Article Text

Abstract
Background: Quadriceps weakness and loss of muscle mass predict mortality in chronic obstructive pulmonary disease (COPD). It was hypothesised that a reduced quadriceps cross-sectional area could be detected by ultrasound in patients with COPD compared with healthy subjects, and that measurements relate to strength and fat-free mass (FFM).
Methods: Rectus femoris muscle cross-sectional area (RFCSA) was measured by ultrasound and whole-body FFM estimated using electrical bioimpedance. Quadriceps strength was measured by maximum voluntary contraction and twitch tension (TwQ) following magnetic femoral nerve stimulation.
Results: 26 healthy volunteers of mean (SD) age 63 (9) years and 30 patients with COPD of mean (SD) age 67 (9) years and percentage predicted forced expiratory volume in 1 s (FEV1) 48.0 (20.8)% with a similar FFM (46.9 (9.3) kg vs 46.1 (7.3) kg, p = 0.193) participated in the study. Mean RFCSA was reduced in patients with COPD by 25% of the mean value in healthy subjects(−115 mm2; 95% CI −177 to −54, p = 0.001) and was related to MRC dyspnoea scale score, independent of FFM or sex. Maximum voluntary contraction strength was linearly related to RFCSA in patients with COPD (r = 0.78, p<0.001). TwQ force per unit of RFCSA was similar in both healthy individuals and those with COPD (mean (SD) 17 (4) g/mm2 vs 18 (3) g/mm2, p = 0.657). Voluntary contraction strength per unit of RFCSA was dependent on central quadriceps activation and peripheral oxygen saturation in COPD.
Conclusion: Ultrasound measurement of RFCSA is an effort-independent and radiation-free method of measuring quadriceps muscle cross-sectional area in patients with COPD that relates to strength.
Statistics from Altmetric.com
Even in non-cachectic patients with chronic obstructive pulmonary disease (COPD), quadriceps strength is typically reduced by up to 30% compared with healthy elderly subjects.1 Quadriceps strength has been shown independently to predict increased healthcare utilisation and mortality in COPD.2 3 In our cohort of patients with moderate to severe COPD, quadriceps strength together with age provided more powerful prognostic information than whole body fat-free mass (FFM) or forced expiratory volume in 1 s (FEV1).3 A related measure, mid-thigh cross-sectional area measured by computed tomography (CT), has also been shown to predict mortality.4
Quadriceps strength may be assessed by maximum voluntary contraction force, but maximum effort cannot be guaranteed and formal testing equipment is cumbersome.5 6 Effort-independent methods of assessing strength such as femoral nerve stimulation are expensive, not widely available and require specific expertise.7 Bedside tests are attractive for their simplicity and accessibility but measurement of thigh circumference, for example, may not accurately reflect the muscle compartment. Ionising radiation exposure makes serial measurements with CT4 or dual energy x ray absorptiometry scanning8 9 undesirable in large populations. MRI avoids this concern, but accessibility and long scanning times remain clinically relevant constraints.
Ultrasound can be used to assess limb muscle size and has been compared with CT and MRI in other research scenarios.10 11 While CT and MRI of the quadriceps are described in COPD,12 13 ultrasound is not widely used. Ultrasound equipment is available in most hospitals and, in principle, trained non-specialists could perform scans rapidly at the bedside. We hypothesised that ultrasound could detect reduced quadriceps muscle size in patients with COPD compared with healthy subjects. We wished to explore how muscle size measured in this manner correlated with quadriceps strength and FFM.
METHODS
Study design and participants
Community dwelling healthy volunteers and patients with stable COPD14 aged 40–90 years were invited to participate. Healthy subjects had an MRC dyspnoea score of 1,15 no spirometric evidence of airflow obstruction and reported no organ dysfunction or co-morbidity affecting the legs. Subjects with COPD were recruited from a respiratory outpatient clinic and had attended a pulmonary rehabilitation course in the preceding year. All were exacerbation-free for at least 4 weeks.
Participants underwent spirometry, FFM measurement and assessment of the right quadriceps. In addition they consented to undergo supplementary studies described below; participation in these additional tests was voluntary, unselected and intended to provide technical and supporting information only.
