Article Text

Abstract
Background: The control of body weight and cardiac sympathetic function in patients with obstructive sleep apnoea-hypopnoea syndrome (OSAHS) are important because both factors have significant effects on the mortality of these patients. It has recently been reported that OSAHS has a significant effect on the secretion of leptin, a hormone involved in the control of body weight and sympathetic nerve activity. In addition to the circadian rhythm of leptin secretion, the effects of one night of treatment with nasal continuous positive airway pressure (nCPAP) and the mechanism of the effects of nCPAP on nocturnal leptin secretion in patients with OSAHS has not yet been elucidated.
Methods: Blood samples were obtained at 21.00 hours, 00.00 hours, 03.00 hours, and 06.30 hours from 21 subjects with OSAHS (mean apnoea and hypopnoea index 52.4/h), with and without nCPAP treatment. Iodine-123 (I123)-meta-iodobenzylguanidine (MIBG) imaging was used to evaluate myocardial sympathetic function before nCPAP treatment.
Results: Plasma leptin reached a peak level at 00:00 hours (p<0.01) in patients with OSAHS, both with and without nCPAP treatment. The first night of nCPAP treatment significantly decreased the plasma leptin levels at 03.00 hours (without nCPAP: mean (SE) 21.6 (4.7) ng/ml; with nCPAP: 19.3 (4.1) ng/ml, p<0.02) and at 06.30 hours (without nCPAP: 17.6 (3.8) ng/ml; with nCPAP: 15.2 (3.2) ng/ml, p<0.01). The magnitude of the decrease in leptin levels after nCPAP treatment was significantly correlated with cardiac sympathetic function measured before nCPAP treatment (p<0.03).
Conclusions: Patients with OSAHS undergo nocturnal increases in leptin levels in spite of interruption of sleep due to apnoea and hypopnoea, a trend seen in normal subjects. Plasma leptin levels in patients with OSAHS decreased significantly after the first night of nCPAP treatment. Enhanced cardiac sympathetic function in these patients may contribute to the leptin levels before nCPAP treatment and vice versa.
- leptin
- obstructive sleep apnoea-hypopnoea syndrome
- cardiac sympathetic function
Statistics from Altmetric.com
Control of body weight and cardiac sympathetic function are both clinically important in patients with obstructive sleep apnoea-hypopnoea syndrome (OSAHS) because they have significant effects on the morbidity and mortality of such patients. Leptin is a circulating hormone that is expressed abundantly throughout the body—specifically in adipose tissue,1–3 although it is also secreted from other tissues including human placenta and stomach.4,5 Leptin induces a complex response that affects control of body weight and energy expenditure.1 It has recently been reported that circulating plasma leptin levels are raised in men with newly diagnosed untreated OSAHS.6–8 Earlier studies of nasal continuous positive airway pressure (nCPAP) in the treatment of patients with OSAHS suggested that OSAHS has a significant impact on serum leptin levels, with significantly decreased levels following nCPAP treatment of 3–4 days, 1 month, and 6 months.6,9 However, these studies did not report the first night effects of nCPAP on serum leptin levels. Patients with OSAHS have significantly higher muscle sympathetic nerve activity (MSNA) than controls,10 but significantly decreased MSNA and blood pressure during sleep have been reported after the first night of nCPAP treatment.10 It is therefore possible that changes in serum leptin levels occur after only one night of nCPAP. In addition to the effects of one night of treatment with nCPAP, it is unknown whether a nocturnal increase in serum leptin levels (as occurs in both lean and obese subjects) also occurs in patients with OSAHS.11 We have therefore studied the nocturnal variation in plasma leptin levels and the first night effects of nCPAP treatment in patients with OSAHS.
