Article Text

Abstract
Background: Caffeine is known to inhibit phosphodiesterases, to mobilise intracellular calcium, and to act as an antagonist at adenosine receptors, all of which can potentially alter nitric oxide (NO) production. It was therefore hypothesised that caffeine may alter exhaled NO (eNO) levels.
Methods: In a randomised, single blind, crossover manner, 12 normal subjects consumed either (1) coffee and a placebo capsule, (2) decaffeinated coffee and a capsule of 200 mg caffeine, or (3) decaffeinated coffee and a placebo capsule. Serum caffeine levels were measured at baseline and 1 hour later. Exhaled NO levels were also measured at baseline and each hour for 4 hours.
Results: A significant percentage fall in mean (SE) eNO from baseline was seen 1 hour after either caffeinated coffee or a caffeine capsule when compared with placebo (13.5 (4.0)%, p=0.009 and 19.0 (3.8)%, p=0.001, respectively).
Conclusion: Caffeine causes a significant decrease in eNO which will need to be considered when designing trials to measure eNO levels. The mechanism may be via adenosine receptor antagonism or by altering levels of cGMP.
- caffeine
- exhaled nitric oxide
Statistics from Altmetric.com
Nitric oxide (NO) is generated from l-arginine by constitutive NO synthases (ecNOS and nNOS) and inducible NO synthase (iNOS). It has become apparent that a number of exogenous factors affect levels of exhaled NO. Cigarette smoking and alcohol decrease exhaled NO levels via effects upon constitutive and iNOS, respectively, while asthmatic inflammation and upper respiratory tract infections increase exhaled NO (eNO) via iNOS induction.1–3
Caffeine is widely consumed as coffee, tea, and cola. Coffee also contains numerous other substances such as minerals, lipids, proteins, carbohydrates, aliphatic acids, glycosides, and contaminants formed during the roasting process including nitrosamines, heterocyclic amines, and paraffins.4 In high doses caffeine inhibits phosphodiesterases, leading to elevation of cyclic AMP (cAMP) and cyclic GMP (cGMP) which may be the mechanism for its weak bronchodilatory effect in mild asthmatic subjects. It can also mobilise intracellular calcium stores and, at lower concentrations, caffeine antagonises adenosine receptors (A1, A2a).4 In addition, an increase in intracellular cGMP upregulates ecNOS expression and an increase in intracellular cAMP downregulates it.5,6 Stimulation of adenosine receptors leads to differential effects, with A2a receptor stimulation increasing NO generation while A1 receptor stimulation leads to decreased NO production by endothelial cells.7 This led us to test the hypothesis that caffeine may have an effect on eNO levels in normal subjects.
METHODS
Study sample and protocol
Twelve normal healthy habitual caffeine drinkers (four men) of mean age of 33.2 (9.3) years were recruited to the study. All were non-smoking non-asthmatic subjects with normal spirometric parameters and no recent history of respiratory tract infections. Subjects abstained from dietary methylxanthines for at least 8 hours before the study. The study was approved by the institutional ethics committee and all subjects gave written informed consent.
There were three arms to the study, which were randomised in a single blind, placebo controlled, crossover manner and comprised: (1) coffee 2.4 g with an approximate caffeine content of 100 mg per 200 ml cup (Espresso filtered coffee, Harris Ltd, Sydney) and a matched placebo capsule (Glucodin (glucose), Boots Healthcare, Australia); (2) decaffeinated coffee (<3 mg caffeine per 200 ml cup, Moccona, Douwe Egberts Joure, Holland) and a capsule of 200 mg caffeine (No Doz, Key Pharmaceuticals, Sydney); or (3) decaffeinated coffee and a placebo capsule. Subjects consumed a further aliquot of the same beverage after the first hour.
At baseline, eNO and serum caffeine levels were measured. Exhaled NO was then measured every hour for 4 hours. Serum caffeine samples were taken 1 hour after caffeine intake to sample peak serum levels of caffeine.
Measurement of exhaled NO
Exhaled NO was measured by chemiluminescence (Model 2107, Dasibi Environmental Corporation, Glendale, CA, USA) with subjects exhaling slowly at a flow rate of 5 l/min from total lung capacity over 30–40 s with constant raised oral pressure avoiding nasal contamination, following ERS recommendations.8 The mean of three successive peak plateau readings was used for analysis. Ambient NO levels were recorded and, if >40 ppb, the analyser was flushed with NO-free gas.
Measurement of serum caffeine levels
Serum caffeine concentrations taken at baseline and 1 hour were analysed by gas chromatography-mass spectroscopy.