Measurements
Spirometry was performed according to international recommendations.14 16 FFM was determined by electrical bioimpedance (Bodystat 1500; Bodystat, Isle of Man, UK). A disease-specific equation was applied in patients with COPD.9 Quadriceps strength was assessed by isometric maximum voluntary contraction (QMVC) and twitch tension (TwQ) following supramaximal magnetic femoral nerve stimulation. QMVC was measured supine on custom-made apparatus based on that used by Edwards et al.5 Participants performed isometric contractions with the knee joint at 90° until consistent traces within 5% of the maximum were obtained. QMVC was taken as the highest mean tension maintained over 1 s. Twitch tension was measured using the method of Polkey et al.7 Unpotentiated twitches were obtained following 20 min quadriceps rest using a 70 mm figure-of-eight coil (Magstim, Whitland, UK). Non-supramaximal responses were discarded. A measure of voluntary quadriceps activation (twitch interpolation) was derived by superimposing twitches during the QMVC.6
Quadriceps ultrasound
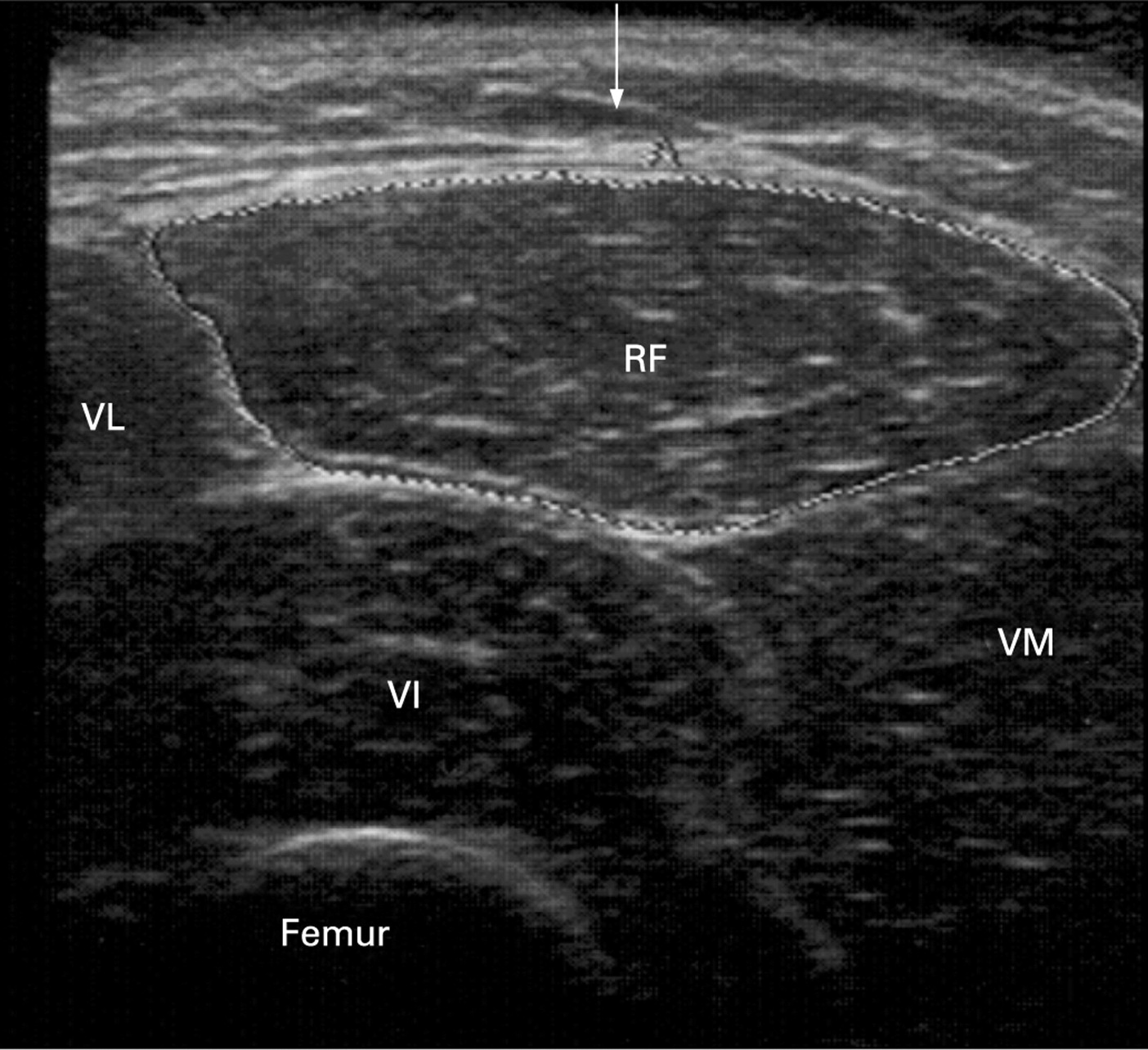
Cross-sectional area of the rectus femoris (RFCSA) was measured by B-mode ultrasonography using an 8 MHz 5.6 cm linear transducer array (PLM805, Toshiba Medical Systems, Crawley, UK), similar to the method of de Bruin et al.17 The transducer was placed perpendicular to the long axis of the thigh on its superior aspect, three-fifths of the distance from the anterior superior iliac spine to the superior patellar border. This was the highest point in the thigh that the entire rectus femoris cross-section could be visualised in a single field in all subjects; other muscles of the quadriceps group could not be encompassed in this manner. Imaging was conducted supine with the rested leg supported in passive extension. Excess contact gel was applied to minimise underlying soft tissue distortion. Oblique imaging was minimised by the operator (JS) using visual feedback to obtain the smallest cross-sectional image. Scanning depth was set to where the femur could be discerned for orientation. Gentle contraction-relaxation manoeuvres were employed to delineate muscle septa prior to image acquisition. RFCSA was calculated by a planimetric technique (Nemio, Toshiba Medical Systems) after the inner echogenic line of the rectus femoris was outlined by a movable cursor on a frozen image (fig 1). RFCSA was taken as an average of three consecutive measurements within 10%.

