Article Text

Abstract
Background: There are few data in asthma relating airway physiology, inflammation and remodelling and the relative effects of inhaled corticosteroid (ICS) treatment on these parameters. A study of the relationships between spirometric indices, airway inflammation, airway remodelling, and bronchial hyperreactivity (BHR) before and after treatment with high dose inhaled fluticasone propionate (FP 750 μg bd) was performed in a group of patients with relatively mild but symptomatic asthma.
Methods: A double blind, randomised, placebo controlled, parallel group study of inhaled FP was performed in 35 asthmatic patients. Bronchoalveolar lavage (BAL) and airway biopsy studies were carried out at baseline and after 3 and 12 months of treatment. Twenty two normal healthy non-asthmatic subjects acted as controls.
Results: BAL fluid eosinophils, mast cells, and epithelial cells were significantly higher in asthmatic patients than in controls at baseline (p<0.01). Subepithelial reticular basement membrane (rbm) thickness was variable, but overall was increased in asthmatic patients compared with controls (p<0.01). Multiple regression analysis explained 40% of the variability in BHR, 21% related to rbm thickness, 11% to BAL epithelial cells, and 8% to BAL eosinophils. The longitudinal data corroborated the cross sectional model. Forced expiratory volume in 1 second improved after 3 months of treatment with FP with no further improvement at 12 months. PD20 improved throughout the study. BAL inflammatory cells decreased following 3 months of treatment with no further improvement at 12 months (p<0.05 v placebo). Rbm thickness decreased in the FP group, but only after 12 months of treatment (mean change –1.9, 95% CI –3 to –0.7 μm; p<0.01 v baseline, p<0.05 v placebo). A third of the improvement in BHR with FP was associated with early changes in inflammation, but the more progressive and larger improvement was associated with the later improvement in airway remodelling.
Conclusion: Physiology, airway inflammation and remodelling in asthma are interrelated and improve with ICS. Changes are not temporally concordant, with prolonged treatment necessary for maximal benefit in remodelling and PD20. Determining the appropriate dose of inhaled steroids only by reference to symptoms and lung function, as specified in current international guidelines, and even against indices of inflammation may be over simplistic. The results of this study support the need for early and long term intervention with ICS, even in patients with relatively mild asthma.
- asthma
- inhaled corticosteroids
- airway inflammation
- airway remodelling
- fluticasone
Statistics from Altmetric.com
Asthma is now accepted as a disease characterised by airway inflammation and bronchial hyperreactivity (BHR).1 There is also accumulating evidence that airway structural changes, or “remodelling” occur, probably secondary to the inflammatory process,1 although this is not a universally reproducible finding.2 Airway remodelling has in turn been linked to the development of physiological dysfunction, providing a possible mechanism for the development of fixed airflow limitation observed in many asthmatic patients.3 However, the relationship between these manifestations of asthma and the impacts of treatment upon them are poorly understood.
In recognition of the growing problem of asthma, international consensus guidelines for treatment in Europe, North America and Asia have emerged.4,5 These advocate treatment with inhaled corticosteroids (ICS), with adjustment of initial treatment to the minimal level consistent with an alleviation of symptoms and optimisation of spirometric parameters.6 However, there are also limited data indicating that BHR may be a useful and practicable clinical index which, in conjunction with optimising symptoms and lung function, resulted in more effective control of asthma.7 There are also advocates for the monitoring of airway inflammation, especially with the advent of non-invasive induced sputum and exhaled breath gas parameters designed to make this feasible for individual patient monitoring.1,8 In contrast, assessment of airway remodelling in airway biopsy specimens is technically difficult,1,9 the available literature scarce and variable,10 and the necessity of obtaining tissue bronchoscopically means that direct assessments of airway remodelling are unlikely to have a place in clinical management in the foreseeable future.
Despite the importance of ICS in current best practice asthma treatment, long term longitudinal data on their effects on physiology and BHR are scarce,11 and on airway inflammation and remodelling even more limited.10,12 In particular, there is an absence of information relating temporal changes in spirometric indices, BHR, airway inflammation and remodelling and the relationship of one to the other over time with treatment. Given the hypothesis that airway remodelling is important in the development of fixed airflow obstruction and long term pathophysiology, these types of studies might help to identify practicable objective outcome measures that could act as surrogates for changes in airway remodelling following ICS treatment.
We have carried out a study to dissect the relationships between spirometry, airway inflammation, and airway remodelling with BHR. Cross sectionally, we constructed a statistical model that related these elements of the asthmatic phenotype, and then validated this in a longitudinal intervention with high dose inhaled fluticasone propionate (FP). We tested the hypothesis that treatment with ICS would improve physiological indices, airway inflammation, and also airway remodelling, but that these changes would not be temporally concordant and that this would further characterise the interrelationships. This is the first longitudinal study that we are aware of that has related long term parallel changes in spirometry, airway inflammation, and remodelling with BHR at multiple time points. As this was a proof of concept study, we chose a high dose of ICS (750 μg FP bd) as an intervention in a deliberate attempt to maximise changes with treatment over 12 months.
METHODS
The study was approved by the Alfred Hospital ethics committee and all subjects gave written informed consent.
