Article Text

Abstract
BACKGROUND Chronic obstructive pulmonary disease (COPD) is common although often poorly characterised, particularly in primary care. However, application of guidelines to the management of such patients needs a clear understanding of the phenotype. In particular, the British guidelines for the management of COPD recommend that the diagnosis is based on appropriate symptoms and evidence of airflow obstruction as determined by a forced expiratory volume in one second (FEV1) of <80% of the predicted value and an FEV1/VC ratio of <70%.
METHODS A study was undertaken of 110 patients aged 40–80 years who had presented to their general practitioner with an acute exacerbation of COPD. The episode was treated at home and, when patients had recovered to the stable state (two months later), they were characterised by full lung function tests and a high resolution computed tomographic (HRCT) scan of the chest.
RESULTS There was a wide range of impairment of FEV1 which was in the normal range (⩾80%) in 30%, mildly impaired (60–79%) in 18%, moderately impaired (40–59%) in 33%, and severely impaired (<40%) in 19% of patients. A reduced FEV1/VC ratio was present in all patients with an FEV1 of <80% predicted but also in 41% of those with an FEV1 of ⩾80% predicted. Only 5% of patients had a substantial bronchodilator response suggesting a diagnosis of asthma. Emphysema was present in 51% of patients and confined to the upper lobes in most (73% of these patients). HRCT evidence of bronchiectasis was noted in 29% of patients and was predominantly tubular; most (81%) were current or ex-smokers. A solitary pulmonary nodule was seen on 9% of scans and unsuspected lung malignancy was diagnosed in two patients.
CONCLUSIONS This study confirms that COPD in primary care is a heterogeneous condition. Some patients do not fulfil the proposed diagnostic criteria with FEV1 of ⩾80% predicted but they may nevertheless have airflow obstruction. Bronchiectasis is common in this group of patients, as is unsuspected malignancy. These findings should be considered when developing recommendations for the investigation and management of COPD in the community.
- chronic obstructive pulmonary disease
- bronchiectasis
- lung function tests
- radiology
Statistics from Altmetric.com
By the year 2020 chronic obstructive pulmonary disease (COPD) is predicted to become the fifth leading cause of morbidity and mortality.1 Already in primary care it accounts for 2665 consultations per 10 000 person years at risk2 which is comparable to that for angina pectoris. Despite being a major health care burden, clinical management has mainly been empirical until publication of the British Thoracic Society guidelines for the management of COPD3 intended for both primary and secondary care physicians.
It is well recognised that the generic term COPD includes patients with a variety of conditions including emphysema, chronic bronchitis, and chronic asthma which may occur alone or in combination.4-6 The common feature of these disorders is longstanding airflow obstruction which does not change markedly over a period of months,3 ,7 although it is accepted that there may be some reversibility of the airflow obstruction in response to bronchodilators.3 ,5 ,7 The British Thoracic Society (BTS) recommends the use of spirometric tests to detect airflow obstruction and confirm the diagnosis of COPD by impairment in forced expiratory volume in one second (FEV1) with little response to inhaled bronchodilators. However, spirometric testing is not widely available in primary care and thus the diagnosis of COPD is often based on clinical symptoms and signs, even though these correlate poorly with lung function.8-10
Patients in primary care with a diagnosis of COPD may therefore be more heterogeneous with respect to their underlying disorder and degree of lung function impairment than those diagnosed in secondary care. The situation is further compounded by difficulty in differentiating COPD from asthma in primary care; this will be critical for the provision of health services and future research in COPD, which will focus increasingly on primary care. For instance, many phase IV clinical trials are carried out in primary care and the results are used to determine clinical practice, often across all health care sectors.
It is therefore important to document the nature of COPD diagnosed in primary care in order to determine the relevance of national guidelines to the management of these patients and interpretation of clinical trials performed in the community.
We have studied 110 patients with a primary care diagnosis of COPD who presented to their general practitioner with an acute exacerbation of their disease. All patients underwent full lung function testing and CT scanning with a high resolution algorithm when they had recovered to their stable state to determine their physiological and radiological characteristics.
Methods
From September 1996 until August 1998 we studied patients aged 40–80 years managed in the community whose general practitioner had diagnosed an acute exacerbation of COPD associated with sputum production. Forty four general practitioners in 29 surgeries participated. Six surgeries referred more than 10 patients each, a further six practices each referred 5–10 patients, and the remaining surgeries entered 1–4 patients. All general practitioners used the same criteria to define an exacerbation, including one or more of increased breathlessness, sputum volume and purulence, with or without worsening of any other symptoms (cough, increased sputum viscosity, wheeze, chest pain, malaise, fever, chills) that prompted the patient to seek advice and treatment from their general practitioner. Patients who were thought to require treatment with oral corticosteroids or hospital admission were excluded from the study. Treatment for the exacerbation was given according to the study protocol: patients with (muco)purulent sputum received an antibiotic and patients with mucoid sputum an inhaled steroid or placebo. Patients were reviewed two months later when they had recovered to their stable clinical state, defined as complete resolution of the acute symptoms without a change in medication or symptoms in the previous four weeks. Full lung function tests and a high resolution CT scan of the chest were carried out on the same day. A total of 182 patients were referred for entry and 131 were recruited into the study. Among the 51 patients who did not enter the study, 18 declined to participate, 11 had been unstable in the four weeks before the current exacerbation, 11 did not have an exacerbation, six were unable to provide a sputum sample, four needed hospitalisation or treatment with prednisolone, and one patient was blind. Twenty one patients participated in the study but were not characterised with lung function tests and a CT scan (16 patients declined, three were found to have a fresh exacerbation on the day of the assessment, one patient was lost to follow up, and one died of overwhelming pneumonia).
