Article Text

Abstract
Background: Chronic thromboembolic pulmonary hypertension (CTEPH) can be successfully treated surgically by pulmonary thromboendarterectomy (PTE) but there are few data on mid-term cardiopulmonary function, particularly on exertion, and clinical benefits following pulmonary PTE.
Methods: A 2 year follow up study was undertaken of clinical status, haemodynamic and lung function indices, gas exchange, and exercise tolerance in 38 patients of mean (SD) age 50 (15) years who had undergone PTE.
Results: In-hospital mortality was about 10%. Before PTE all the patients were severely impaired (NYHA classes III–IV). There was no time difference in the improvement in the parameters: nearly all the improvement in cardiac output, gas exchange, and clinical status was achieved in the first 3 months as a result of the relief of pulmonary obstruction. At 3 months the percentage of patients with normal cardiac output and Pao2 and of those with reduced clinical impairment increased to 97%, 59%, and 87%, respectively, without any further change. Only mean pulmonary artery pressure (mPAP), carbon monoxide transfer factor (Tlco), and exercise tolerance improved gradually during the second year, probably due to the recovery of the damaged small vessels. Tlco was overestimated before PTE but afterwards the trend was similar to that of mPAP.
Conclusions: At mid term only a few patients did not have a satisfactory recovery because of lack of operative success, hypertension relapse, or the effect of preoperative hypertension on vessels in non-obstructed segments. Most of the patients, even the more compromised ones, had excellent long lasting results.
- pulmonary embolism
- endarterectomy
- pulmonary function tests
- CO, cardiac output
- CTEPH, chronic thromboembolic pulmonary hypertension
- CVP, central venous pressure
- FEV1, forced expiratory volume in 1 second
- FVC, forced vital capacity
- mPAP, mean pulmonary artery pressure
- Pao2
- Paco2, arterial oxygen and carbon dioxide tension
- PTE, pulmonary thromboendarterectomy
- PVR, pulmonary vascular resistance
- RVEF, right ventricular ejection fraction
- TLC, total lung capacity
- Tlco, carbon monoxide transfer factor
- VC, vital capacity
Statistics from Altmetric.com
- CO, cardiac output
- CTEPH, chronic thromboembolic pulmonary hypertension
- CVP, central venous pressure
- FEV1, forced expiratory volume in 1 second
- FVC, forced vital capacity
- mPAP, mean pulmonary artery pressure
- Pao2
- Paco2, arterial oxygen and carbon dioxide tension
- PTE, pulmonary thromboendarterectomy
- PVR, pulmonary vascular resistance
- RVEF, right ventricular ejection fraction
- TLC, total lung capacity
- Tlco, carbon monoxide transfer factor
- VC, vital capacity
Patients suffering from chronic thromboembolic pulmonary hypertension (CTEPH) present with progressive exertional dyspnoea and fatigue that respond poorly to medical treatment. CTEPH is the only type of pulmonary hypertension that can be successfully treated with conservative surgery—that is, pulmonary thromboendarterectomy (PTE)—in selected patients.1–3 To date, only about 2500 PTE operations have been performed worldwide.3
Follow up studies of PTE have shown sustained improvement in pulmonary haemodynamics.4–7 To our knowledge, the only study which has addressed the long term effects of PTE in a large sample of patients found that most had good functional status and a good quality of life with minimal use of health care services.8 However, because of the cross sectional design of their study, the authors stressed the need for a longitudinal prospective study to establish the functional and clinical benefit of this unique surgical procedure.
Moreover, there are few data on mid term cardiopulmonary function,9 particularly on exertion after PTE, and further investigation into lung abnormalities of CTEPH is needed to gain insight into some previous findings such as a time discrepancy between haemodynamic and gas exchange results10 and the persistently reduced carbon monoxide transfer factor (Tlco) after PTE.11
Since 1994 we have been following up all patients undergoing PTE. The short and mid term results of PTE in terms of survival, symptoms, cardiopulmonary function, and exercise tolerance are reported to evaluate the time course of improvement. We have also determined whether some clinical or haemodynamic variables can predict the mid term outcome.