Ultrasound of the quadriceps. Sample ultrasonogram of the right quadriceps in a healthy woman aged 59 years. The arrow indicates the direction of the scan (5 cm scanning depth displayed). RF, rectus femoris; VL, vastus lateralis; VM, vastus medialis; VI, vastus intermedius.
Supporting studies
Although related information is described elsewhere,10 11 the findings of de Bruin et al did not report specific information regarding the relationship of the RFCSA and other scanning modalities such as CT. A subset of volunteers underwent CT scanning of the quadriceps for comparison with the ultrasound scans taken in this study. CT scans were performed using a Siemens SOMATOM Sensation 64-slice scanner, similar to the method of Bernard et al.12 Scans were taken at the mid-point of a line between the pubic symphysis and tibial plateau. Mid-thigh, quadriceps and rectus femoris muscle cross-sectional areas were calculated using Siemens SIENET software (MagicView VE 40) after manual outline with a movable cursor. Inter-occasion repeatability of right leg RFCSA measurement was assessed in a subset of healthy and COPD volunteers after an interval of 2–4 weeks, during which subjects continued their normal level of daily activity. Images and force traces were archived and analysed following completion of data collection. Inter-observer agreement was assessed between two observers (JS and PS), each blind to the other’s scans.
Statistical analysis
Based on previous data, 25 patients in each group were required for an 80% chance of detecting a 20% reduction in the mean TwQ of patients with COPD compared with healthy subjects at the 5% significance level.1 Similar to the source of this calculation, all volunteers were analysed prospectively; no direct case matching was performed. Differences were not sought between healthy subjects and those with COPD in the technical and supporting studies. Mean differences between healthy and COPD groups were analysed with unpaired t tests or Mann-Witney U tests; normality was assessed by the D’Agostino and Pearson omnibus method. Correlations were described using Pearson coefficients (or Spearman rho for non-normally distributed or categorical data) to two decimal places with accompanying two-tailed p values. Multiple linear regression analysed the relationship between RFCSA and FFM (the continuous variable) with sex and disease group as categorical variables. The MRC dyspnoea score was also included in an analysis of patients with COPD. Bland-Altman analysis18 described agreement between observers and interval RFCSA scans. Analysis and figure construction used SPSS Version 16.0 (SPSS Inc, Chicago, Illinois, USA) or GraphPad Prism Version 5.0 (GraphPad Software, San Diego, California, USA).
RESULTS
Participants
Thirty patients with stable COPD and 26 healthy volunteers participated in the study. The median MRC dyspnoea score was 3 (interquartile range 2.75–4.00) in patients with COPD. 25 were prescribed inhaled corticosteroid and 28 took at least one long-acting bronchodilator; none took oral corticosteroids. Baseline characteristics are shown in table 1.
