Article Text

Abstract
Background: Endobronchial ultrasound (EBUS) with transbronchial needle aspiration (TBNA) is becoming widely used for mediastinal lymph node staging in patients with known or suspected lung cancer. While a substantial number of case series have evaluated test performance of this investigation, the small sample sizes limited the ability to accurately evaluate the precision of EBUS-TBNA as a staging modality. A systematic review was performed of published studies evaluating EBUS-TBNA for mediastinal lymph node staging to ascertain the pooled sensitivity and specificity of this investigation.
Methods: A literature search was constructed and performed by a professional medical librarian to identify the literature from 1960 to February 2008. Pooled specificity and sensitivity was estimated from the extracted data with an exact binomial rendition of the bivariate mixed-effects regression model.
Results: Of 365 publications, 25 were identified in which EBUS-TBNA was specifically focused on mediastinal node staging. Of these, only 10 had data suitable for extraction and analysis. The overall test performance was excellent with an area under the summary receiver operating characteristics curve of 0.99 (95% CI 0.96 to 1.00); similarly, EBUS-TBNA had excellent pooled specificity of 1.00 (95% CI 0.92 to 1.00) and good pooled sensitivity of 0.88 (95% CI 0.79 to 0.94).
Conclusions: EBUS-TBNA has excellent overall test performance and specificity for mediastinal lymph node staging in patients with lung cancer. The results compare favourably with published results for computed tomography and positron emission tomography.
Statistics from Altmetric.com
Diagnostic fine needle aspiration of paratracheal masses began as early as 1978, using an oesophageal biopsy needle directed via a rigid bronchoscope.1 2 As technology improved, smaller and more flexible aspiration needles were manufactured for use within a flexible bronchoscope.1 The development of endobronchial ultrasound (EBUS) became a significant complementary advancement. Olympus developed one of the first purpose-specific models3 with a convex probe facilitating real-time EBUS-guided transbronchial needle aspiration (TBNA) of mediastinal and hilar lymph nodes.
As technology advances, EBUS-TBNA has become increasingly available and more widely used for mediastinal lymph node staging in patients with known or suspected lung cancer. While there are a number of published case series evaluating the sensitivity and specificity of this investigation, the numbers recruited within each study are small and therefore the precision on the derived estimates in each is wide.
The aims of our study were to perform a systematic review of EBUS-TBNA and to ascertain the pooled sensitivity and specificity of this investigation compared with published results of computed tomography and positron emission tomography scans (CT and PET) for mediastinal lymph node staging in patients with lung cancer.
Methods
Study identification and eligibility
We sought to identify all studies that used EBUS for mediastinal lymph node staging for lung cancer. The search was constructed and performed by a professional medical librarian.
A systematic literature search was performed of Medline (1950– February 2008), Embase (1974– February 2008) and Cochrane Library 2008, Issue 1. To achieve the maximum sensitivity of the search strategy and identify all relevant studies, appropriate free text and thesaurus terms were used including, among others, “non-small cell lung carcinoma”, “neoplasm staging” and “endobronchial” (the full search strategy is listed in online Appendix A). We searched trial registers on the Internet. In order to locate unpublished work, abstracts from major scientific meetings 2005–2007 were searched. Reference lists of all relevant studies were reviewed. No restrictions were placed on language.
Three investigators (KA, PS, EL) independently evaluated references for inclusion. Discordances were resolved by consensus. We included all studies that examined EBUS for mediastinal staging in patients with suspected or confirmed lung cancer (both small and non-small cell subtypes).
When multiple papers were published from a single institution we included all papers where there were no overlapping study periods. In the event of multiple publications with overlapping study periods, we included only one publication to prevent double counting of the patient cohorts. The selection was based on a hierarchy consisting first of patient population characteristic (ie, all patients with suspected lung cancer) followed by the publication with the largest patient series.