METHODS
Study design
Our follow up protocol, which requires examinations 3 months after the operation and then yearly for 5 years, yielded complete detailed data for up to 2 years on 30 patients.
Population
Between May 1994 and October 1999 38 patients (19 men and 19 women) of mean (SD) age at operation of 50 (15) years with CTEPH were treated with PTE. Of the 38 patients, 16 had a positive history of venous thromboembolism, eight had a positive history of venous thromboembolism and antiphospholipid antibody syndrome, two had a positive history of venous thromboembolism, antiphospholipid antibody syndrome, and systemic lupus erythematosus, and three presented with only the antiphospholipid antibody syndrome. Despite detailed analyses, no cause for CTEPH was found in nine patients. Of the 38 patients, 32 had had an IVC filter laced; all the patients with venous thromboembolism had received this treatment.
Three patients died perioperatively and two others had persistent postoperative pulmonary hypertension and were transplanted during the first year after PTE. Thus, 33 patients (15 men and 18 women) of mean (SD) age 51 (15) years had follow up results at 1 year. Two patients died during the second year after PTE and three of the 33 were not followed up at 2 years because they lived too far from the hospital.
Operation
The selection criteria for surgery3,12–14 and the standardised protocol for the operation4 were those which have been previously published, except that we do not usually clamp the ascending aorta or use cardioplegia.5 In all but one of the cases the approach was bilateral.
Preoperative and postoperative measurements
Preoperatively and 3 months, 1 year, and 2 years after PTE the patients underwent the following tests.
Clinical examination
A clinical examination with determination of the NYHA class and the length of time (<24 or ≥24 months) in that class before surgery. Patients in NYHA classes I or II were considered less clinically impaired and those in NYHA classes III or IV as more impaired.
Right heart haemodynamic study
A right heart haemodynamic study (Explorer, Baxter International Inc, Irvine, CA, USA) was undertaken using published normal resting haemodynamic values. The haemodynamic parameters were dichotomised according to their normality range (mean ±2SD).
Lung function
Spirometric tests (Pulmonet III, Sensormedics, Anheim, CA, USA) were performed and Tlco (single breath method, Transferscreen II Jaeger, Wurzburg, Germany) was measured.15–17 A restrictive pattern was defined as a total lung capacity (TLC) of ≤80% predicted and a forced expiratory volume in 1 second (FEV1)/forced vital capacity (FVC) ratio of >88% predicted in men and 89% predicted in women. An obstructive pattern was defined as an FEV1/FVC ratio of ≤88% predicted in men and 89% predicted in women. Adjusted Tlco for haemoglobin concentration was defined as pathological when <80% predicted.
Arterial blood gas analysis
Radial arterial blood gas analyses (Ciba Corning Diagnostics Corp, Hedfield, MA, USA) were carried out. The measured arterial oxygen tension was standardised to an arterial carbon dioxide tension (Paco2) of 5.3 kPa (Pao2st).18 Patients were defined as hypoxaemic when Pao2st was <9.3 kPa10 and hypocapnic when Paco2 was <4.7 kPa.
Exercise testing
Treadmill exercise testing (modified Bruce protocol)19 was performed starting from step 0 (2.7 km/h, 3 min) to step 0.5 (2.7 km/h, 3 min, 5% incline) to step 1 (2.7 km/h, 3 min, 10% incline) and up to step 4 with a 2% increase in incline at each step and with an increased speed (stage 2: 4 km/h, 3 min; stage 3: 5.5 km/h, 3 min; stage 4: 6.8 km/h, 3 min). The test was interrupted at the onset of breathlessness or when the fall in percentage arterial oxyhaemoglobin saturation (ΔHbSao2) was >5% or when the heart rate reached 80% of the maximal predicted. Poor or good tolerance to exercise was defined as the ability to cover at least 458 metres or not; this threshold was the median distance covered at 1 year. HbSao2 and heart rate were measured using a pulse oximeter (Oxyshuttle, Sensormedics, Anheim, CA, USA). Fifteen patients before PTE and one at 3 months after PTE did not perform the Bruce protocol because of severe hypoxaemia at rest (Pao2 <8 kPa).