Quadriceps strength and RFCSA
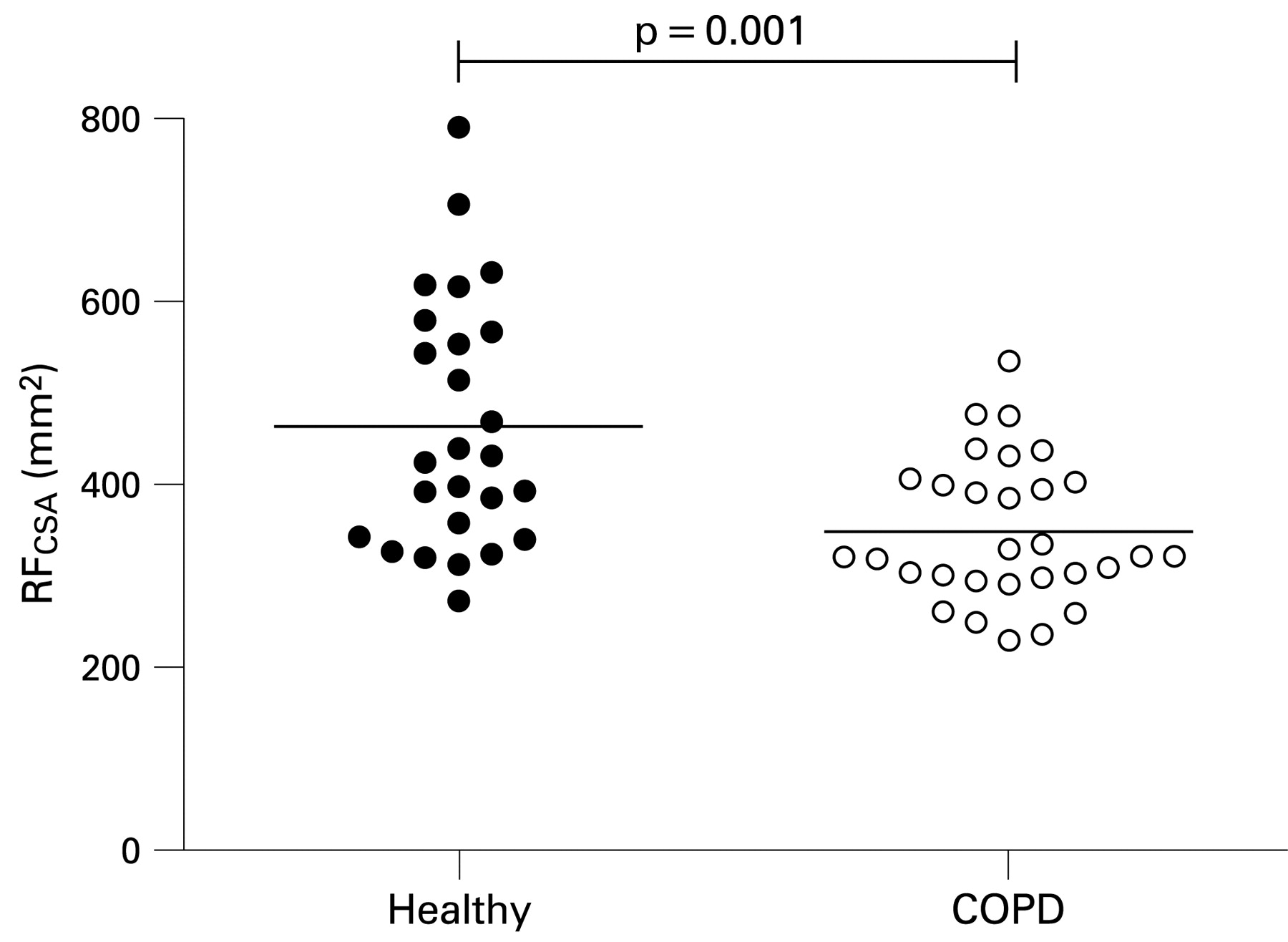
Supramaximal TwQ responses were unobtainable in one healthy subject and four with COPD. QMVC and TwQ were correlated with a Pearson coefficient of 0.81 (p<0.001). The TwQ/QMVC ratio was similar in healthy and COPD groups (median (IQR) 0.22 (0.20–0.28) and 0.25 (0.19–0.30), p = 0.359) as was twitch interpolation (0.90 (0.86–0.96) and 0.92 (0.82–0.95, p = 0.955). Individual RFCSA results are shown in fig 2. Mean group differences for quadriceps strength and RFCSA are shown in table 2.

Rectus femoris cross-sectional area (RFCSA, in mm2) in healthy subjects (solid circles) and subjects with chronic obstructive pulmonary disease (open circles). Horizontal lines indicate mean values.