Patient selection
Thirty five mild to moderate yet symptomatic atopic asthmatic patients (24 men) were recruited. All fulfilled ATS criteria for asthma as previously described.13 Their mean (SD) age was 39 (13) years (range 20–70). None were current smokers, 16 were ex-smokers having given up a median of 16 years (interquartile range 6–22 years) prior to recruitment. There was no evidence of smoking related disease in any participant in the study. All subjects had diagnosed asthma for at least 12 months. Subjects were using only inhaled salbutamol for relief of symptoms and no “preventer” medication. No subjects had received treatment with regular ICS or inhaled long acting β2 agonists for at least 3 months before the study; 34 subjects had not received oral corticosteroid treatment for at least 12 months before the study, one had received a course of oral corticosteroid treatment 3 months before the study.
Twenty two normal healthy volunteers (11 men) were also recruited and underwent one bronchoscopic examination and physiological evaluation. None of the normal individuals had any history of respiratory illness; six were atopic. Their mean (SD) age was 38 (13) years (range 19–61). All were non-smokers, six were ex-smokers having given up a median of 13 years (interquartile range 10–18 years) before recruitment with no evidence of smoking related disease.
Study design
Following inclusion in the study there was a 2 week run in period in which the asthmatic subjects were continued on salbutamol alone. Following this baseline spirometric measurement, flow-volume loops and methacholine challenge tests were performed followed by bronchoscopic examination with airway biopsy specimens and bronchoalveolar lavage (BAL). The asthmatic patients were then randomised using computer generated numbers in balanced blocks into a double blind, placebo controlled, parallel group study with the addition of either 750 μg FP bd, given via a metered dose inhaler, or a physically identical placebo. Physiological assessments were repeated following 3, 6, and 12 months of treatment and bronchoscopic examination with airway biopsy and BAL was repeated at 3 and 12 months. Treatment was then discontinued and physiological assessments were repeated 1 month later.
All asthmatic and normal pathological end points were read blind to any clinical information, and all at the end of the study. The study was only uncoded after the blinded data was put on to a `checked and locked' database, administered remotely to the pathology laboratory by one of the authors (RB).
Patient assessments
Skin tests
Atopic status was assessed by skin prick testing to a panel of seven common aeroallergens and was defined by a response of ≥3 mm to one or more.
Spirometric tests and methacholine challenge
Forced expiratory volume in 1 second (FEV1) and BHR to methacholine were measured within 1 week before commencing study medication and again after 3, 6, and 12 months of regular treatment with study medication after a bronchodilator free period of at least 8 hours. A rolling seal spirometer (2130 SensorMedics Corporation, CA, USA) was used for measurement of FEV1 and flow-volume manoeuvres according to ATS criteria. BHR to methacholine was assessed by a previously described dosimeter technique and expressed as the cumulative dose required to provoke a 20% decrease in FEV1 (PD20) using linear interpolation from a dose-response plot.14
Bronchoscopic examination and airway biopsies
Subjects were premedicated with intravenous 0.4 mg atropine and 5–15 mg midazolam. Nebulised salbutamol (5 mg) was also given 15–30 minutes before bronchoscopic examination in both the asthmatic and normal subjects. 4% lignocaine was applied topically to the nose, pharynx, and larynx and 2% lignocaine below the cords in 2 ml aliquots as required up to a maximum dose of 6 ml. Subjects were monitored using pulse oximetry and administered oxygen during the procedure.
Bronchoalveolar lavage of the right middle lobe was performed with 3 × 60 ml aliquots of phosphate buffered saline and aspirated after minimal dwell time. Six endobronchial biopsy (EBB) specimens were taken from around the segmental subcarinae of the right lower lobe of each patient using alligator forceps (Olympus FB15C). Following macroscopic assessment for quality, these were placed in ice cold acetone-containing protease inhibitors (2 mM phenyl methyl sulphonyl fluoride with 20 mM iodoacetamide). BAL fluid and EBB specimens were immediately taken to the laboratory for further processing.
Processing of BAL fluid
Unprocessed BAL fluid was maintained at 4°C and the volume measured. Total, differential, and mast cell counts were performed on the unfiltered BAL fluid as previously described.15
Processing of biopsy specimens
Biopsy specimens were embedded into the hydrophilic polymer glycol methacrylate. This embedding method is designed to yield an optimal compromise between morphological and antigenic preservation. Coded blocks were cut on a semi-thin resin microtome (Leica RM 2310, Nussloch, Germany) using glass triangular knives. The 2 μm sections were then floated on water and adhered to silanised slides.
Biopsy staining
A modified three layered immunoperoxidase staining method was used as previously described15 and sections were stained with goat anti-type I and III collagen (Southern Biotechnology, Birmingham, Alabama, USA). Positive staining was developed by incubation with DAB chromogen and slides were counterstained with Mayer's haematoxylin. Each staining run included a negative isotype IgG1 control slide. Slides were assigned a number from a random code and read blind to time, treatment, and patient group.
EBB quantification
Subepithelial reticular basement membrane (rbm) thickening was assessed using sections immunostained for collagen I. This method was prospectively decided upon after a pilot study comparing EBB sections stained with collagen I and collagen III, using immunohistochemistry, as well as sections stained cytochemically with haematoxylin and eosin and toluidine blue. Collagen I consistently gave the sharpest delineation of rbm thickness suitable for subsequent image analysis, as assessed by a panel of three observers (MP, CW, and EHW).