It is also important to understand the mechanism which drives these changes in leptin levels because leptin has been reported to be associated with an increased risk of myocardial infarction, haemorrhagic stroke, and abnormal fibrinolysis in men and postmenopausal women.12–14 Although a relationship between leptin levels and MSNA in patients with OSAHS has not been found,8 MSNA levels do have a significant positive correlation with leptin concentrations in healthy non-diabetic men.15 We have therefore studied the relationship between the changes in plasma leptin levels and cardiac sympathetic nerve function.16
METHODS
Subjects
Twenty one men of mean (SE) age 45.0 (2.4) years and body mass index (BMI) 28.9 (0.8) kg/m2 with OSAHS (apnoea-hypopnoea index (AHI) 52.4 (3.4) episodes/h) underwent nCPAP treatment. Polysomnography was performed16,17 before nCPAP was started and again on the first night of nCPAP treatment. There was a 1 week interval between the two polysomnographic examinations. OSAHS was established on the basis of clinical and polysomnographic criteria.16,17 In addition to clinical symptoms, an AHI of >20 events/hour was used as a selection criterion because these patients were good candidates for nCPAP treatment. Six of the patients had hypertension (five of whom were prescribed antihypertensive drugs), four had diabetes (one of whom was prescribed a glucosidase inhibitor while the others received only diet therapy), and two patients had both hypertension and diabetes (one patient received an antihypertensive drug and an oral hypoglycaemic agent; the other was on antihypertensive drugs only). No patient was given subcutaneous insulin. These treatment regimens had been adhered to several months before nCPAP therapy was started. Control leptin samples were obtained at night (n=21) and in the morning (n=5) from the patients.
The study was approved by the Institutional Committee for the Protection of Human Subjects and all patients gave informed consent before the study.
Polysomnography
Polysomnography was started at 21.00 hours and ended at 06.30 hours. Surface electrodes were applied using standard techniques to obtain an electroencephalogram, an electromyogram of the chin, an electrocardiogram, and an electrooculogram. Sleep was defined according to the criteria of Rechtschaffen and Kales.18 Ventilation was monitored by inductive plethysmography (Respitrace; Ambulatory Monitoring, Ardsley, NY, USA). Airflow was monitored by thermistors (Nihon Kohden, Tokyo, Japan) placed at the nose and mouth, while arterial oxygen saturation (Sao2) was monitored continuously with a pulse oximeter (Pulsox-7; Minolta, Osaka, Japan). A polygraph (Polygraph System RM-6000; Nihon Kohden, Tokyo, Japan) was run continuously at 10 mm/s to record all of the above physiological data simultaneously throughout the course of the experiment. All parameters were stored in a data recorder (A-621; Sony Precision Technology, Tokyo, Japan) for subsequent analysis. Before blood sampling at 21.00 hours and 06.30 hours, blood pressure was measured three times and the mean value was calculated. The nCPAP pressure was titrated manually throughout one night. Apnoea was defined as the cessation of airflow at the nose and mouth lasting for more than 10 seconds. Hypopnoea was defined as a decrease of 50% or more in thoracoabdominal motion associated with a fall in the baseline oxygen saturation of 4% or more. All AHI values were calculated to express the number of episodes of apnoea and hypopnoea per hour of total sleep time.
Blood sampling and analysis
Patients ingested a light hospital meal in the evening. From 20.00 hours to 06.30 hours on the following day the patients did not eat or drink anything. Before polysomnography an 18-gauge catheter was inserted into the right antecubital vein. The catheter was connected to tubing, extended sufficiently so as not to disturb sleep, and locked by heparinised saline. Blood samples were withdrawn for analysing leptin, glucose, and immunoreactive insulin (IRI) at 21.00 hours, 00.00 hours, 03.00 hours, and 06.30 hours. In five of the 21 patients blood samples were taken at two separate times 06.30 hours before nCPAP treatment was initiated. Blood samples were immediately centrifuged at 4°C for 10 minutes and stored at –80°C for later analysis.