Relationship between quadriceps strength and RFCSA
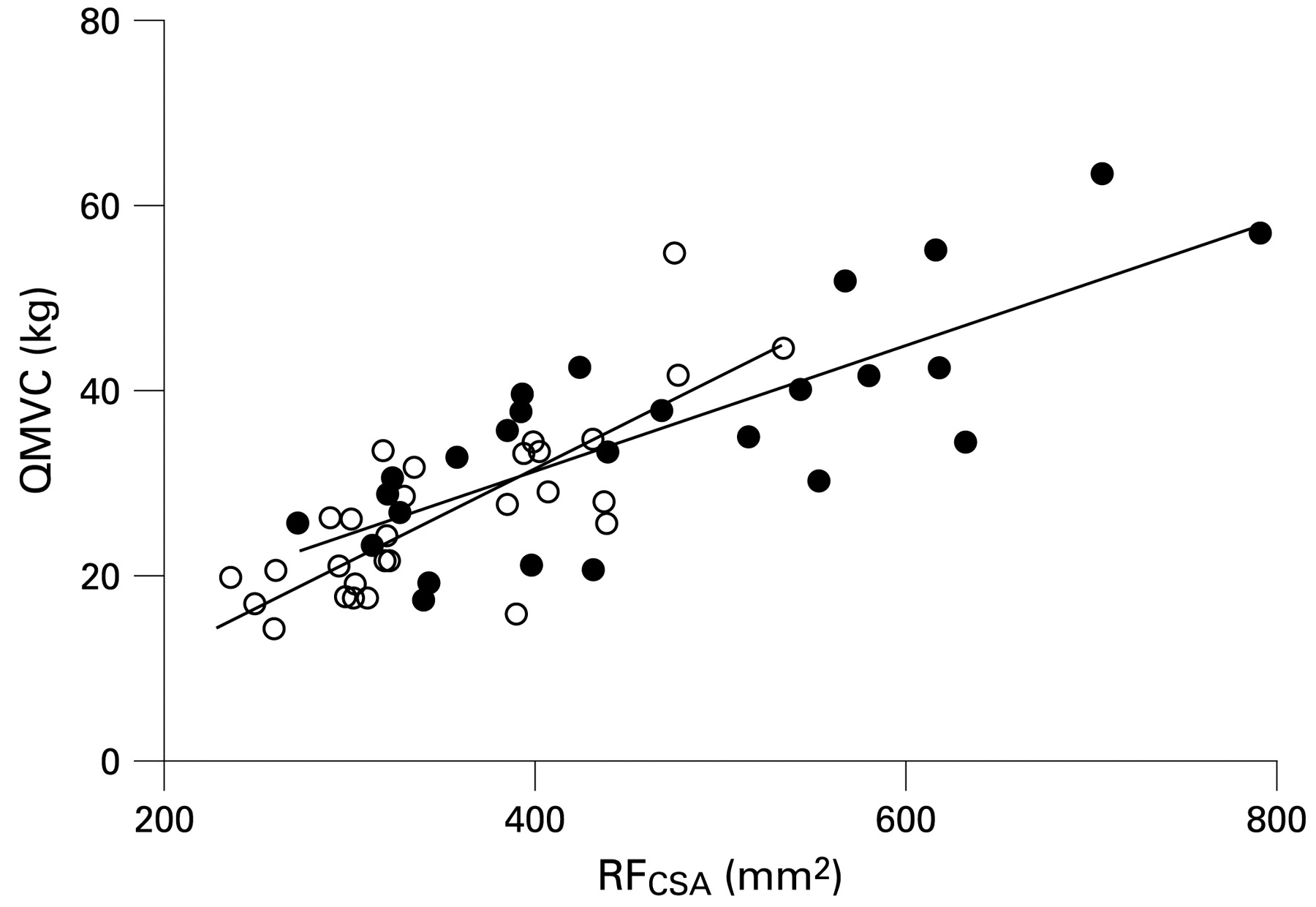
Quadriceps strength shared a linear relationship with RFCSA in both healthy subjects (QMVC, r = 0.80; TwQ, r = 0.72; p<0.001) and patients with COPD (QMVC, r = 0.78; TwQ, r = 0.69, p<0.001). The relationship was similar between groups (table 2, fig 3). Greater QMVC strength per unit of RFCSA correlated with higher twitch interpolation values in both groups. Greater QMVC/RFCSA was noted among healthy subjects with fewer recorded smoking pack years (r = 0.50, p = 0.009) and in patients with COPD with a higher resting Sao2 (r = 0.41, p = 0.025); neither correlated with TwQ/RFCSA or absolute QMVC.