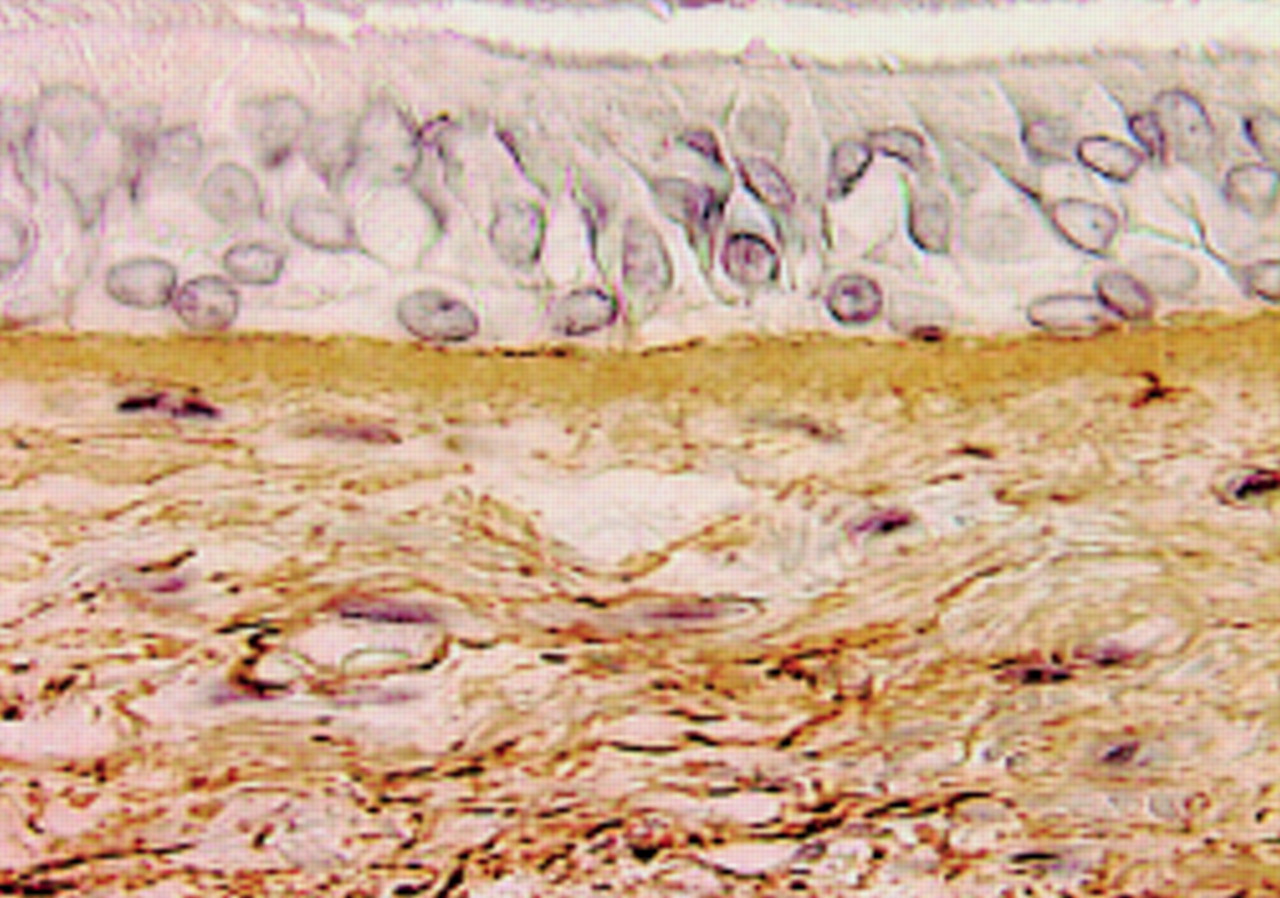
A single experienced observer (MP) made measurements of rbm from the base of the bronchial epithelium to its outer limit. The measurement therefore included the “true” basement membrane as well as “reticular components”. An image analyser (Image Pro Plus 4.0, USA) was used to score all the rbm in a whole well preserved section by drawing two lines that demarcated it. The method, which was calibrated against a standard graticule for each scoring session, avoided any potential subjectivity by measuring all the available rbm. In all cases a total length of >2 mm was quantified, giving a sample that substantially exceeds a recently recommended total of 1 mm for such estimations.9 An example of a typical photomicrograph of collagen I staining of an EBB section is shown in fig 1.

Photomicrograph (Image Pro plus video capture) showing subepithelial reticular basement membrane thickening as denoted by collagen immunohistochemistry with further more diffuse staining in the lamina propria.
Diffuse collagen staining in the lamina propria for collagen I and collagen III was assessed using the same interactive computerised image analysis system (Image Pro Plus). At least five consecutive non-overlapping fields below the area quantified as rbm were defined by a single experienced observer (CW) to a depth of up to 150 μm below the basement membrane, with smooth muscle excluded. For the most part these five regions represented all the available lamina propria, again to avoid subjectivity in sampling. Positive collagen staining was expressed as percentage positive staining of the total area using a preset colour detection threshold to create a mask of the positive staining area. This colour setting was kept on the computer memory and applied to all the specimens quantified so that the same definition of “positive staining” was used throughout the study. The intraobserver coefficient of variation for this method was 8%.