We excluded papers that were not about EBUS, review articles, studies that included patients with the primary underlying disease other than lung cancer, studies that were solely focused on mediastinal node staging and studies of restaging after induction therapy.
Quality assessment, data abstraction and synthesis (QADAS)
The QUADAS scoring system was used to appraise the quality of all included studies.4 It is a specific tool that assesses 14 domains of design and the presentation of studies of diagnostic accuracy. Data were abstracted with the patient as the unit of analysis to prevent cluster sampling error and to focus on the ability of EBUS to accurately stage the mediastinum rather than any particular lymph node or station.
Two-by-two contingency tables were created for each study, with patients categorised into one of four options: true positive, false positive, false negative and true negative. The extracted data were pooled with an exact binomial rendition5 of the bivariate mixed-effects regression model developed by van Houwelingen6 7 for treatment trial meta-analysis and modified for synthesis of diagnostic test data8 9 using the Midas9 module in Stata 9.2 (StataCorp, College Station, Texas, USA).
Results
Study selection
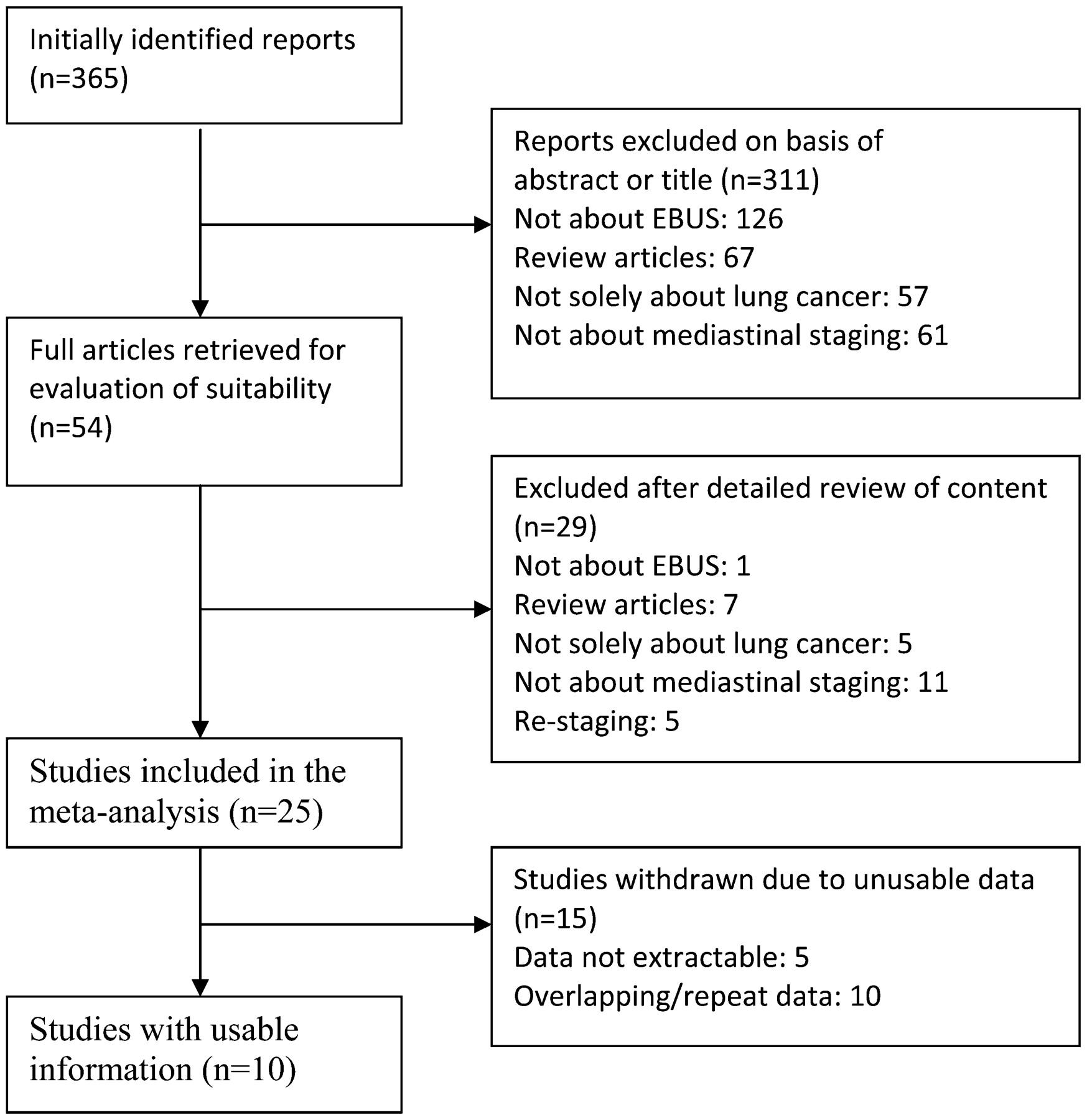
Our search strategy identified 365 papers for consideration. Of these, 311 were excluded based on review of the abstracts (126 not specifically pertaining to EBUS, 67 review articles, 57 not solely about lung cancer and 61 not about mediastinal staging). Of the 54 publications that remained, full manuscripts were obtained and a further 29 studies were excluded (1 not specifically pertaining to EBUS, 7 review articles, 5 not solely about lung cancer, 11 not about mediastinal staging and 5 that involved restaging. From the 25 publications deemed eligible for inclusion, 