Statistical analysis
Changes in the haemodynamic and respiratory parameters with time were assessed by fitting a general linear model (with logit link for dichotomous variables). Huber-White robust standard errors were calculated to account for intrapatient correlation of measurements over time. The strength of association between mPAP and Pao2 was measured using the Pearson correlation coefficient. Mean changes at each time point and their 95% confidence intervals were calculated for all the haemodynamic and respiratory parameters measured. The median change in NYHA (and 95% confidence interval) was also computed at each time point. To verify the prognostic value of baseline mean pulmonary artery pressure (mPAP), NYHA class, and length of time in NYHA classes III or IV for normalisation of NYHA, Pao2 and exercise tolerance logistic models were fitted. The odds ratio (OR) and its 95% confidence interval were calculated. Bonferroni's correction for multiple outcomes was computed. A p value of <0.05 was considered statistically significant. All tests were two tailed (statistical software Stata 7, Statacorp, College Station, TX, USA).
RESULTS
Survival
In the immediate postoperative period two patients died of massive alveolar haemorrhage, presumably due to a peripheral pulmonary vessel injury caused by PTE; a third patient died three days after PTE of severe haemoptysis. These three deaths give an in-hospital mortality after PTE of about 10%. No other death occurred up to 1 year but two other patients died during the second year; one had a relapse after 12 months and the other, who had not shown any clinical improvement after surgery but refused lung transplantation, developed pneumonia 17 months after the operation. Thus, in the follow up period the death rate was 4 per 100 person-years.
Clinical examination
At the time of surgery 20 patients were in NYHA class III and 13 in class IV, having spent a median period of 13 months (range 6–48) in these classes. A significant improvement (p<0.0001) based on change in NYHA class was seen by 3 months (p<0.001) and no further significant changes were observed; 87%, 94%, and 93% of the patients were in classes I or II 3 months, 1 year, and 2 years, respectively, after PTE.
Haemodynamic indices
Table 1 shows the mean (SD) values of haemodynamic parameters before PTE and during follow up. Before PTE the patients had a high mPAP and PVR (pulmonary vascular resistance) and low cardiac output (CO) and right ventricular ejection fraction (RVEF). Three months after surgery a significant improvement was seen in all the haemodynamic variables which persisted more or less unchanged at 1 year and 2 years for all variables; only mPAP showed a further improvement over time (3 months v 1 year, p=0.06; 1 year v 2 years, p< 0.05). In particular, 3 months after PTE all the patients showed complete recovery of central venous pressure (CVP) and CO. At 3 months 97% of the patients had a normal RVEF, and at 1 year and 2 years 94% and 92% of the patients had ejection fractions in the normal range. At 3 months 36% of patients had a normal PVR, and at 1 year and 2 years 50% and 54% had normalised values. At 3 months 31% of the patients had a normal mPAP, and at 1 year and 2 years 45% and 56% of patients had pressure values in the normal range.
Mean (SD) haemodynamic indices before PTE and during the follow up period and the mean (95% confidence intervals) changes over time
Lung function indices
Mean lung volumes were in the normal range before PTE and during the follow up period (table 2). Before PTE, 24% of patients had a mild restrictive pattern which normalised by the end of the follow up period. One patient had persistent bronchial obstruction due to asthma.
Mean (SD) lung function indices (% predicted) before PTE and during the follow up period and the mean (95% confidence intervals) changes over time
Before PTE mean Tlco values were slightly reduced but the overall trend after PTE showed a significant improvement (table 2). The mean Tlco before PTE differed significantly from that at 1 year (p<0.05) and 2 years (p< 0.05) but not from that at 3 months. Tlco was in the normal range in 29%, 30%, 35%, and 42% of the patients, respectively, before PTE, and 3 months, 1 year, and 2 years after the operation.