Analysis of data
BAL cell data were analysed as percentages with absolute counts. Analyses were performed according to the distribution of the data with or without log transformation. PD20 data are presented as geometric means and 95% confidence intervals (CI). Spirometric parameters are presented as least square means with standard errors using the multiparametric generalised linear model for analysis. Where appropriate, non-parametric Mann-Whitney tests were used to assess the differences between the effects of the treatments. 23 asthmatic subjects had complete data for all seven study visits, and these data are presented in summary measurements. Analyses of the treatment effects were also carried out on differences over time using all the available data in a generalised linear model; this allowed subjects with incomplete data to be included in the analyses. There were no differences in the results when these two approaches were used. Asthmatic subjects who became non-responsive to the maximum dose of methacholine used for BHR determination (6.4 mg) following treatment were all assigned an arbitrary value of 12.8 mg for analytical purposes.
Univariate Pearson correlations were calculated for log transformed data. A stepwise multiple regression procedure was then used to construct a model for BHR using variables indicated by the univariate analysis. This resulted in the determination of partial R2 values for significant variables. R2 values are also sometimes referred to as “coefficients of determination” and are dimensionless measures ranging from 0 to 1. A model R2 value of 0.4 would indicate that 40% of the variability in the outcome variable could be explained by the variables included in the model. The model was built up by sequential addition of variables such that the partial R2 value for epithelial cells and eosinophils was gained by adding these terms into a model already containing rbm thickening and epithelial cell variables. The model was validated with a backward elimination procedure and non-significant terms were removed. GLM and multiple regressions were made using SAS statistical software; Minitab for Windows was used elsewhere.
RESULTS
Withdrawals, clinical efficacy and safety
Five patients withdrew from the study because of worsening asthma symptoms coupled with lack of efficacy of the study medication, all from the placebo group (p=0.02, Fisher's exact test). One patient on FP treatment withdrew because of throat irritation; there were no other adverse events attributable to FP treatment.
Baseline data
Physiology
At baseline the subjects assigned to the two groups were comparable for age, sex, and height. Baseline FEV1 was 96 (27)% predicted and 94 (21)% predicted in the FP and placebo groups, respectively (p=0.9), and MMEF25–75 iin the two groups was 60 (39)% predicted and 55 (25)% predicted (p=0.7). Levels of BHR in the two groups were similar with geometric mean PD20 values of 71 (95% CI 23 to 221) μg in the FP group and 32 (95% CI 9–112) μg in the placebo group.
Airway inflammation
Baseline BAL fluid data are summarised in table 1. A typical asthmatic BAL fluid inflammatory cell profile was seen with an increased % median (range) of eosinophils (1.8 (0–23) v 0.6 (0–6.4), (p<0.01)), mast cells (0.1 (0–0.58) v 0.02 (0–0.12), (p<0.0001)), and epithelial cells (2.6 (0.3–17.6) v 1.4 (0–10.4), (p<0.01)) compared with the controls.
Baseline median (range) BAL fluid total cell count (TCC) and differential counts for asthmatic and normal subjects
Subepithelial reticular basement membrane (rbm) thickening
As expected, rbm thickness was variable in the biopsy specimens assessed. Nevertheless, there was a significant overall increase in mean (SD) rbm thickness in asthmatic patients compared with controls: 9.1 (2.2) μm v 7.7 (1.2) μm (95% CI for difference 2.3 to 0.5 μm, p<0.01, fig 2)

Comparison of reticular basement membrane (rbm) thickening in asthmatic and normal subjects (medians represented by horizontal lines).
Longitudinal data
Physiology
There was a small but significant improvement in FEV1 following 3 months of treatment with FP from 3.44 (0.14) l to 3.60 (0.12) l (p<0.01, p<0.05 v placebo group, 95% CI for change 0.03 to 0.57) with no further improvement at 6 or 12 months. Placebo had no effect. There was also a significant improvement in MMEF25–75 following 3 months of treatment with FP from 3.20 (0.25) l/min to 3.55 (0.20) l/min (p<0.01, p<0.05 v placebo group, 95% CI for change 0.04 to 0.90), with no further significant change at 12 months. Placebo had no effect (fig 3).

Effect of treatment for 3, 6 and 12 months with FP (closed circles) and placebo (PL) (open circles) on (A) FEV1 and (B) MMEF25–75. Least squared mean (SE) values are displayed and the data are normalised so that the baseline data represent 100%.
There was a large and significant change in PD20 from the baseline value to 302 (95% CI 86 to 1070) μg following 3 months of treatment with FP (p<0.001). Unlike airflow values, PD20 continued to improve, increasing to 726 (95% CI 606 to 1307) μg at 6 months and 5370 (95% CI 1011 to >6400) μg at 12 months (p<0.0001 v baseline). Following cessation of FP treatment PD20 deteriorated significantly at 1 month follow up to 490 (95% CI 152 to 1560) μg (p<0.01 v 12 month value; fig 4). There were no changes from baseline in the placebo group at 3 months (42 (95% CI 12 to 141) μg) or at 12 months (43 (95% CI 10 to 189) μg). The difference between FP and placebo treatments was significant throughout all comparisons (p<0.001)—for example, the 95% confidence intervals for change (expressed as dimensionless ratios due to the logarithmic analyses) between the two groups at 3 months were 3–6 fold (p<0.001) and at 12 months were 22–633 fold (p<0.000, fig 4).