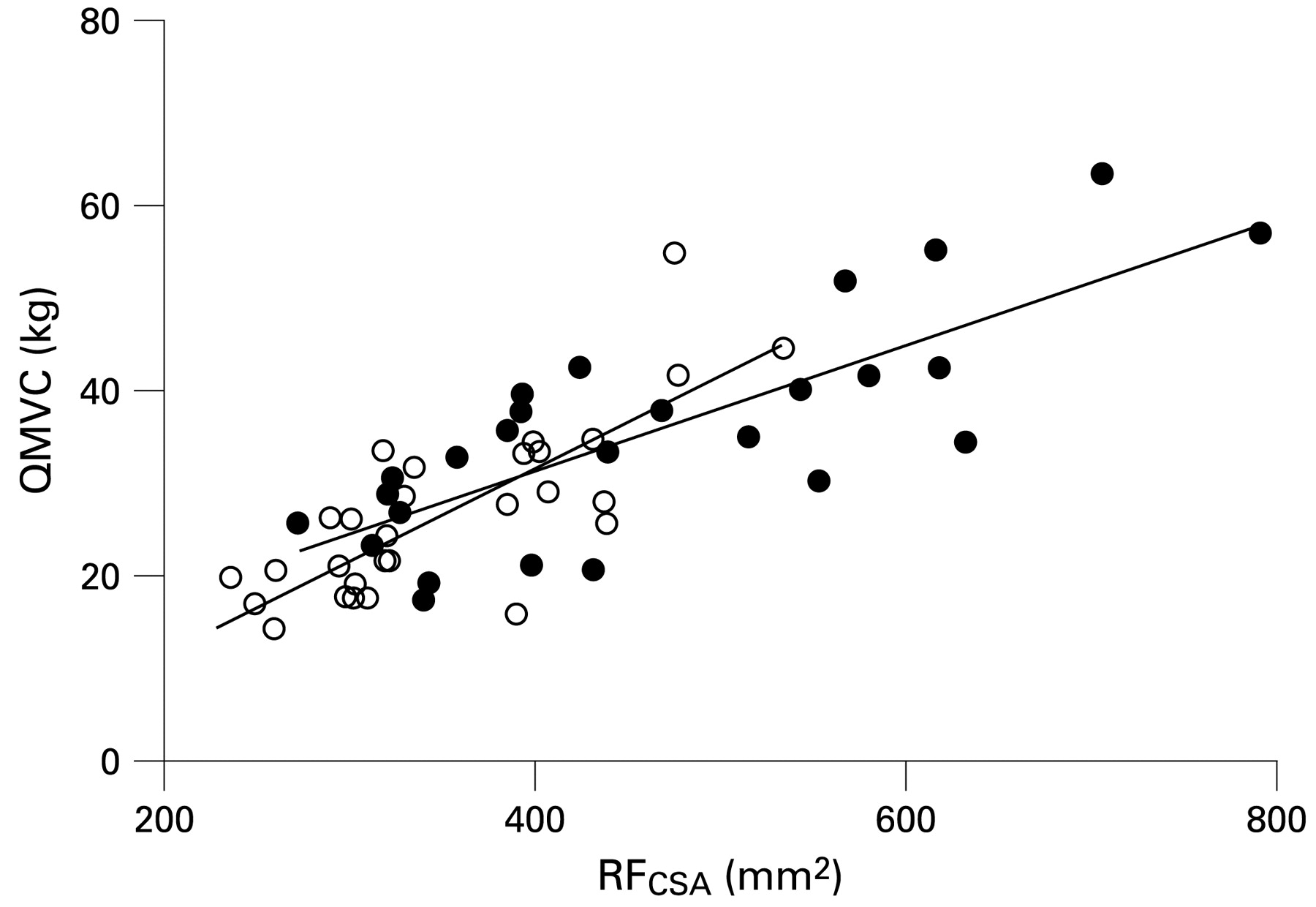
Relationship between rectus femoris cross-sectional area (RFCSA) and quadriceps maximum voluntary contraction (QMVC) in healthy subjects (solid circles) and subjects with chronic obstructive pulmonary disease (open circles). Regression lines for each group are superimposed. Combined regression equation for both groups given by: QMVC (in kg) = 0.077 × RFCSA (in mm2) − 0.28.
Relationship between rectus femoris size and FFM
QMVC, TwQ, RFCSA and FFM were significantly larger in men, irrespective of disease status (mean (SD) RFCSA in men 460 (133) mm2 vs 347 (83) mm2 in women, p<0.001). FFM, as opposed to weight, BMI or FFMI, displayed the closest correlations with RFCSA and quadriceps strength. Age did not determine RFCSA or quadriceps strength in those studied, nor did FEV1 or Sao2 among subjects with COPD.