10 were excluded for repeat data and 5 because insufficient information was provided for data extraction (fig 1). Finally, data were extracted from 10 publications,10 11 12 13 14 15 16 17 18 19 of which 6 were full papers10 13 15 16 17 18 and 4 were published abstracts11 12 14 19 (tables 1 and 2). The details are listed in online Appendix B.

Data and search extraction. EBUS, endobronchial ultrasound.
Study characteristics
Study results
Quality assessment
Our application of the QUADAS tool revealed that there were generally low scores in all of the eligible papers. The highest score was only 9 out of a possible 14, the lowest was only 2, with a mean of 6.1.
Test performance
The point specificity for the pooled data was 1.00 (95% confidence interval (CI) 0.92 to 1.00, fig 2). Unlike tests of imaging compared with tissue diagnosis, EBUS-TBNA is a test that provides tissue, similar to the reference standard. It is therefore not surprising that the pooled specificity is 1.00 (all patients who are truly negative would not be expected to test positive on EBUS). However, it is important to note that, in one case,18 although EBUS-TBNA yielded a positive result, the reference standard was negative, accounting for the lower bound of the confidence interval of 0.92.
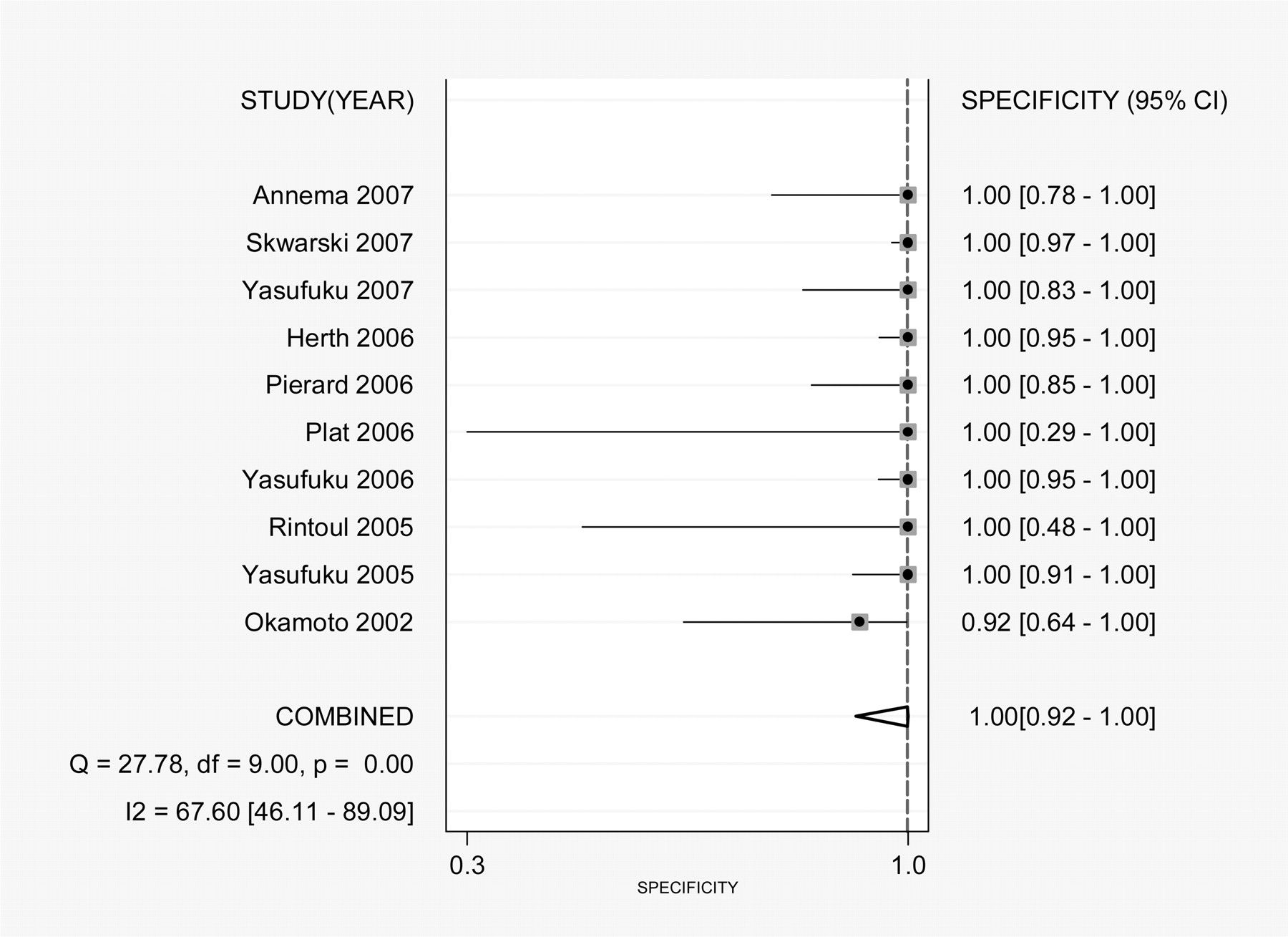
Forest plot of specificity.
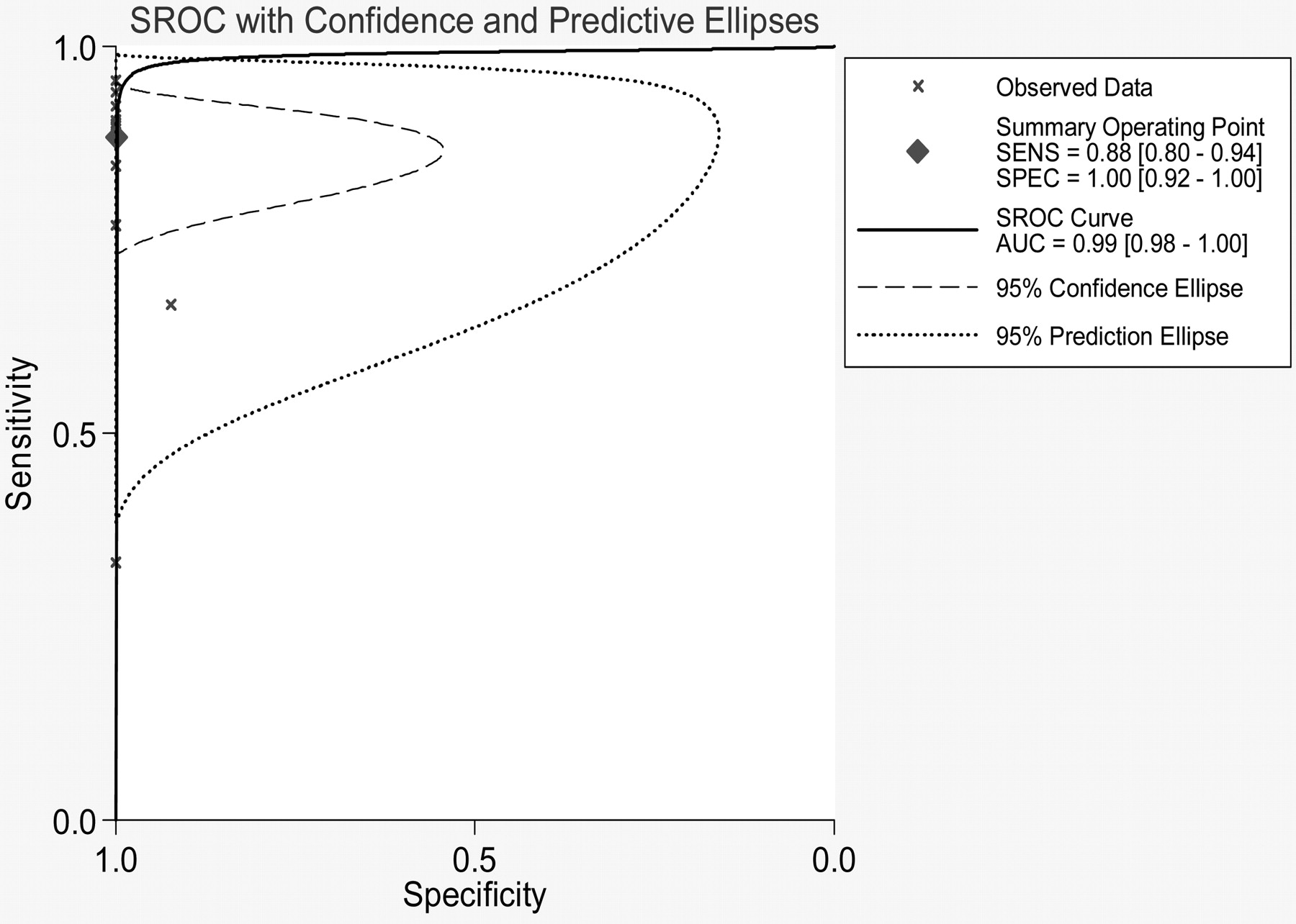
The point sensitivity for the pooled data was good at 0.88 (95% CI 0.79 to 0.94, fig 3) and the area under the summary receiver operating characteristics curve was 0.99 (95% CI 0.96 to 1.00, fig 4).

Forest plot of sensitivity.

{kind=link}
{kind=link}
{kind=link}
{kind=link}
Summary receiver operating characteristics (SROC) plot.
The results corresponded to a positive likelihood ratio of 680.86 (9.66 to 48000.00) and a negative likelihood ratio of 0.12 (0.06 to 0.21).
