Article Text

Abstract
Background: Chronic obstructive pulmonary disease (COPD) is often associated with peripheral muscle weakness, which is caused by several factors. Acute exacerbations may contribute, but their impact on muscle force remains unclear. Correlations between peripheral muscle force and inflammatory and anabolic markers have never been studied in COPD. The effect of an acute exacerbation on quadriceps peak torque (QPT) was therefore studied in hospitalised patients, and the aforementioned correlations were examined in hospitalised and in stable patients.
Methods: Lung function, respiratory and peripheral muscle force, and inflammatory and anabolic markers were assessed in hospitalised patients on days 3 and 8 of the hospital admission and 90 days later. The results on day 3 (n=34) were compared with those in clinically stable outpatients (n=13) and sedentary healthy elderly subjects (n=10).
Results: Hospitalised patients had lowest mean (SD) QPT (66 (22)% predicted) and highest median (IQR) levels of systemic interleukin-8 (CXCL8, 6.1 (4.5 to 8.3) pg/ml). Insulin-like growth factor I (IGF-I) tended to be higher in healthy elderly subjects (p=0.09). QPT declined between days 3 and 8 in hospital (mean −5% predicted (95% CI −22 to 8)) and partially recovered 90 days after admission to hospital (mean 6% predicted (95% CI −1 to 23)). QPT was negatively correlated with CXCL8 and positively correlated with IGF-I and lung transfer factor in hospitalised and in stable patients.
Conclusions: Peripheral muscle weakness is enhanced during an acute exacerbation of COPD. CXCL8 and IGF-I may be involved in the development of peripheral muscle weakness in hospitalised and in stable patients with COPD.
- chronic obstructive pulmonary disease
- interleukins
- IGF-I
- peripheral muscle force
Statistics from Altmetric.com
Chronic obstructive pulmonary disease (COPD) is a progressive and irreversible airway disease which seriously affects peripheral muscle force.1 Peripheral muscle weakness may, in turn, result in reduced exercise capacity,2 higher use of healthcare resources,3 or decreased survival.4,5 An extensive body of literature indicates that peripheral muscle weakness is of multiple origin.1 The relative contribution of these factors is poorly understood. We hypothesise, however, that steroid treatment6 and changes in the nutritional, metabolic, inflammatory, and oxidative states at the time of an acute exacerbation may contribute to a decrease in peripheral muscle force.7–12 Although patients with COPD frequently experience acute exacerbations,13 the clinical course of peripheral muscle force during an acute exacerbation has never been studied.
Systemic levels of insulin-like growth factor I (IGF-I) and of inflammatory markers may also be important in the development of skeletal muscle weakness in COPD.14–17 IGF-I, which is a major growth promoting factor, appears to be low in COPD.18 Its relationship with muscle force is unknown. It has been speculated that peripheral muscle force is inversely related to tumour necrosis factor alpha (TNF-α) and interleukin (IL)-6.1 So far, only negative correlations between indirectly estimated skeletal muscle mass and IL-6, TNF-α and its receptors have been observed in clinically stable COPD.19 Moreover, data from patients admitted to hospital during an acute COPD exacerbation are not available.
Interleukin 8 (CXCL8) is a chemoattractant cytokine which is thought to be a very important regulator of the local bronchial inflammatory response in COPD.20 There is some evidence to suggest that CXCL8 might play a role in peripheral muscle wasting in myositis,21 but a relationship between CXCL8 and peripheral muscle weakness in patients with COPD has never been studied.
A study was undertaken to investigate the clinical course of quadriceps force during an acute COPD exacerbation and to investigate the correlations of quadriceps force with systemic levels of IGF-I, IL-6, CXCL8, and TNF-α in hospitalised and in stable patients.
METHODS
Study design
Thirty four patients with COPD (forced expiratory volume in 1 second (FEV1)/forced vital capacity (FVC) <70%) consulted the emergency department because of deterioration in their respiratory status.22 The decision to admit patients to the hospital was made by the attending chest physician who was not familiar with the present study protocol. The presence of purulent sputum was documented in 22 patients. In addition, 22 patients were classified as having a type 1 exacerbation, eight had a type 2 exacerbation, while four others had a type 3 exacerbation.22 Patients admitted to hospital received oral methylprednisolone 32 mg/day for 1 week, followed by 24 mg/day for 4 days and a subsequent decrease of 4 mg/week. On day 3 of the hospital admission venous blood was taken and pulmonary function,23 maximal inspiratory mouth pressure (Pimax),24 handgrip force (HGF),25 and quadriceps peak torque (QPT)26 were measured. The results in the hospitalised patients (day 3) were compared with those of 13 consecutive patients with clinically stable COPD who visited the outpatient clinic (FEV1/FVC <70% and no hospital admissions due to acute exacerbations during the year before testing). Moreover, 10 sedentary healthy elderly subjects (normal pulmonary function and no active participation in sporting activities) were recruited from relatives of students at the faculty of physical education and physiotherapy. Patients with stable COPD and the sedentary healthy elderly subjects were matched for sex and age and performed the previously mentioned tests in an outpatient setting. Table 1 summarises the characteristics and physiological data of the three groups.