MIBG imaging
Iodine-123(123I)-meta-iodobenzylguanidine (MIBG) imaging has been used to evaluate myocardial sympathetic function in various cardiac diseases.19,20 The patients underwent 123I-MIBG cardiac imaging after polysomnography without nCPAP treatment. Each subject received 30 mg potassium iodine on the day before the study began, continuing until the day after the study ended in order to block tracer uptake by the thyroid gland. Using a gamma camera equipped with a low energy, parallel hole, general purpose collimator, planar images were obtained at rest in the anterior view over a 3 minute interval at 15 minutes (early image) and 3 hours (delayed image) after an injection of 111 MBq MIBG. The regions of interest within the heart were set manually on these planar images. The mean heart counts from the early image and from the delayed image were calculated. On the planar images a region in the upper mediastinum was used to calculate the mean mediastinal counts. The heart to mediastinum count ratios were calculated as an index of the myocardial uptake of MIBG. The heart to mediastinum count ratios from the early image (H/M early) and from the delayed image (H/M delay) were used as indices of cardiac sympathetic function.19,20
Assays
The plasma leptin level was measured by radioimmunoassay (RIA) with intra-assay and interassay coefficients of variation of 5.3% (n=10) and 5.9% (n=10), respectively.21 Serum levels of IRI were measured by RIA (Insulin-RIA-beads II, Dainabot, Tokyo, Japan) and plasma glucose was determined by an enzyme method (Glu-L 2; Wako Chemical, Osaka, Japan).
Data analysis
The data are presented as mean (SE) values. A non-parametric method was used for data analysis. Changes in plasma leptin levels during sleep were compared using the Friedman test. If a significant difference was found, differences between the peak values and the immediate values (before and after peak values) were compared by the Wilcoxon signed rank test, as were paired data of plasma leptin, glucose, and serum IRI concentrations at each sampling time before and after nCPAP treatment. The plasma leptin levels measured at two separate times in five of the subjects at 06.30 hours were also compared using the Wilcoxon signed rank test. Spearman rank correlation coefficients were calculated to analyse the correlation between variables. These calculations were performed using StatView software for Windows (Version 4.5; Abacus Concepts, Berkeley, CA). A p value of <0.05 was considered significant.
RESULTS