Spirometric testing
Spirometric tests were performed using a dry wedge spirometer (Vitalograph, UK) to ensure that all subjects had a normal forced expiratory volume in 1 second (FEV1).
Statistical analysis
Exhaled NO values were log transformed to the normal distribution and analysed by two way repeated measures ANOVA to compare the differences between the three treatment groups over time. Exhaled NO levels were expressed as mean (SE) parts per billion (ppb) and changes in exhaled NO displayed as mean (SE) % change from baseline. Serum caffeine levels were reported as mean (SE) mg/l and analysed by paired t test. Significance was taken as p<0.05, with post hoc Bonferroni corrected paired t test applied to significant ANOVA results.
RESULTS
Subjects
Eleven of the 12 subjects completed the study; one subject was withdrawn because of a respiratory tract infection.
Exhaled NO
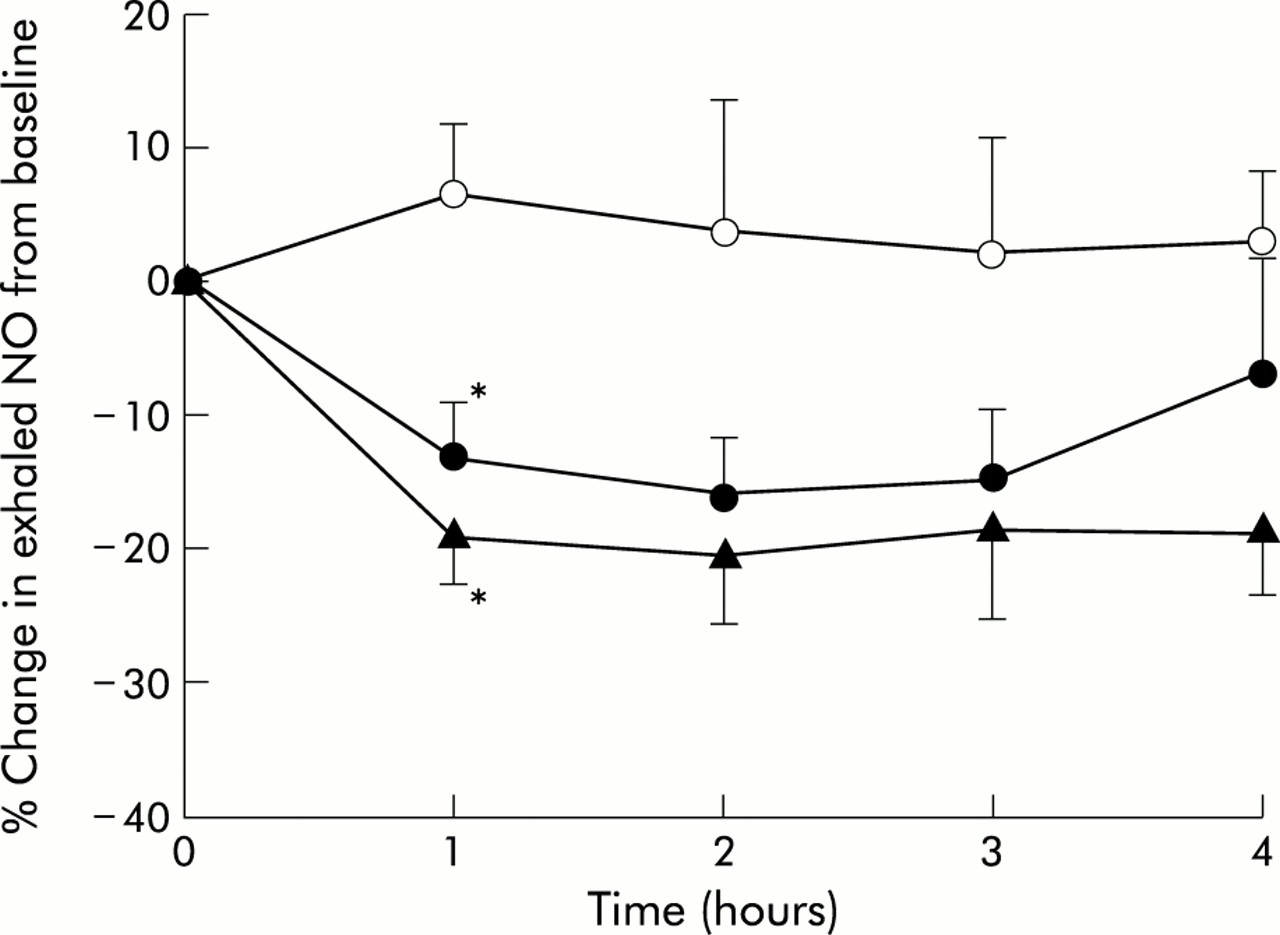
Baseline eNO results were not significantly different between the study days in any of the three phases. After coffee or caffeine consumption there was a significant decrease in eNO levels compared with placebo (p=0.008, two way ANOVA). Mean eNO levels decreased significantly in the first hour after coffee or caffeine consumption compared with the placebo phase and caused a mean percentage fall of 13.5 (4.0)% and 19.0 (3.8)% (p=0.009 and p=0.001 respectively, post hoc t tests, fig 1). Mean eNO levels during the coffee and caffeine phase remained consistently lower than baseline levels during the following 3 hours, although the difference was not statistically significant.