Characteristics and physiological data of hospitalised COPD patients, clinically stable COPD patients, and healthy elderly subjects
The tests were repeated on day 8 of the hospital stay and 90 days after admission in the hospitalised patients. Nine patients were excluded from the analysis to determine changes between days 3 and 8 of the hospital stay. Two patients were discharged before day 8. In four others blood was not taken to assess systemic CXCL8, and three patients were reluctant to repeat the QPT test. The patients who dropped out had comparable characteristics to those of the 25 patients who were tested on day 8 (QPT at day 3, 67 (17)% predicted). The drop out was therefore random among the patients with COPD and was not limited to those patients who were worse initially.
Between days 8 and 90, 12 patients dropped out because of poor compliance with the study protocol. This may bias the results by the fact that the patients who were compliant with their 90 day appointment were better at day 8 (mean (SD) QPT 72 (18)% of the predicted value) than those who dropped out (mean (SD) QPT 50 (21)% of the predicted value).
The ethics committee of the University Hospitals Leuven granted approval for this cross-sectional and longitudinal study. The participants (all men) gave oral and written informed consent.
Blood sample analyses
Venous blood was drawn from supine subjects between 08.15 and 09.00 hours, before any exercise testing was done. Samples were drawn in evacuated tubes coated with lithium heparin (for C-reactive protein (CRP)), clot activator silica (for IGF-I), or potassium ethylenediaminetetraacetic acid (for IL-6, CXCL8, IL-10 and TNF-α) (Becton Dickinson Vacutainer Systems, Plymouth, UK). The systemic levels of CRP and IGF-I were determined using an immunoturbidimetric assay (Roche Diagnostics Corporation, Indianapolis, IN, USA) and a radioimmunoassay (Nichols Institute Diagnostics, San Juan Capistrano, CA, USA), respectively, according to the manufacturers’ specifications. The systemic levels of IL-6, CXCL8, IL-10, and TNF-α were determined using Human Inflammation Cytometric Bead Array (Becton Dickinson Biosciences, San Diego, CA, USA).27 In brief, cytometric bead array employs a series of particles with discrete fluorescence intensities to simultaneously detect multiple soluble analytes in a small serum sample (50 μl). Data were obtained and analysed using an FACScan flow cytometer and Cell Quest software. The lower detection limit for cytometric bead array was 1.0 pg/ml.
Statistical analyses
Mean (SD) values were calculated. Non-normally distributed variables were expressed as median (interquartile range (IQR)) and were logarithmically transformed (log) for further analyses. The three groups were compared using one way analysis of variance (parametric variables) or a Kruskal-Wallis test (non-parametric variables). Only when the p value was below 0.05, a post hoc test was performed. Some participants of all groups had values below the detection limit for CRP, IL-6, or IL-10. Nevertheless, all data were included by using the detection limit as the value for those values below the limit (3.0 mg/l and 1.0 pg/ml, respectively).
Changes during the stay in hospital and between day 8 of the hospital admission and 90 days afterwards were analysed using a Mann-Whitney U test (non-parametric variables) or a paired t test (parametric variables). A Pearson product moment correlation test was performed to assess relationships, and a stepwise multiple regression analysis was carried out to assess independent contributors to the variance in QPT in hospitalised COPD patients. A priori, a two sided level of significance was set at 0.05.
RESULTS
Cross-sectional comparison
Hospitalised (day 3) and clinically stable COPD patients had moderate to severe airflow obstruction, moderately reduced arterial oxygen tension, and impaired respiratory and peripheral muscle force (table 1). Hospitalised patients had lowest body mass index (BMI), HGF, and QPT. CRP and CXCL8 levels were highest in hospitalised COPD patients (table 2). IL-6 did not differ significantly between the three groups. TNF-α was only detectable in one hospitalised and in one clinically stable COPD patient (9.3 and 1.6 pg/ml, respectively). Systemic IGF-I tended to be highest in healthy sedentary elderly subjects (p=0.09).