Anthropometric data, arterial blood gas tensions, and spirometric data are presented in table 1. The effects of nCPAP treatment on OSAHS are shown in table 2; sleep apnoea, nocturnal oxygen saturation, blood pressure, and sleep architecture all showed improvements.
Characteristics of study patients
Effects of nCPAP on obstructive sleep apnoea syndrome
Nocturnal profile of plasma leptin levels
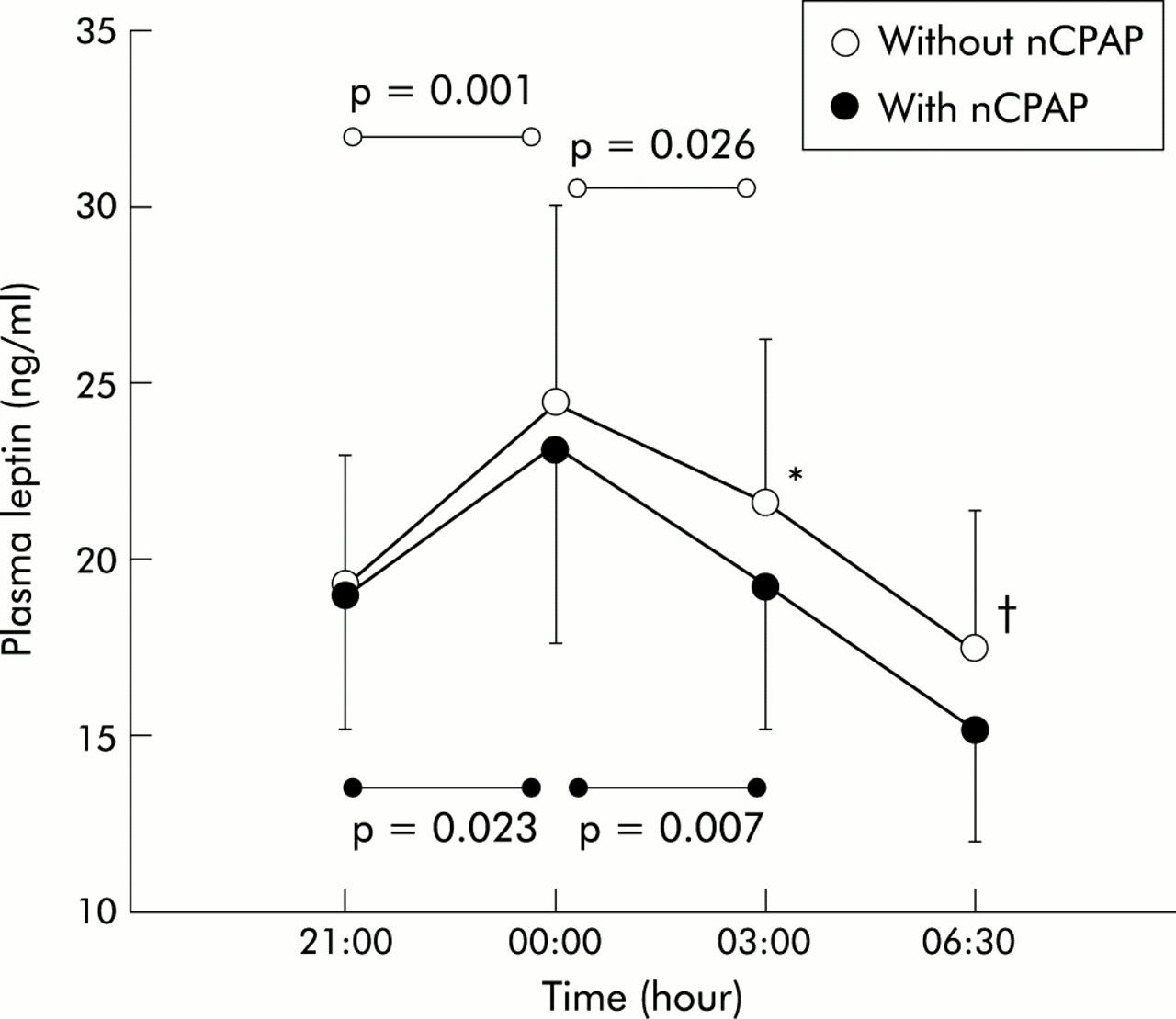
On each night the control leptin levels at 21.00 hours (before sleep) were the same (before nCPAP, 24.5 (5.6) ng/ml; just before an application of nCPAP, 23.2 (5.6) ng/ml, p=0.39). Plasma leptin levels measured at 06.30 hours before nCPAP treatment at two separate times in five patients were not significantly different from one another (first sample: 12.0 (3.6) ng/ml; second sample: 12.0 (4.1) ng/ml, p=0.85). The nocturnal profile of plasma leptin levels at 21.00 hours, 00.00 hours, 03.00 hours, and 06.30 hours in patients with OSAHS with and without nCPAP treatment are shown in fig 1. The trend towards a nocturnal increase was seen both with and without nCPAP treatment. On both nights plasma leptin levels peaked at 00.00 hours (p<0.05). On the first night of nCPAP treatment plasma leptin levels decreased significantly at 03.00 hours (without nCPAP, 21.6 (4.7) ng/ml; with nCPAP, 19.3 (4.1) ng/ml, p=0.016) and at 06.30 hours (without nCPAP, 17.6 (3.8) ng/ml; with nCPAP, 15.2 (3.2) ng/ml, p=0.009). The magnitude of changes in leptin levels with and without nCPAP treatment did not correlate significantly with the magnitude of changes in any parameters during polysomnography including AHI and blood pressure (table 2).

Nocturnal profiles of plasma leptin levels. Plasma leptin levels at 03.00 hours (*p<0.02) and 06.30 hours (†p<0.01) decreased significantly with nCPAP treatment. A peak level was seen at 00.00 hours which decreased significantly on both nights of the study. Plasma leptin levels at 00.00 hours with and without nCPAP treatment were significantly higher than the immediate values at 21.00 hours and 03.00 hours. Statistical analysis was performed by the Friedman test and Wilcoxon signed rank test and intragroup analysis was performed using the Wilcoxon signed rank test.
MIBG scintigram
H/M early and H/M delay did not correlate significantly with serum leptin levels at any point before or after nCPAP treatment. The results of MIBG scintigraphy before nCPAP treatment and the magnitude of the difference in plasma leptin levels before and after nCPAP treatment (Δleptin) showed a correlation only at 06.30 hours (H/M early: r = −0.50, p=0.027; H/M delay: r = −0.55, p=0.014; fig 2).