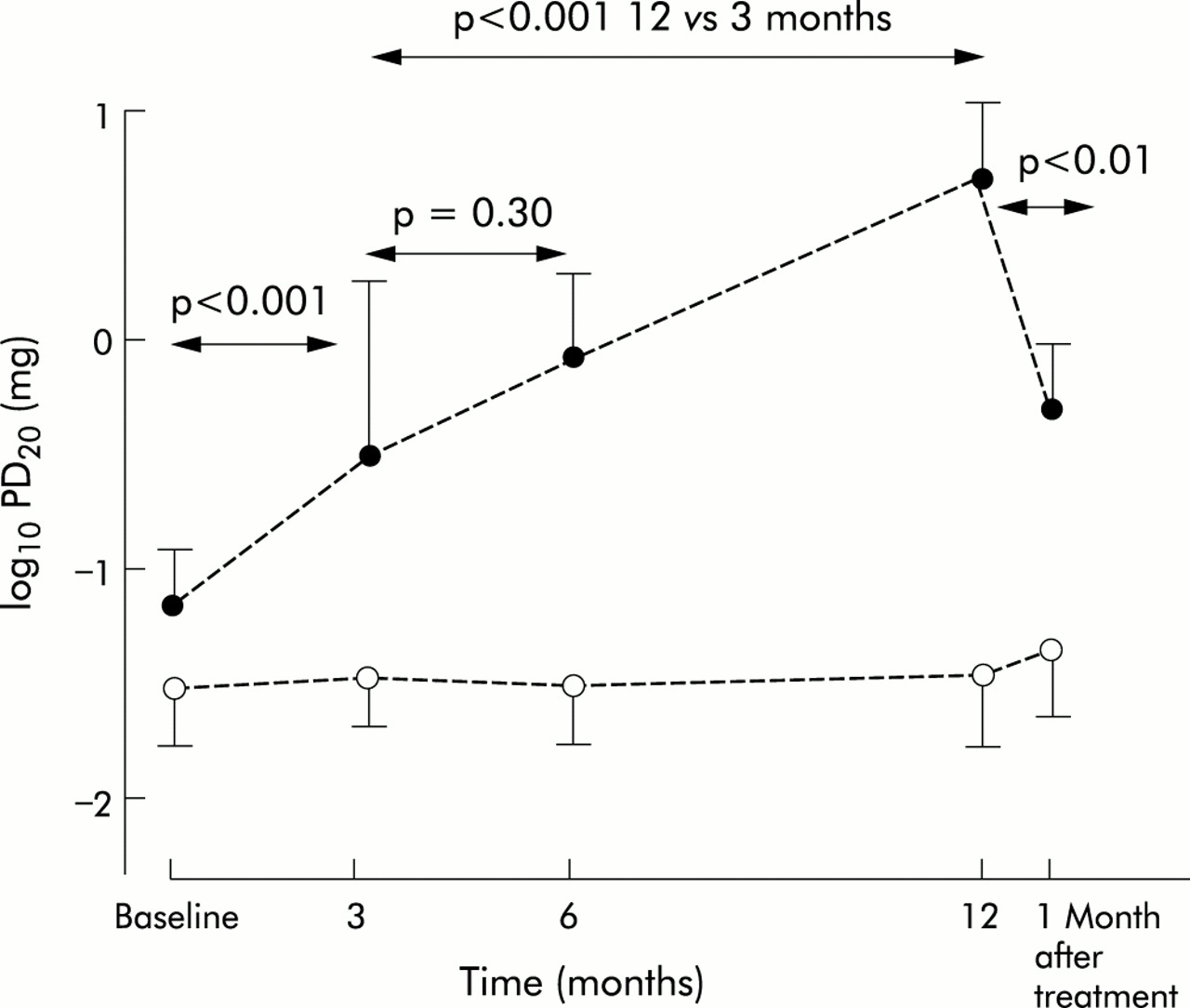
Effect of 3, 6, and 12 months of treatment with FP (closed circles) and placebo (PL) (open circles) on log10 PD20 FEV1 to methacholine (geometric mean (SE) values).
Airway inflammation
There were no changes in BAL inflammatory cell counts following placebo treatment but there were significant reductions in BAL eosinophils, mast cells, and epithelial cells following 3 months of treatment with FP (p<0.05) which essentially normalised the BAL cell profile. There were no further changes following 12 months of treatment (fig 5).

Comparison of changes in % BAL eosinophils for FP (closed circles) and placebo (PL) (open circles). **p<0.01 v baseline; p<0.05 v placebo.
Subepithelial reticular basement membrane (rbm) thickening
There was no difference in rbm thickness following 3 months of treatment with FP but at 12 months there was a significant decrease in rbm thickness from 10.1 (2) μm to 8.2 (2) μm (p<0.01, 12 months FP v baseline; p<0.05 12 months FP v 3 months; fig 6). There was no significant difference in rbm thickness following treatment with placebo at any time (fig 6). The difference between FP and placebo data was significant (95% CI for difference –4.4 to 0.2 μm, p<0.05).

Comparison of changes in rbm thickness for FP (closed circles) and placebo (PL) (open circles). **p<0.01 12 months FP v baseline; p<0.05 v placebo.
Diffuse collagen staining in the lamina propria
Data for diffuse collagen staining for subtypes I and III are summarised in table 2. There were no effects of treatment with either FP or placebo and no difference was observed from control data at baseline.