Systemic levels of inflammatory and of anabolic markers
Longitudinal changes
Retrospectively, systemic CRP levels at day 1 (emergency room) were retrieved from the patients’ files. On day 1 of the hospital admission CRP was detected in 88% of patients (median (IQR) 28 (11–86) mg/l). The systemic levels of CRP decreased significantly between days 1 and 3 (median −14.1 mg/l (95% confidence interval (CI) −153.8 to 0.6), p=0.0001) and between days 3 and 8 (median −2.6 mg/l (95% CI −27.0 to 9.4), p=0.02). Furthermore, QPT decreased by a mean of 5% of the predicted value (95% CI −22 to 8, p=0.05, fig 1) and FEV1 had a strong tendency to increase (mean 2.2% of predicted value (95% CI −5.8 to 10.7), p=0.06) between days 3 and 8. Other variables did not change significantly during the hospital stay.

Decrease in quadriceps peak torque (QPT, expressed in Newton-metres, Nm) between days 3 and 8 of hospital admission followed by a significant increase at 90 days.
Between day 8 of hospitalisation and 90 days after discharge FEV1 (mean 6% of predicted value (95% CI −16 to 22), p=0.10), QPT (mean 6% of predicted value (95% CI −1 to 23), p=0.008, fig 1), and IGF-I (median 38 μg/l (95% CI −38 to 103), p=0.02) increased significantly.
Correlations
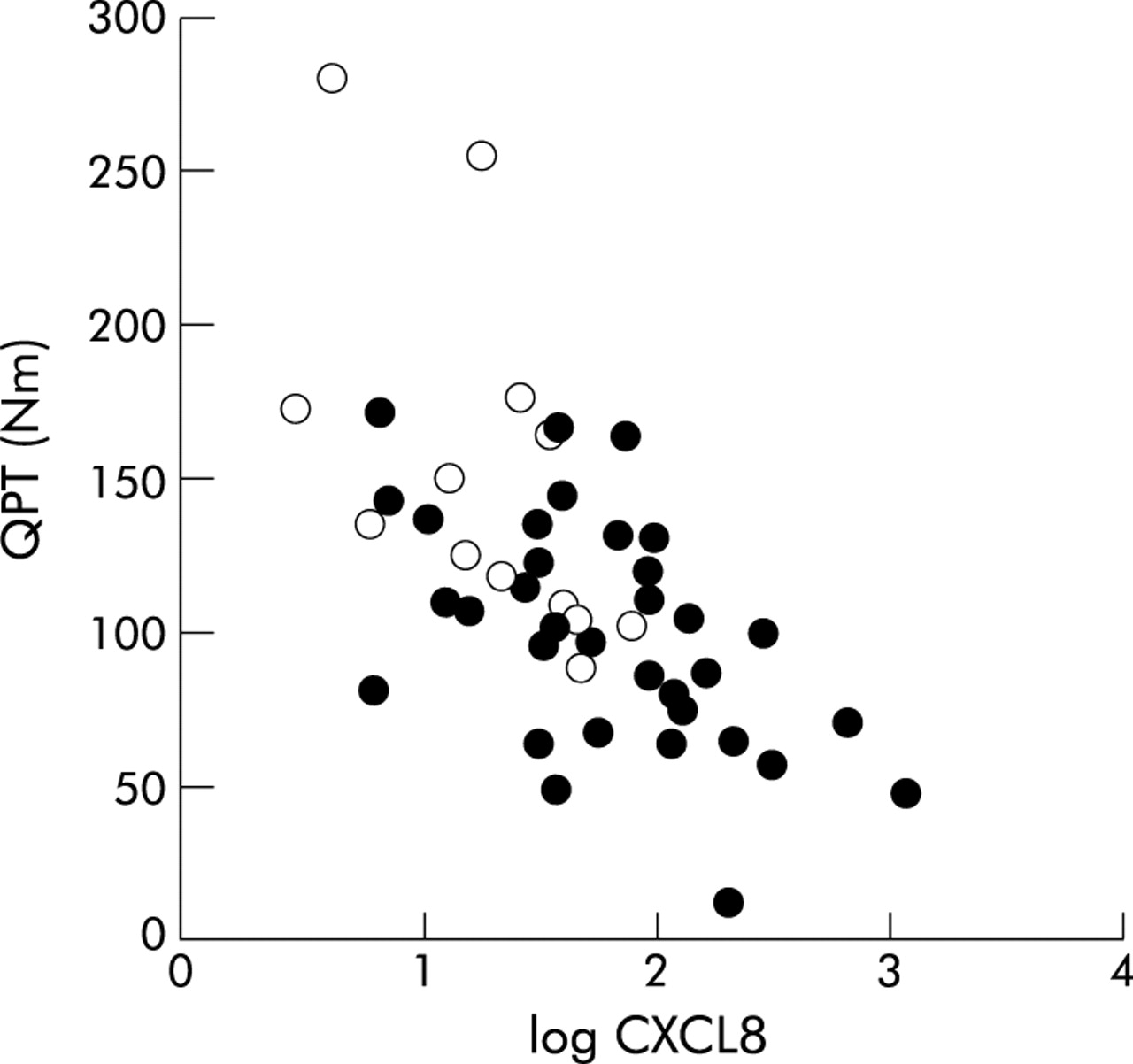
The relationships between QPT, pulmonary function, and systemic levels of inflammatory and anabolic markers in hospitalised patients (day 3), stable patients, and in sedentary healthy elderly subjects are shown in table 3 and fig 2. Briefly, QPT was inversely correlated with log CXCL8 and with log IL-6 in hospitalised COPD patients. The relationship with log CXCL8 was also present in patients with stable COPD.