RFCSA correlated with FFM in both healthy subjects (r = 0.66, p<0.001) and those with COPD (r = 0.43, p = 0.019); regression slopes were not significantly different (p = 0.263). The relation in healthy subjects remained significant (p = 0.024) when adjusted for greater RFCSA in men (table 3, model I), but was no longer significant in patients with COPD (p = 0.24, model II). Allowing for sex and the dependence of RFCSA on FFM, RFCSA was smaller in patients with COPD than in healthy subjects (−121 mm2 (95% CI −166 to −76), p<0.001). Analysis of MRC dyspnoea score as an independent variable showed that it explained more of the variation in RFCSA in patients with COPD than FFM and sex (models II and III) and, in a model with all three variables, remained statistically significantly associated with RFCSA while FFM and sex no longer showed a relation (model IV). This was not found to be the case with FEV1 or Sao2 if substituted for MRC score.
Supporting studies
Eighteen participants agreed to an additional CT scan of the quadriceps. RFCSA measured using ultrasound significantly correlated with that measured by CT (intraclass coefficient r = 0.88). No significant bias was associated with either modality. The relationship of RFCSA to the whole quadriceps cross-sectional area (QCSA) is shown in fig 4. The relationship between strength in these 18 subjects and the different measured cross-sectional variables on CT are described further in the online supplement.

{kind=link}
{kind=link}
{kind=link}
{kind=link}
Relationship between rectus femoris cross-sectional area (RFCSA) and total quadriceps cross-sectional area (QCSA) measured by CT scanning. Squares indicate individual results for RFCSA compared with the whole QCSA measured by CT scanning. Regression line (solid) and 95% confidence interval (dashed) shown. Eighteen subjects (10 with COPD, 8 healthy) underwent CT validation of the ultrasound measurements made in this study.
Nineteen volunteers underwent repeat measurement of RFCSA on two occasions. The mean (SD) bias and 95% limits of agreement were 12 (43) mm2 and −72 to +96 mm2. The coefficient of repeatability was 85 mm2 and index of reliability 0.97. The corresponding values for interobserver RFCSA measurement (n = 10) were 2 (32) mm2, −61 to +65 mm2, 64 mm2 and 0.99.
DISCUSSION
This study shows that ultrasound can generate a simple measure of quadriceps muscle cross-sectional area that is related to strength in both healthy persons and patients with COPD. The RFCSA was reduced in COPD by 25% of the mean value observed in a healthy population with a similar FFMI.
Experimental critique
Inter-observer and inter-occasion agreements for ultrasound RFCSA measurement were comparable to other reported clinical ultrasound measures (eg, carotid artery intimal thickness19). Measurement differences are probably operator-related, such as oblique imaging of the RFCSA or placement of an inaccurate cursor outline for area calculation. Previous studies suggest that differences between serial CT or MRI cross-sectional area measurements20 21 are smaller than those observed for ultrasound. Certainly these modalities can use bony landmarks for position more accurately than surface anatomy. Ascertaining the scanning point between visits seems important as evidenced by the narrower inter-observer limits of agreement (when RFCSA is measured at a marked point). Related ultrasound measurements have studied the response to training;22 23 it remains to be investigated whether rectus femoris ultrasound is useful for assessing interventions or longitudinal change in COPD.
A clinician without prior ultrasound experience performed the RFCSA measurements following 2 weeks of familiarisation. Scanning was completed more quickly than the quadriceps strength assessment. Visualisation of the rectus femoris border was subjectively easier when less subcutaneous fat was present and RFCSA may therefore be unmeasurable in severely obese subjects. Adequate visualisation of intermuscular septa may also be problematic if body fat is grossly depleted.20 Measurement of quadriceps muscle thickness24 rather than cross-sectional area may be more feasible in such scenarios; however, our personal experience suggests that any excess compression by the ultrasound probe is likely to introduce additional measurement variability. Serial measurements of quadriceps muscle thickness have been studied in an intensive care unit (ICU) population;24 however, poor or absent correlations between muscle layer thickness and strength have previously been reported.25
Using RFCSA as a measure of quadriceps size assumes that all four muscles of the quadriceps group atrophy by a similar amount. Indeed, this pattern has been observed in age-related muscle loss.26 The relationship between RFCSA and quadriceps cross-sectional area also suggests this may be a reasonable assumption, but the rectus femoris only constitutes approximately 10% of the total quadriceps cross-sectional area.26 Muscle size as measured by RFCSA correlated well but not perfectly with maximum voluntary contraction strength in COPD (r = 0.80 with QMVC). A comparable coefficient (0.73) originally described the relationship between strength and total mid-thigh cross-sectional area measured by CT.12 In the 18 subjects who underwent CT scanning, correlations were only slightly improved with cross-sectional measures that included the whole quadriceps muscle (see table S2 in online supplement). Additional variation in the relationship between strength and muscle size may arise from differences in muscle quality which were not specifically sought in this study. Reduced tension generation associated with increased muscle lipid content27 or altered muscle fibre pennation angles23 have been reported in other conditions.