Mean (SE) percentage collagen staining by area in the lamina propria of biopsy specimens from asthmatic and normal subjects with follow up data in the asthmatics following 3 and 12 months of treatment with inhaled fluticasone propionate (FP) or placebo (PL)
Cross sectional relationships between inflammatory cell physiology and rbm thickening
Univariate analyses
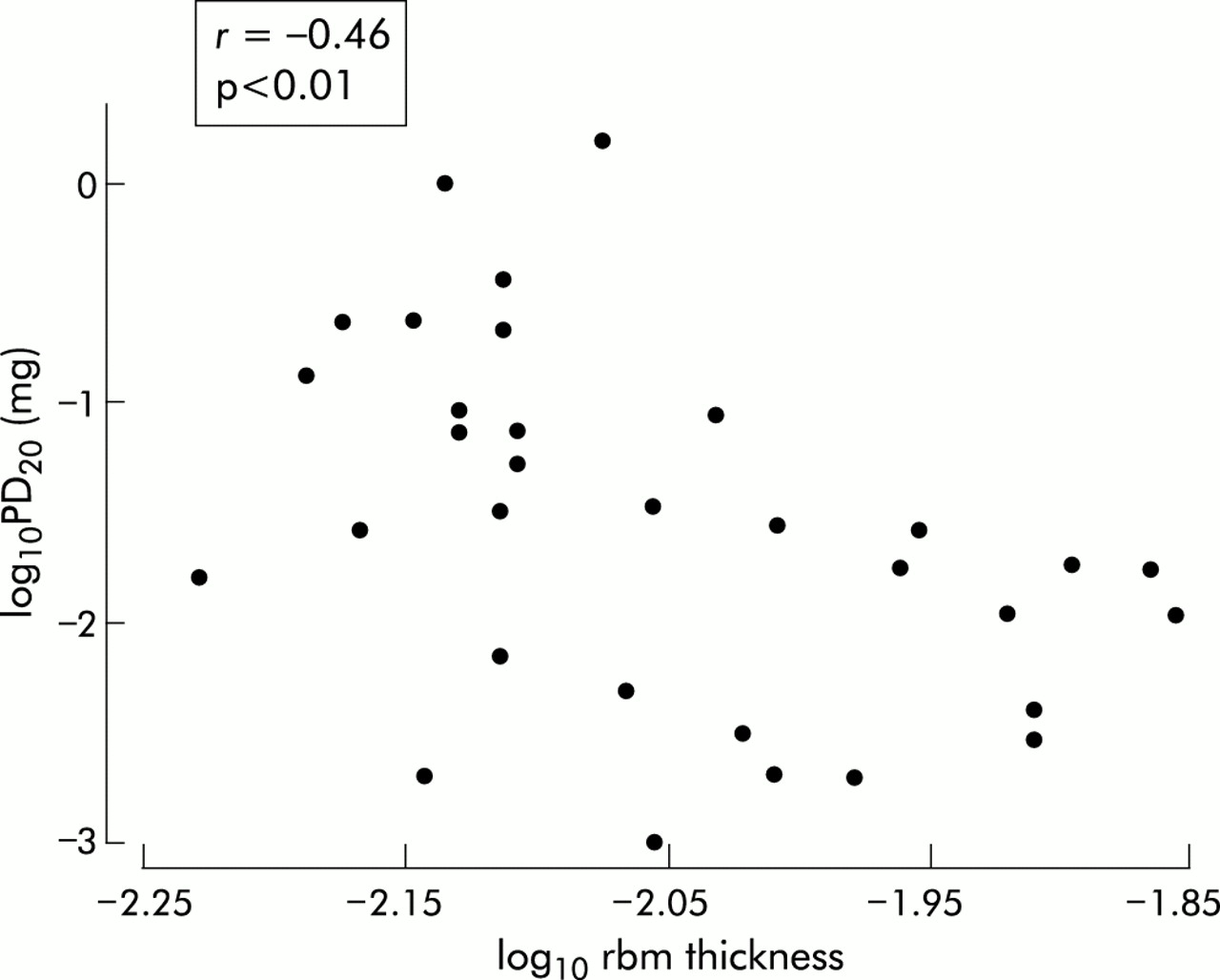
A limited series of correlation analyses were performed to explore potential relationships between inflammation, rbm thickening, and physiology. No correlations or trends were observed between spirometric indices and inflammatory cell counts or rbm thickening, but there were significant correlations between log10 baseline BAL eosinophils and mast cells and log10PD20 (BHR) (r=–0.34, p=0.05 and r=–0.37, p=0.03, respectively). There was a significant correlation between log10 mast cells and log10 rbm thickness (r=0.48, p=0.006, fig 7) and between BHR and log10 rbm thickness (r=–0.46, p<0.01, fig 8).

Correlation between log10 % BAL mast cells and log10 rbm thickness at baseline.

{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
Correlation between log10 rbm thickness and log10 PD20FEV1 to methacholine (mg) at baseline.