Correlations between quadriceps peak torque, pulmonary function, and systemic levels of inflammatory and anabolic markers

{kind=link}
{kind=link}
Inverse correlation between quadriceps peak torque (QPT, expressed in Newton-metres, Nm) and logarithmically transformed interleukin 8 (log CXCL8) in hospitalised (day 3, •) and clinically stable patients with COPD (○).
In contrast to the patients with stable COPD (r=–0.13, p=0.71) and the healthy controls (r=0.13, p=0.67), HGF was associated with log CXCL8 in the hospitalised patients (r=–0.39, p=0.02). Moreover, log CXCL8 was significantly associated with Tlco in hospitalised and in stable COPD patients (r=–0.41, p=0.02; and r=–0.56, p=0.05, respectively). A stepwise multiple regression analysis showed that age, transfer factor, and log CXCL8 were significant determinants of QPT in hospitalised COPD patients at day 3. This model explained 59% of the variance in QPT (p=0.01).
DISCUSSION
This study clearly demonstrated lower peripheral muscle force and higher systemic inflammation on day 3 of hospitalisation for an acute COPD exacerbation compared with stable COPD patients and healthy elderly subjects. Furthermore, peripheral muscle force declined throughout the hospital admission and partially recovered 90 days after discharge. Peripheral muscle force was positively correlated with systemic IGF-I levels and pulmonary function, and negatively with systemic CXCL8 levels in hospitalised and in stable COPD patients.
Changes in peripheral muscle force
Peripheral muscle weakness is a well known systemic feature in patients with clinically stable COPD.28 This is the first study to show a pronounced muscle weakness in hospitalised COPD patients compared with stable patients. Inpatients also had lowest BMI and hence, presumably, the lowest muscle mass.29 The reduction in QPT, however, remained (61 (21)% predicted) when the analysis was limited to hospitalised patients with a BMI of ⩾ 24 kg/m2 (n=16, BMI 28 (3) kg/m2). Consequently, the reduction in muscle force in hospitalised COPD patients cannot solely be due to loss of body weight. To determine the mechanism by which muscle force is reduced is beyond the scope of this paper.30
This study is the first to show a significant decrease in peripheral muscle force during an acute exacerbation in hospitalised COPD patients. Several factors may be related to this decrease. Changes in the nutritional, metabolic, oxidative, and inflammatory state have been observed at the time of an acute COPD exacerbation.7–9,11,12 In addition, bed rest31 and treatment with oral methylprednisolone may result in a rapid decrease in muscle force.26 Besides reducing muscle mass, corticosteroid treatment can also result in a reduction in muscle force per unit cross sectional area.26,28 The dose of oral methylprednisolone, however, is unlikely to play a decisive role in the present study as all hospitalised patients received a similar dose, and no relationship was found between the dose of oral methylprednisolone and the changes in muscle force between days 3 and 8.
Although patients did not conduct any structured exercise programme during the 90 day recovery period after hospitalisation, QPT increased by a mean of 8% of the value on day 8. This improvement is probably due to the reversibility of the systemic effects of an acute exacerbation on the nutritional and metabolic states, oxidative stress, and inflammation, together with increased daily physical activity. Nevertheless, the reported improvements in QPT of about 30% after local dynamic strengthening exercises or after whole body endurance exercises in COPD32 by far exceeds the spontaneous recovery observed in the present study. An exercise training programme following acute exacerbations still therefore appears to be potentially beneficial in COPD.
