SAB had adequate sensitivity to detect the small increase in average EE (0.5 METs) resulting from a modest increase in average walking speed (14 m/min). The average increase in distance walked as a consequence of the increased speed (ie, 84 m) is likely to be considered important by individuals with COPD.23 Given the excellent repeatability of the measurements of EESAB, a clinician could confidently detect differences resulting from small changes in walking speed of a patient.
The average difference between EESAB and EEIC was small (0.2 METs). Figure 1 reveals that EEIC and EESAB were similar for all tasks. Previous studies in other populations report that, during flat treadmill walking, EESAB was greater than EEIC.19 24 25 The disparity between these results and our data may reflect the faster walking speeds selected during the earlier studies19 25 or differences in efficiency between treadmill and corridor walking. Alternatively, it might reflect differences in the management of the data as we compared EESAB with EEIC only during the steady state. Studies that included data during non-steady state exercise may have underestimated EE.24 25
Our finding of a limit of agreement of 1.3 METs compares favourably with earlier work in healthy individuals and those with cystic fibrosis, reporting limits at 1.5 METs19 and 3.4 METs (assuming mean weight=70 kg),25 respectively. Our finding of similar measures of EESAB compared with EEIC agrees with one9 but not both previous studies in COPD.13 One study13 reported that EESAB was lower than EEIC and the magnitude of this difference increased with greater metabolic demands. The disparity between their data and ours may be the result of the older version of software used in the previous study13 or a difference in activities. Our protocol and that used by Langer et al9 were characterised by activities of daily living, while Patel et al13 examined agreement during field-based walking tests and suggested agreement was worse at more intense walking speeds, >82 m/min. As only 2 (8%) subjects in our study selected walking speeds >82 m/min, we do not comment on the agreement between EESAB and EEIC for individuals at these speeds.
Measurements of EESAB were repeatable. One previous study in an obese population reported a strong correlation between EESAB measured at rest over 2 days (r=0.88; p <0.001).24 Our data extend this finding by reporting a mean difference in EESAB measured during conditions of daily living over 2 days of 0.0 METs and a coefficient of repeatability of 0.4 METs. Therefore, a difference in average daily EESAB during conditions of daily living of >0.4 METs is needed to be 95% confident that any difference in EESAB is not simply the result of measuring it on a different day. Of interest, EESAB demonstrated less day-to-day variability than EEIC.
The SAB significantly underestimated step rate at slow speeds. Although previously reported,9 our data extend this finding by demonstrating the threshold below which the SAB is unlikely to yield accurate results (ie, speeds <50 m/min).
We present preliminary data to suggest shortcomings of using the SAB in a population who use a rollator to ambulate. Fixation of the upper limb on a rollator is likely to dampen the input from the accelerometer, a contention supported by the large underestimation of step rate during this task. The average EESAB was similar to EEIC, supporting the contention that the SAB algorithm relies more on the physiological sensor data than the accelerometer data in its estimation of EE.13 Nevertheless, the use of a rollator substantially increased the variability in the measurement of EESAB, thereby compromising agreement with EEIC and its repeatability, suggesting that clinically the SAB is unlikely to yield useful measures of EE in rollator users. Given the reduced number of subjects available for these secondary analyses, we emphasise that these data must be interpreted with caution.
Limitations
Although our design enabled us to undertake a detailed examination of the measurement properties of the SAB during walking, the main activity undertaken by people with COPD during daily life,14 we did not evaluate activities such as stair climbing, cycling or upper limb activity, which may contribute to the EE in COPD. Cost and access prevented our undertaking measurements of EE via direct calorimetry or doubly labelled water.7 Although some variability contributing to the limit of agreement may have resulted from measurement error associated with EEIC, portable gas analysis units are widely used to collect the reference measure for determining agreement with EESAB.9 13 19 24 25
Conclusion
The SAB is a useful and well-tolerated device in people with COPD. It was sensitive to small increases in EE resulting from increased walking speed. During supine, sitting, standing and walking there was fair agreement between EESAB and EEIC as the limit of agreement was equal to 1.3 METs. Repeatability of EESAB was excellent (coefficient of repeatability=0.0 METs) but it underestimated step rate at average walking speeds <50 m/min. Measures of EESAB collected while walking with a rollator were highly variable and are therefore less likely to be useful.
Acknowledgments
We greatly acknowledge the assistance of Clarissa Muere, Dr Vishal Bansal and Sachi O'Hoski with data collection for this study.
references
Supplementary materials
Web Only Data thx.2009.128702
Files in this Data Supplement:
{kind=link}
Footnotes
Funding Great West Life. DB is supported by a Canada Research Chair and RG by the NSA Chair in Respiratory Rehabilitation Research.
Competing interests None.
Ethics approval This study was conducted with the approval of the West Park Healthcare Centre.
Provenance and peer review Not commissioned; externally peer reviewed.