Arterial blood gas analysis
Table 3 shows mean (SD) values of Pao2 and Paco2 before PTE and during the follow up period. Before surgery the mean Pao2 was moderately to severely reduced and Paco2 was slightly reduced. Pao2 showed a significant improvement which was achieved by 3 months without any further improvement. A significant correlation was found between mPAP and Pao2 measured at any time during the follow up period (r=0.75; p<0.0001). Paco2 showed a significant attenuation of the hyperventilation which, like the improvement in Pao2, was achieved by 3 months after the operation. Before PTE and 3 months, 1 year, and 2 years after surgery 10%, 59%, 52%, and 50%, respectively, of the patients had Pao2 values in the normal range whereas 21%, 45%, 48%, and 50%, respectively, had Paco2 values in the normal range.
Mean (SD) Pao2st and Paco2 values before PTE and during the follow up period and the mean (95% confidence intervals) changes over time
Exercise testing
Table 4 shows the mean (SD) total distance covered until exercise interruption resulting from dyspnoea, ΔHbso2 >5%, an increase in heart rate over 80% of the maximal predicted, or leg pain before PTE and during the follow up period. The overall trend showed a statistically significant improvement. At each time during the follow up period there was a significant change compared with the preoperative value. Table 5 shows the percentage of patients who interrupted the exercise test at each step of the Bruce protocol at different time points during the follow up period.
Mean (SD) total distance covered in metres until exercise interruption before PTE and during the follow up period and the mean (95% confidence intervals) changes over time
Percentage of patients interrupting exercise at each step of the Bruce protocol and at each time during the follow up period
Time course of normalisation after surgery
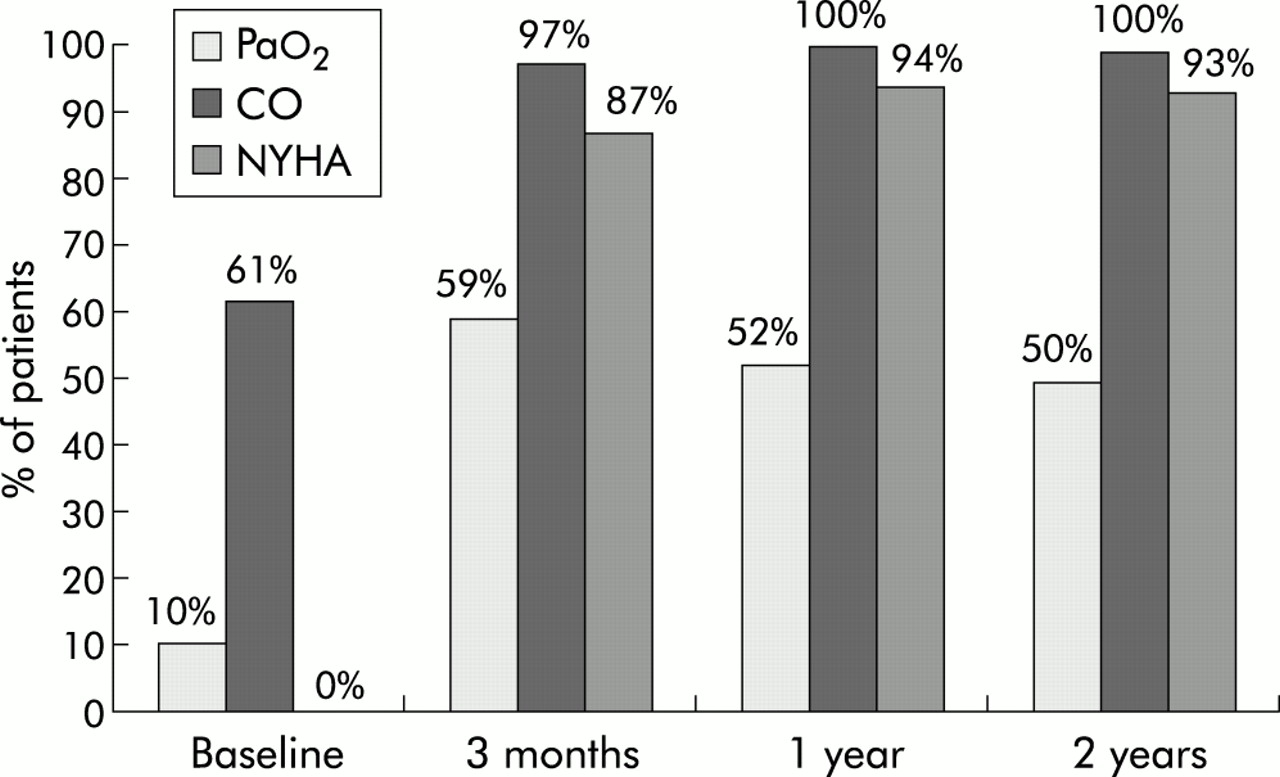
As shown in figs 1 and 2, before surgery all the patients had pulmonary hypertension and were more clinically impaired, almost all had hypoxaemia and poor exercise tolerance, while only 40% had a low cardiac output. The beneficial effects of PTE on cardiac output, gas exchange, and clinical status were nearly all gained during the first 3 months after PTE (fig 1); only patients with normal mPAP and good exercise tolerance progressively increased over time (fig 2).