Peripheral muscle force and IGF-I
Systemic IGF-I levels tended to be lower in patients with COPD than in healthy controls (table 2). Low systemic IGF-I levels have been reported previously in COPD.18 The positive relationship between IGF-I levels and QPT in hospitalised patients and those with stable COPD (table 3) suggests a possible involvement of IGF-I in the development of peripheral muscle weakness. In the present study, however, only systemic IGF-I was determined. Autocrine/paracrine IGF-I production of peripheral muscles was not addressed. Discrepancies between systemically and locally produced IGF-I have been reported in patients with chronic heart failure33 and in healthy elderly subjects.34
Peripheral muscle force and systemic inflammation
Based on findings in animals,35,36 healthy elderly subjects,17 and chronic patients,16,19 it has been suggested that peripheral muscle force might be negatively related to the inflammatory state in COPD.1 This study is the first to substantiate this hypothesis. IL-6 and CXCL8 were inversely related to QPT (table 3). It is remarkable that CXCL8 was the only systemic inflammatory marker to contribute independently to the variance in QPT in hospitalised COPD patients. The present observation, though surprising, is in keeping with several lines of evidence available in the literature. It has been shown that CXCL8 might be involved in the loss of muscle mass in children with myositis, and systemic levels of CXCL8 (r=0.45) and TNF-α (r=0.37) were significantly associated with systemic levels of creatine kinase (the iso-enzyme of peripheral muscle that indicates muscle damage).21 Furthermore, proteolysis inducing factor, which initiates muscle proteolysis,37 induces systemic CXCL8.38 Thus, high levels of systemic CXCL8 may reflect the degree of muscle wasting and, hence, muscle weakness.
In a previous study carbon monoxide transfer factor and systemic inflammation (IL-6 and TNF-α) explained 32% and 40%, respectively, of the variance in peripheral muscle mass in patients with stable COPD.19 However, based on the relationship between transfer factor and systemic inflammation shown in healthy elderly smokers39 and in patients with COPD in the present study, these factors are likely to be interrelated.
Limitations of the study
This study has clear limitations. Firstly, tests applied to measure muscle force in the present study are motivation dependent. For QPT, however, the variability in maximal voluntary contractions was found to be similar to measurements by magnetic stimulation.40 Secondly, TNF-α was detectable in only 4% of the patients. This is in line with the findings of Schols and co-workers41 but in contrast to those of De Godoy et al.42 Methodological differences are likely to explain this discrepancy. Indeed, TNF-α is difficult to measure.19,43 Nevertheless, based on the increased CRP levels on day 1 of hospitalisation in the present study, as in previous studies,7–9 we can safely conclude that increased systemic inflammation was present in our hospitalised patients. Thirdly, a cross-sectional design is not adequate to establish a causal relationship between systemic CXCL8 levels and QPT. It was, however, the only systemic inflammatory marker that significantly contributed in the stepwise multiple regression analysis. Fourthly, at first sight it could be argued that the hospitalised and stable COPD patients may have a different degree of airflow obstruction. However, pulmonary function decreased at the onset of acute exacerbations and recovered 90 days later.44 We have previously found an increase in FEV1 of 8% predicted after admission to hospital.45 Based on these results, matching was performed which, in retrospect, appeared appropriate.
Conclusions
Muscle force was found to be significantly reduced in patients admitted to hospital with COPD and is subject to change during and after an acute exacerbation. This study is the first to show correlations between peripheral muscle force and systemic levels of IGF-I and CXCL8 in patients with COPD. The mechanisms underlying the change in peripheral muscle force and its relationship with CXCL8 and IGF-I need further investigation.
Acknowledgments
The authors are grateful to the respiratory nurses of the pneumology ward E650 of the University Hospital Gasthuisberg for taking the blood samples and to Leen Luyts for her technical assistance with the processing and the analyses of the serum. The authors also thank Professor Dr J L Ceuppens for his suggestions to the manuscript and the physiotherapists I Coosemans and L Herremans for testing all the subjects.
REFERENCES
Footnotes
-
This study was supported by Fonds voor Wetenschappelijk Onderzoek-Vlaanderen (FWO) grants # G.0237.01 and # G.0175.99, and FWO Levenslijn grant # 7.0007.00. TT and GGR are postdoctoral fellows of the FWO-Vlaanderen.
Linked Articles
- Airwaves