Discussion
The results of our study indicate excellent overall test performance as assessed by the area under the receiver operating characteristics curve. In addition, EBUS-TBNA had excellent specificity and good sensitivity. The pooled results of specificity of EBUS-TBNA (100%) compared favourably with a previously published meta-analysis that reported an overall specificity for CT of 79% and PET of 90%. The sensitivity was also favourable at 88% in comparison with reported pooled results for CT of 59% and PET of 81%.20
The favourable results of EBUS-TBNA compared with both CT and PET does not necessarily mean that it should be adopted as the investigation of choice for staging of mediastinal lymph nodes in patients with known or suspected lung cancer. Unlike diagnostic imaging techniques, EBUS-TBNA acquires tissue samples and is more invasive. There has been a report of torrential haemorrhage due to inadvertent biopsy of the pulmonary artery.21 In a number of the published studies, patients were admitted to hospital, anaesthetised and underwent a rigid bronchoscopy as well as EBUS-TBNA. However, this is not considered routine in clinical practice where the procedure is generally performed as a day case procedure with conscious sedation. Moreover, EBUS-TBNA can assess all lymph node stations in close proximity to the airway such as the paratracheal and subcarinal stations. Although this meta-analysis focuses on mediastinal staging, it should be noted that the endobronchial technique is also able to sample contralateral hilar lymph nodes. The main blind spots for EBUS-TBNA are the lymph nodes in the aortopulmonary window, para-aortic station, paraoesophageal stations and the inferior pulmonary ligament. In future, combination EBUS with endoscopic ultrasound (EUS) will increase the lymph nodes that are accessible using endoscopic techniques.
Integrated PET/CT carries additional advantages of screening for distant metastatic disease such as the adrenal glands and is likely to remain the initial screening investigation of choice. Surgical staging is considered the reference standard, but cervical mediastinosocpy can only sample lymph nodes in the paratracheal and subcarinal locations. Para-aortic, aortopulmonary window, paraoesophageal and inferior pulmonary ligament lymph nodes cannot be assessed unless more invasive access (mediastinotomy and video-assisted thoracoscopy) is employed.
It is likely that EBUS-TBNA will have an increasingly important role in staging the proximal mediastinal lymph node stations, especially in centres where mediastinoscopy and lymph node biopsy are not readily available or when the risks of surgical procedure are high (patients in poor health and those who have had a previous mediastinoscopy).
Limitations
There are a number of important limitations that may influence the interpretation of the results of this review. While there have been a large number of papers published on the subject, they emanate from only a small group of authors and therefore the excellent results are generated from only a handful of experts. We would be cautious about external validity and generalising the results to less well trained practitioners and to those starting out with this technique. A degree of publication bias must be expected as it is unusual for practitioners to publish their poor results. With regard to quality assessment, in general the included studies scored poorly when assessed by QUADAS. In many studies there was poor description of reference test performance (systematic nodal dissection or mediastinoscopy staging) and, as such, we were unable to comment on the accuracy of the reference standard.
Two of the studies used radial ultrasound followed by TBNA rather than real-time ultrasound.10 18 Owing to the small numbers, it was not possible to compute and compare separate estimates for formal statistical comparisons. However, the individual study results were felt to be in keeping with the overall pooled estimates.
It would be important for future studies to directly compare the results of CT, PET-CT, EBUS-TBNA, mediastinoscopy and systematic lymph node dissection for staging and to better define where EBUS might fit into the diagnostic algorithm in relation to mediastinoscopy and lymph node biopsies. As EBUS mediastinal staging becomes more available, it should be introduced with careful auditing of each individual’s results. Further studies in different institutions by different operators would greatly increase the external validity of the results of future meta-analyses on this topic.
Conclusion
The results of our study indicate excellent overall test performance and specificity of EBUS-TBNA when used for mediastinal lymph node staging in patients with lung cancer. In addition, the pooled test specificity and sensitivity compare favourably with published results for CT and PET. More work is required to directly compare the role of EBUS-TBNA in relation to mediastinoscopy and define its clinical utility in the era of integrated PET-CT.
Acknowledgments
The authors gratefully acknowledge the contribution of Mary Macdowell (Mount Sinai, USA) for the translation of articles published in Spanish and Tom Triebel (West Middlesex Hospital, UK) for translations of articles published in German.
REFERENCES
Supplementary materials
Web only appendix 64;9:757
Files in this Data Supplement:
Footnotes
▸ Appendices A and B are published online only at http://thorax.bmj.com/content/vol64/issue9
Competing interests None.
Provenance and Peer review Not commissioned; externally peer reviewed.