Correlation between (A) early heart to mediastinal count ratios, an index of myocardial uptake of MIBG (H/M early), and the magnitude of changes in plasma leptin levels (Δleptin) at 06.30 hours before and after nCPAP treatment (r = –0.50, p=0.027); and (B) correlation between delayed heart to mediastinal count ratios (H/M delay) and Δleptin at 06.30 hours before and after nCPAP treatment (r = –0.55, p=0.014).
Nocturnal profile of glucose and insulin levels
Nocturnal plasma glucose and serum IRI levels were measured in 19 of the 21 patients (fig 3). At 21.00 hours, about 3 hours after the evening hospital meal, plasma glucose and serum IRI showed no significant differences with or without nCPAP treatment, but a significant difference was seen in the plasma glucose level at 06.30 hours between those treated with nCPAP and those not treated (p<0.05, Wilcoxon signed rank test).

{kind=link}
{kind=link}
{kind=link}
Nocturnal profiles of (A) serum immunoreactive insulin levels and (B) plasma glucose levels. No significant difference was seen in serum immunoreactive insulin levels with and without nCPAP treatment at each sampling time; plasma glucose levels were significantly decreased with nCPAP treatment at 06.30 hours (*p=0.027).
DISCUSSION
We have shown that the nocturnal rise in the plasma leptin concentration is seen in patients with OSAHS whether or not they receive nCPAP treatment. After the first night of treatment with nCPAP the plasma leptin concentration decreased significantly at 03.00 hours and at 06.30 hours, although the control levels at 21.00 hours (before sleep) were the same. We have also shown that H/M early and H/M delay (indices of myocardial MIBG uptake showing cardiac sympathetic function and integrity of the heart) were significantly correlated with the magnitude of the decrease in the plasma leptin level at 06.30 hours compared with the level before nCPAP treatment—that is, plasma leptin levels in OSAHS patients who had exacerbated cardiac sympathetic function before nCPAP treatment decreased in proportion to the magnitude of their exacerbated cardiac sympathetic function activity before starting nCPAP treatment.
We have previously reported that plasma leptin levels decreased in the morning after treatment with nCPAP for 3–4 days, 1 month, and 6 months.9 It has recently been reported that serum leptin levels are significantly increased in patients with OSAHS compared with age and weight matched controls,6–8 and these levels were found to decrease significantly after 6 months of treatment with nCPAP.6,9 However, the precise timing of the fall in leptin levels after the introduction of nCPAP treatment has remained uncertain. In this study we have shown that plasma leptin levels begin to decrease during the first night of treatment with nCPAP. Although the AHI on the first night of treatment was small (table 2), it is possible that plasma leptin levels might decrease significantly with nCPAP treatment before 03.00 hours if nCPAP titration was more perfect because the data during the first night of treatment—especially in the early part of the polysomnographic study—are often imperfect.
The nocturnal increase in plasma leptin levels was seen in patients with OSAHS both with and without nCPAP treatment—a trend seen in both lean and obese subjects.11 It has been reported that there is a correlation between the diurnal rhythm of leptin and meal times.22 However, the meal times of the patients before and after nCPAP were the same in our study, so our patients showed nocturnal increases in plasma leptin levels despite sleep fragmentation due to AHI, although the leptin levels at 03.00 hours and 06.30 hours decreased significantly after one day of nCPAP treatment.
From the results of the cardiac MIBG scintigram and plasma leptin levels before and after nCPAP treatment, the decrease in plasma leptin levels seen after one day of treatment might be explained by the effect of nCPAP on sympathetic nerve activation. This, together with the effects on blood pressure found in this study, is consistent with another report suggesting that nCPAP decreases MSNA and blood pressure during sleep.10 Previous reports have also shown that increased cardiac sympathetic function is improved after one month of nCPAP treatment.16 In addition, Snitker et al15 reported that MSNA levels had a significant positive correlation with leptin concentrations in healthy non-diabetic men. The decrease in sympathetic nerve activity due to nCPAP treatment might therefore also reduce serum leptin levels. On the other hand, several reports have shown that leptin administration increases sympathetic nerve activity,23,24 and it has recently been reported that leptin may play a role in the pathogenesis of some forms of obesity related hypertension.25 Decreased leptin levels in patients with OSAHS following treatment with nCPAP might therefore improve sympathetic nerve activity including blood pressure (table 2). Further studies are needed to determine whether the decrease in serum leptin levels improves the sympathetic nerve activity or whether improved sympathetic nerve activity causes serum leptin levels to decrease. Although nCPAP treatment significantly improves AHI, REM time %, and the severity of hypoxaemia, as indicated by the percentage of time with Sao2 <85% or 90% and blood pressure (table 2), these measurements were not correlated with the decrease in the serum leptin levels. Further research is therefore also required to determine the factors that significantly impact on serum leptin levels.