Multiple regression analyses
Based on the results of the univariate analysis, mast cells and eosinophils were used in a model as possible predictors of rbm thickness. The only significant predictor for rbm thickness was mast cells, with R2=0.23 (p=0.008). For BHR, baseline spirometric values, log10 eosinophils, mast and epithelial cells were considered as potential predictors. In addition, log10 rbm thickness was included to dissect the relative contributions of airway remodelling and inflammation towards the predictive model. The inclusion of baseline spirometric parameters had a partial R2 of 0.0006 (p=0.7) while log10 mast cells had a partial R2 of 0.009 (p=0.55); these terms were therefore removed from the model. In contrast, log10 rbm thickening had a partial R2 of 0.21 (p=0.009), log10 epithelial cells had an R2 of 0.11 (p=0.04), and log10 eosinophils had an R2 of 0.08 (p=0.046). The overall R2 of the model was 0.40, indicating that 40% of the variability in BHR cross sectionally at baseline could be explained by rbm thickness (21%), epithelial cell numbers (11%), and eosinophil numbers (8%).
A breakdown of the multiple regression analysis for BHR to methacholine is given in table 3.
Breakdown of multiple regression analysis for bronchial hyperresponsiveness to methacholine
Relationships between inflammation, remodelling, and BHR with time
The improvement in BHR with FP at 3 months represented a change in PD20 of 2.1 doubling doses and occurred over the same time as normalisation of airway inflammation. The total change in PD20 following 12 months of treatment was 6.2 doubling doses, with the change between 3 and 12 months representing 4.1 doubling doses. This greater secondary improvement in BHR was associated with a significant decrease in rbm thickness. Of the total change in rbm thickness over 12 months (–1.9 μm), approximately 90% occurred in the 3–12 month treatment period. Thus, one third of the total improvement in BHR was associated with early changes in airway inflammation but the remainder was associated with the more refractory improvement in airway remodelling.
DISCUSSION
We have explored the relationship between airflow, BHR, airway inflammation, and airway remodelling in asthma and were able to construct a model from our cross sectional data which indicated that, while airway inflammation was an important component for BHR, remodelling represented a stronger predictor. With this model, 40% of the variability in BHR could be explained by multiple regression containing remodelling and inflammatory components (rbm thickness 20%, epithelial cells 11%, eosinophils 8%). A long term prospective intervention study was then used to evaluate the effect of high dose ICS treatment at multiple time points to validate this model. The results of this intervention limb corroborated our cross sectional analysis, indicating that approximately one third of the improvement was associated with improvement in airway inflammation and two thirds were associated temporally with changes in airway remodelling. These data are novel and, as far as we are aware, are the first to dissect the relative contribution of airway inflammation and remodelling to BHR and to elucidate their relative temporal improvements with ICS.
Our study advances the rather sparse body of knowledge available about airway remodelling and its relationship with other elements of the asthmatic phenotype at a number of levels. A review of the available literature indicates that there is considerable divergence, with different methods being used to measure rbm thickening and >100% variation across studies for published measurements in normal and asthmatic subjects (ranging in asthmatic patients from 7.4 (2.5) μm to 23.1 (3.4) μm2,16–18). In spite of the between study variability of absolute measurements, a relatively thickened rbm has been found consistently in asthmatic endobronchial biopsy specimens.2,16–19 However, a recent study by Chu et al2concluded that rbm thickening is not a clearcut finding in asthma and does not differentiate between asthmatics of varying severity. The authors discussed the limitations of defining asthma severity on the basis of different levels of corticosteroid treatment, pointing out that the effect of treatment probably introduces ambiguity into the interpretation of such asthma investigations.
As well as uncertainty about the strength of rbm thickening in defining asthma severity, the literature on the effect of ICS in airway remodelling is confused and contradictory. The evidence that exists comes mainly from small studies with unconvincing data.19–21 Indeed, the available literature on airway remodelling was recently described by Fish and Peters10 as “largely speculative and perhaps too tautologic”, and there have been recent calls for more studies relating indices of asthma activity with indices of remodelling.1,10,12,22 We provide fresh data indicating potential links between pathological and physiological abnormalities and their relative responses to “disease modifying” treatment. We found that, relative to normal controls, rbm thickening was present even in mild asthmatics who were receiving as needed β2 agonist medication only. However, the difference is subtle and variable. As in the study by Chu et al,2 our data indicated a considerable overlap between asthmatic and normal subjects and support the view that this aspect of airway remodelling does not necessarily discriminate individual asthmatic patients from normal subjects in the dichotomous manner implied by some studies.19 However, it is generally present in asthmatic patients as a group, does seem to be related to physiological change, and can be positively affected by ICS, although this needs to be for a longer term than is needed to treat the acute manifestations of asthmatic airway inflammation.
Our finding of a decrease in rbm thickness following 12 months of treatment with FP supports a limited number of intervention studies that have shown such an effect of ICS,16,23–25 in addition to their somewhat better documented ability to reduce airway inflammation following much shorter treatment periods.7,16,26 However, our finding that the change was not observed following 3 months of treatment with FP even at high doses was also important, and it is interesting that the latest available study of the effect of treatment with FP at a dose of 1000 μg/day for 2 months was negative.27 The slow onset of change in rbm thickness that we observed may be a possible reason why this and other previous studies with different doses and treatment durations might not have observed an effect of ICS.20,21,28 Our data also indicated that studying patients on different background baseline levels of ICS might indeed significantly distort any relationship between disease activity and airway remodelling in cross sectional designs, as suggested by Chu et al.2
We prospectively analysed airway inflammation from BAL differential cell counts. The decision to use BAL cell data was based on extensive work evaluating therapeutic interventions that showed that BAL fluid and biopsy specimens gave complementary and concordant information on airway inflammation, although in general BAL gave more robust and consistent signals.15,29 Our study gives new evidence to support the paradigm that airway inflammation, particularly mast cells, might be associated with the development of airway remodelling.30 We found that mast cells were not a significant predictive term in the multiple regression model for BHR but that, in contrast, in the multiple regression for remodelling 23% of the variability of rbm thickness could be explained by variation in the percentage of mast cells in the BAL fluid. We consider that the reduction in rbm thickness seen only in the 12 month biopsy sample, the correlation between mast cells and rbm thickness, and the finding that inflammation has been cleared by 3 months of treatment with FP suggest that airway remodelling may represent a consequence of airway inflammation.