Although QMVC and TwQ shared a similar relationship with RFCSA in both healthy subjects and patients with COPD, the level of central activation measured by twitch interpolation influenced QMVC force produced per unit of muscle size, as did peripheral oxygen saturation in the patients with COPD. Given that peripheral oxygen saturation had no relationship with TwQ per RFCSA or absolute MVC, this suggests that volitional measures requiring a degree of physical exertion are subject to additional factors in COPD.
Significance of findings
In two previous studies the prevalence of quadriceps weakness in COPD has been found to exceed that of whole body FFM depletion.8 28 In the present study FFM was more closely correlated with RFCSA in healthy subjects than in those with COPD. However, the interpretation of the disparity between FFM and RFCSA depletion warrants caution. FFM calculation in COPD is dependent on electrical bioimpedance and body water content. Group differences in hydration status (or diuretic usage, taken in five patients with COPD and two healthy subjects for uncomplicated essential hypertension) cannot be ruled out. Nevertheless, excess lower limb muscle loss or preferential quadriceps wasting within the leg could also underlie this disparity. For example, the quadriceps may be more sensitive to mechanical unloading associated with inactivity while other leg muscles are relatively preserved; other leg muscle groups were not studied in order to qualify this hypothesis. An increased MRC dyspnoea score (assigned according to breathlessness at different levels of general activity) was related to a reduced RFCSA in COPD, independent of FFM or sex. As well as providing prognostic information, the MRC score relates to more detailed quality of life measures29 30 and the observed relationship may be in keeping with a model of quadriceps weakness driven by inactivity.
A pilot study of serial RFCSA measurement in ICU patients is summarised in table S1 in the online supplement. An 18% reduction in the baseline RFCSA was observed in an unselected sample of six subjects over 10 days. Comparable reductions in quadriceps strength have been reported in healthy bedbound individuals after 10 days.31 Future studies may find ultrasound measurement of the rectus femoris a useful tool for monitoring change which, given the findings described here, may also permit inferences about muscle strength. We caution that a much larger study would be necessary to validate this contention, ideally with parallel measurement of body water and other radiological and muscle contractility assessments.
Improved exercise capacity in advanced COPD can be achieved without a change in lung function, such as following pulmonary rehabilitation. There is likely to be an increased focus on the selection and assessment of patients referred for rehabilitation, including the identification of those with wasted or weak quadriceps muscles.32 Certain patients may benefit from advanced techniques such as adjunctive non-invasive ventilation or neuromuscular electrical stimulation. Novel pharmacological interventions may eventually become available which could augment or extend the benefit of rehabilitation on skeletal muscle performance.33 Thus, near patient quadriceps assessment may prove increasingly useful in COPD; rectus femoris ultrasound has the advantage of being relatively straightforward to learn, effort-independent and free of ionising radiation.
In summary, ultrasound can obtain a measure of quadriceps size at the bedside that is related to maximum isometric strength. Similar to others, we observed a weaker association between quadriceps muscle bulk and FFM in patients with COPD, suggesting that direct lower limb muscle assessment—whether by ultrasound, CT or strength measurement—is important. Muscle force produced per unit of muscle size during volitional quadriceps strength assessment is dependent on factors extrinsic to the muscle and highlights the importance of patient motivation and cooperation when making such measurements. Ultrasound may prove useful when assessing the quadriceps in COPD or other conditions if non-volitional strength assessment or other scanning modalities are unavailable or impractical.
REFERENCES
Supplementary materials
Web only appendix 64;5:418-23
Files in this Data Supplement:
Footnotes
Additional tables and figures are published online only at http://thorax.bmj.com/content/vol64/issue5
Funding: JMS was funded by a grant from the British Lung Foundation (PO4/8), and was the recipient of an educational grant from GlaxoSmithKline administered by the Royal Brompton Hospital, London. KW was funded by the Stroke Association and the Medical Research Council (UK). JSS was funded by a European Respiratory Society Research Fellowship. CJJ was funded by the Medical Research Council (UK).
Competing interests: None.
Ethics approval: King’s College Hospital local research ethics committee approved the study and informed consent was obtained.