Percentage of patients with normal standardised arterial oxygen tension (Pao2st) and cardiac output (CO) and with less clinical impairment (NYHA class I–II) before PTE and at each time point during the follow up period.

{kind=link}
{kind=link}
Percentage of patients with normal pulmonary arterial pressure (mPAP) and good tolerance to exercise before PTE and at each time point during the follow up period.
Clinicohaemodynamic characteristics before PTE and mid term outcome
Baseline mPAP, NYHA class, and time in NYHA classes III or IV were not significant predictors of normalisation either of NYHA or of Pao2 at 1 year. Only baseline NYHA class IV was associated with persistent impaired exercise tolerance at 1 year (OR 7.2, 95% CI 1.4 to 38.3; p=0.04 after Bonferroni's correction).
DISCUSSION
This follow up study shows that PTE is an effective surgical procedure for CTEPH, the success of which is proved by the low mortality rate, the prompt reduction in pulmonary hypertension, and the restoration of cardiac output in almost all patients, even those who were very compromised. PTE provides excellent symptomatic improvement. No further improvement was seen in haemodynamic parameters and gas exchange data beyond 3 months after surgery; only mPAP and exercise tolerance improved gradually and continued to improve during the second year of follow up. Tlco is overestimated before PTE but after PTE the trend was similar to that of mPAP. No clinical or haemodynamic parameter before PTE was able to predict the mid term outcome, except for NYHA class which predicted exercise tolerance.
The operative and perioperative mortality rate in our sample was close to an acceptable level (currently below 10%), which is similar to the rate reported from the University of California, San Diego Medical Center.6
The reported mid and long term mortality rates vary depending, at least in part, on the different periods in which the surgery was performed.11 In general the results have gradually improved with practice, except for those from the San Diego Medical Center4,20 which were good even at the beginning of the 1990s. Another factor which may account for different results is that follow up studies may extend for more than a few years during which pulmonary hypertension may recur in cases in whom the cause persists after an asymptomatic period.2 In our sample two patients relapsed into severe pulmonary hypertension, one of whom died 12 months after PTE. Both these patients had a history of venous thromboembolism associated with antiphospholipid antibody syndrome. Our relapse rate of 6% is similar to that reported from the San Diego Medical Center.21
In 1990 Kapitan et al22 reported the impression that postoperative improvement in right ventricular function and haemodynamics is prompt in most cases but that gas exchange improves more gradually over a period of weeks to months. They suggested that this could be because the relief of mechanical obstruction results in ventilation perfusion (VA/Q) abnormalities in vessels impaired by the effects of pulmonary hypertension which then remodel slowly, or because PTE injures operated vessels and adversely affects the postoperative perfusion distribution. A few years later Tanabe et al10 confirmed the time discrepancy between the improvement in pulmonary haemodynamics and gas exchange after PTE. Although the long term follow up in the study by Tanabe et al, the sample was small and the first postoperative examination was at 1 month. The difference in the time course between this and our follow up study could be explained by the fact that at 1 month the recovery in respiratory function may still be impaired by the direct effect of surgery, postoperative atelectasis, postoperative pulmonary oedema, diaphragm elevation, pleural adhesions, and general fatigue. All these factors may cause ventilation-perfusion abnormalities or diffusion limitations resulting in prolonged hypoxaemia. We found that at 3 months, when all these operative factors had been overcome, there was already substantial concordance between symptoms, cardiac results, pulmonary haemodynamics, and gas exchange. At 1 and 2 years only pulmonary pressure was further improved, probably due to a gradual recovery of damaged small vessels.