The plasma glucose level was found to be reduced at 06.30 hours after one night of nCPAP treatment, but IRI levels did not change. From these results we speculate that insulin activity for glucose also improved after the first night of nCPAP treatment. It has been reported that exogenously administered leptin improves insulin activity26,27; in our study the insulin activity for glucose improved in spite of decreased leptin levels. Phillips et al8 recently reported that OSAHS may be accompanied by further resistance to the metabolic effects of leptin, greater than the resistance evident in obesity alone. Further improvements in leptin resistance to the metabolism of insulin and glucose after nCPAP treatment might therefore enhance the action of insulin on glucose more than the decrease in leptin levels.
The primary limitation of our study was that blood samples were obtained only four times while the serum leptin level cycles every 7 minutes.28 However, the nocturnal profile of the leptin levels before and after nCPAP treatment was the same as in previously reported studies,11,28 although the levels at 03.00 hours and 06.30 hours decreased significantly after nCPAP treatment. The serum leptin levels therefore appear to be accurate despite the longer sampling intervals.
A second limitation of this study is that there was no statistically significant correlation between MIBG uptake before treatment and any of the eight measurements of plasma leptin before and after nCPAP treatment, and Δleptin was significantly correlated with the early and delayed MIBG uptake at 06.30 hours only. Confidence in the significance of Δleptin at 06.30 hours may therefore be reduced by the amount of statistical testing performed, and the relationship between leptin levels and cardiac sympathetic function should be studied further, including long term effects of nCPAP treatment on leptin levels and MIBG scintigraphy.
Ideally, we would have liked to have done complementary studies of leptin and glucose measurements in weight matched subjects without OSAHS during a single night of sham nCPAP. However, it is difficult to find weight matched subjects without OSAHS in Japan because East Asian subjects are more likely to develop OSAHS at a lower BMI than Western subjects.29 The control leptin levels corresponding to the two measurements at 21.00 hours and the two measurements at 6.30 hours were the same before nCPAP treatment, but following nCPAP treatment the serum leptin levels decreased significantly at 03.00 hours and 06.30 hours. Treatment with nCPAP for one night therefore significantly lowered the leptin levels, although no weight matched control subjects were studied.
A further limitation of this study is that no women were included. It has been reported that the circulating concentration of leptin is significantly higher in both premenopausal and postmenopausal women than in men, even when the levels were corrected for differences in BMI or percentage body fat (premenopausal women > postmenopausal women > men).30 The changes in leptin levels with and without nCPAP treatment would therefore have been different if women had been included in the study. Although the overall results would have been similar, further studies are needed to apply the results of this study to women.
This study has shown that decreased serum leptin levels in the morning may be a marker of improved cardiac sympathetic nerve function. This finding has clinical relevance in light of the negative associations of increased leptin levels—namely, an increased risk of myocardial infarction,12 haemorrhagic stroke,13 and abnormal fibrinolysis in men and postmenopausal women.14 It has also been reported that hypercoagulable states are improved by nCPAP treatment.17 Although leptin levels change according to body weight1,2 and with meal times,22 continuous measurement of leptin levels before and after the initiation of nCPAP treatment, in addition to the measurement of body weight, may prove helpful in evaluating the prognostic factors and efficacy of treatment in patients with OSAHS.
Acknowledgments
The authors thank T Ueda for manuscript preparation. This work was supported in part by grants from Tahei Ueda Memorial Fund; the Japanese Ministry of Education, Science, Sports, and Culture (grant No.13670598); and the Japanese Ministry of Health and Welfare.