{kind=link}
Percentage change in exhaled NO compared with the baseline value (0) at 1, 2, 3, and 4 hours after administration of decaffeinated coffee and placebo (open circles, mean (SE) baseline value 9.9 (2.4) ppb), coffee and placebo (closed circles, mean (SE) baseline value 11.6 (2.3) ppb), or decaffeinated coffee and 200 mg caffeine (triangles, mean (SE) baseline value 12.3 (2.6) ppb) in 11 normal subjects. *p<0.05.
Serum caffeine levels
Baseline serum caffeine levels did not differ significantly between study days. The mean (SE) serum caffeine level changed after 1 hour during the three phases: (1) caffeinated coffee and placebo from 0.6 (1.3) mg/l to 2.8 (0.8) mg/l, p=0.002; (2) decaffeinated coffee and caffeine from 0.6 (1.2) mg/l to 3.7 (0.9) mg/l, p=0.003; (3) decaffeinated coffee and placebo from 0.5 (1.3) mg/l to 0.4 (0.3) mg/l, p=0.21. No relationship was found between serum caffeine levels and change in eNO.
DISCUSSION
This study shows that caffeine significantly decreases eNO levels, either as 200 mg caffeine or as coffee with an average caffeine content of 100 mg. There are many other additional components of coffee, but none have a known mechanism which would cause NO to fall. The mechanism for this reduction in eNO is not certain, but it is known that at doses similar to those used in our study caffeine antagonises adenosine receptors. At higher concentrations caffeine causes inhibition of the breakdown of cAMP and cGMP, but it may also inhibit guanylate cyclase.5,6,9
Adenosine enhances NO production from endothelial cells through adenosine A2a receptors, while adenosine A1 receptors decrease it.7 Thus, caffeine could antagonise A2a receptors if these are active in airway epithelium, reducing the generation of NO.7 If caffeine acts by adenosine receptor antagonism, then A1 receptors are less likely to be involved. Direct airway AMP challenge has also been associated with a fall in eNO, but this was interpreted as being related to airway bronchoconstriction.10
An alternative mechanism by which caffeine could alter NO generation is through the inhibition of the phosphodiesterases and hence the breakdown of the secondary messengers cGMP and cAMP. However, theophylline inhibits soluble guanylate cyclase thus reducing the formation of cGMP, so the effects of caffeine on cGMP may be mixed.5,9 Cyclic GMP upregulates ecNOS generation while cAMP may downregulate it,5,6 but these effects are at the level of protein translation which would not be expected to be seen for some hours. It would appear therefore that the immediate effect of caffeine observed in this study is more compatible with a reduction in cGMP via inhibition of soluble guanylate cyclase.9
Spirometric tests were not performed so as not to alter the levels of eNO spuriously, as some reports have suggested a fall in eNO after repeated spirometry alone.11 Silkoff et al measured exhaled NO both after repeated spirometric testing and β2 adrenergic agonist inhalation in asthmatic and normal subjects and found that spirometric testing decreased eNO levels while the β2 agonist increased them.11 Others have reported that eNO levels are reduced shortly after bronchoconstriction to direct and indirect stimuli in subjects with asthma, and suggested that eNO levels can be modulated by bronchial tone.10 The first measurement after intervention was at the end of the first hour, which was at the time when previous studies have indicated that eNO is no longer significantly different from baseline. In addition, the control phase of the experimental design indicates that the effects on eNO are due to caffeine and not to repeated spirometric tests (fig 1).
Decaffeinated coffee had no effect on eNO levels, suggesting that caffeine is the principal agent causing the decrease in eNO. Caffeine is associated with a brief reduction in eNO levels over 4 hours in normal subjects, which suggests that it should be withheld for at least this time period before taking measurements in normal and probably in asthmatic subjects; however, this latter group was not assessed in this study.
Acknowledgments
The authors thank the participants for donating their time. The study was funded in part by NHMRC, Australia.