According to Kapitan et al23 one gas exchange parameter which did not improve postoperatively was Tlco. Before PTE 29% of the patients in our study had a normal Tlco; the bronchial circulation may be responsible for this. Because of the proliferation of anastomotic bronchial vessels, pulmonary capillaries distal to even completely obstructed pulmonary arteries will not be free of blood and will be available for carbon monoxide exchange.23,24 The relief of pulmonary obstruction ultimately leads to reperfusion of previously unperfused pulmonary parenchyma, but this change in perfusion will not increase Tlco. Because of the overestimation of Tlco by the single breath method before PTE, the improvement is not visible at 3 months but becomes significant at 1 and 2 years. This finding is in disagreement with that of Kapitan et al23 who did not find any improvement in Tlco at 1 year.
We also observed further improvement at 1 and 2 years in exercise tolerance. In addition to the gradual improvement in VA/Q, this was probably due to the change in overall clinical status which allowed progressive training.
Despite the undoubted efficacy of PTE, at the 2 year follow up about half of the patients still had mPAP >20 mm Hg, Tlco <80% predicted, Pao2 <9.3 kPa, and impaired exercise tolerance. Apart from those patients in whom the operation was not successful or who suffered relapse of pulmonary hypertension, the different mid term outcomes was dependent on the effects of pulmonary hypertension before surgery on vessels in the non-obstructed segments of the lungs, including medial and intimal hypertrophy and obliteration, and by the different recovery after PTE of the damaged small vessels. Unfortunately, none of the preoperative parameters measured before PTE was able to predict the mid term outcome, except NYHA class which predicted mid term exercise tolerance.25
The main finding of this study is that most of the improvement in clinical and functional parameters after PTE is achieved in the first 3 months due to the relief of central mechanical obstruction, while only minimal further changes occur later, probably as a result of further correction in VA/Q inequality. The excellent clinical results of this operation are long lasting in most patients, even the more compromised ones.
APPENDIX
Pavia Thromboendarterectomy Group M Viganò, A M D'Armini, B Cattadori, C Monterosso, G Koukoulis (Division of Cardiac Surgery, Director M Viganò), V Emmi (Intensive Care Unit, Director A Braschi), F Piovella, S Serafini, M Barone (Thromboembolism Unit, Director F Piovella), F Recusani, C Falcone, S Ghio, L Scelsi, C Raineri (Division of Cardiology, Director L Tavazzi), I Cerveri, M C Zoia, M Beccaria, A Corsico, P Fulgoni (Institute of Respiratory Disease, Director E Pozzi), R Passera (Radiodiagnostic Unit, Director A Villa), R Dore, G Meloni (Institute of Radiology, Director R Campani), E Arbustini, M Grasso (Institute of Pathology, Director U Magrini), P Vitulo and T Oggionni (Division of Pulmunology, Director A Rossi), IRCCS Policlinico San Matteo; C Aprile (Nuclear Medicine Unit, Director C Aprile), IRCCS Fondazione Maugeri Pavia; C Fracchia, G Callegari (Division of Pulmunology, Director C Fracchia), IRCCS Fondazione Maugeri Montescano.
Acknowledgments
The authors thank William R Auger for his scientific and editorial assistance.
REFERENCES
Footnotes
-
↵* Members of the Pavia Thromboendarterectomy Group are listed in the Appendix.