Mast cells, in particular, have long been considered as potentially important in airway remodelling in asthma. They are present in other fibrotic pathologies and are equipped with an array of preformed and newly generated inflammatory mediators including histamine, neutral proteases, tryptase, heparin sulphate, prostaglandins, cysteinyl leukotrienes, as well as a range of cytokines, growth factors and chemokines.30 Despite the potential key importance of mast cells, knowledge of their role in airway diseases is limited and a recent editorial indicated that this was a key area for further research.30 Our findings are, to our knowledge, the first to include a prospective longitudinal component, but are supported by limited cross sectional data studying airway inflammation and the genesis of airway remodelling.31 In addition, a descriptive longitudinal study by Laprise et al has suggested that airway inflammation precedes rbm thickening, even in newly diagnosed asthma.32
The potential mechanism by which rbm thickening contributes to any functionally important changes has been brought into question,2,17 and it has been suggested that it does not relate to other “remodelling” changes which may be functionally more important but may simply be an unrelated epi-phenomenon. It is reasonable to consider this, and also to recognise that correlation does not imply causation. However, in a recent study by James et al rbm thickening was statistically related to several other parameters of remodelling.33 This study was performed on whole resected lung specimens with which this group has provided important pathophysiological asthma data.33–35 Rbm thickening has the considerable advantage of being an index that can be measured on airway biopsy specimens and can be followed sequentially in longitudinal studies.
Few studies have investigated diffuse collagen deposition in the lamina propria of asthmatic biopsy specimens and no published longitudinal studies have been found on the effect of ICS treatment. The lack of difference in diffuse interstitial collagen deposition between asthmatic and normal subjects was surprising, as this was in contrast to a previous smaller cross sectional study from this laboratory17 but agreed with the more recent work by Chu et al.2 In our 12 month longitudinal study we did not detect any effect of treatment with ICS. It would seem reasonable to conclude, even from the limited accumulated experience, that frank alteration of diffuse collagen deposition in the lamina propria is not a universal or necessary finding in asthma.
Current guidelines advocate the titration of ICS dosages against symptoms and spirometric data, with the requirement that they be minimised to a level consistent with stabilising the conventional clinical end points.6 We found that 3 months of treatment with FP resulted in maximal improvements in spirometric parameters and airway inflammation. There was good symptomatic control with FP over the period of the study, perhaps not surprisingly given the large dose used. Even so, in terms of current management guidelines this would have meant that treatment would have been stepped down at that point, before the maximal benefit in BHR or significant change in airway remodelling had been realised. There is active debate about the possible role of objective non-invasive tests of airway inflammation in asthma management,36,37 so much effort has been put into induced sputum studies and exhaled breath measurements of inflammatory products.36–39 It is therefore of some interest that our data indicated that the inclusion of information on the response of airway inflammation in the management paradigm would not, in fact, have altered the decision to reduce treatment at 3 months. We are not suggesting that the high dose of ICS used in our study is clinically appropriate in patients with mild asthma as all the changes we observed may well have been achieved with a much lower dose. However, we wish to highlight the fact that current guidelines for the management of asthma are not entirely satisfactory and do not indicate the length of time ICS should be administered for optimal effect.
In contrast to spirometric parameters and airway inflammation, BHR continued to improve over the same time period as changes in airway remodelling, with improvements in both rbm thickness and PD20 occurring with 12 months of treatment. We therefore feel that our findings are important, supporting the view that BHR is a composite reflection of airway inflammation and remodelling in asthmatic patients.1 The lack of specificity for any one part of the pathophysiology of asthma may actually represent a strength of the BHR measurement, since it would seem prudent to target treatment strategies towards both inflammation and remodelling. Optimising improvement in BHR would seem to be potentially practicable, with internationally standardised methodologies available.40
In summary, we have constructed a model which indicated that, while airway inflammation and remodelling were important predictors for BHR in asthmatic patients, rbm thickening represented the strongest single predictor. These cross sectional data were corroborated in a long term prospective intervention study which confirmed associations between airway remodelling, inflammation, and BHR. Our data support the need for early and long term intervention with ICS even in relatively mild asthmatics, and the need to assess further the potential merit of longitudinal BHR testing in patient management, since this may reflect both airway inflammation and remodelling.
Acknowledgments
The authors acknowledge the commitment of the patient volunteers, Michael Bailey for statistical analysis, the technical assistance of Ms Sally Gollant (patient recruitment), Drs Xun Li and Frank Thien (bronchoscopies), Ms Tiffany Bamford (bronchoscopic sample reception), and Associate Professor John Wilson for contributing to protocol development.
REFERENCES
Footnotes
-
Supported by NHMRC Australia, The Alfred Foundation and Glaxo-Wellcome Australia.
-
Chris Ward is a European Respiratory Society Long Term Research Fellow.