Where possible, a spontaneously expectorated sputum sample was collected on the morning of the assessment day. Its macroscopic appearance was assessed by experienced laboratory staff and allocated a number depending on the degree of purulence by reference to a standard colour chart (Bronkotest, Heredilab, Utah, USA). This chart was based on the principle that increasing colouration of sputum from mucoid (0–2) to mucopurulent (3–5) and purulent (6–8) occurs as the concentration of myeloperoxidase rises, reflecting increasing numbers of neutrophils in the airway secretions.11
Full lung function tests were performed according to national guidelines.12 Dynamic lung volumes (FEV1, forced vital capacity (FVC), and relaxed vital capacity (VC)) were measured on a wedge bellows spirometer (Vitalograph, Buckinghamshire, UK). Static lung volumes were measured by helium dilution and gas transfer by the single breath carbon monoxide method using the Benchmark system from Morgan Medical (Kent, UK).
Reversibility of airflow obstruction was assessed by spirometric tests 20 minutes after administration of inhaled salbutamol (400 μg). To determine any additional effect inhaled ipratropium bromide (60 μg) was then administered and spirometric testing was repeated after a further 45 minutes. Both drugs were given via a large volume spacer device under the supervision of trained staff and all measurements were corrected to body temperature and pressure saturated with water vapour (BTPS). Reference equations for the calculation of predicted values were those produced by the European Community for Steel and Coal.12
After lung function tests had been completed a high resolution CT scan of the chest was performed. One millimetre slices were obtained at 10 mm intervals in inspiration with an acquisition time of one second for each slice. Window width was set at 2000 Hounsfield units (HU) and window level at –700 HU. Scans were initially reported by a specialist respiratory radiologist and then reviewed again, without knowledge of the first report, six months later together with a chest physician for the presence of bronchiectasis. The presence and type of bronchiectasis were determined by consensus. Criteria for the diagnosis of bronchiectasis were lack of tapering, visibility of bronchi within 1 cm of the pleura and bronchial dilatation (bronchial diameter larger than that of the accompanying pulmonary artery; avoiding slices close to bronchial bifurcation).13 Bronchiectasis was described as cystic, varicose, or tubular (cylindrical) according to the criteria first described by Naidich et al 14 and recently reviewed by Hansell.13
Emphysema was identified as areas of well demarcated low density without a perceptible wall associated with attenuation and distortion of the lung vasculature. Changes ranged from small focal areas of destruction with normal surrounding lung (centrilobular emphysema) to frank confluent destruction (panacinar or advanced centrilobular emphysema).15 Emphysema was characterised as limited when confined only to the upper lobes and extensive when it also involved the lower and/or middle lobes.
Data with a normal distribution are presented as the mean (SD) and were compared statistically using the Student'st test for unpaired data. Multiple means were compared with the one way ANOVA using Tukey's test for post-hoc comparison only when the results of the ANOVA were significant at a level of p<0.05. Data was logarithmically transformed where necessary to fulfil the requirement for equal variances. Any data with a skewed distribution were summarised as medians with quartiles and compared using non-parametric tests. Proportions were compared using the χ2 test (Fisher's exact test where appropriate). Two sided tests were used. Statistical analysis was carried out using SPSS version 8.0.
The study was approved by the University of Birmingham NHS Trust Research Ethics Committee.
Results
A total of 110 patients underwent HRCT scanning of the chest and 108 completed lung function tests technically valid for analysis (although a further two did not complete bronchodilator reversibility testing and one patient declined to have static lung volumes measured).
Details of age, sex, smoking history, use of inhaled steroids, and co-morbidity are shown in table 1. The group was predominantly male (58%), 49% were ex-smokers and 45.5% were current smokers, and 48% were receiving long term inhaled steroid therapy.
Demographic information for all patients and for those with full lung function tests stratified by degree of impairment of FEV1
Co-morbid conditions were present in 44 patients and included hypertension (n = 24), ischaemic heart disease (n = 19), atrial fibrillation (n = 4), diabetes mellitus (n = 7), cerebrovascular disease (n = 5), and peripheral vascular disease (n = 4). Fifteen patients had more than one co-morbid condition (most commonly hypertension with ischaemic heart disease).
LUNG FUNCTION TESTS
Pre-bronchodilator spirometry
One hundred and eight patients completed pre-bronchodilator spirometric tests. The patients were stratified according to the degree of impairment of the FEV1 expressed as a percentage of the value predicted for age, sex, and height and classified as normal (⩾80%), mildly (60–79%), moderately (40–59%) or severely impaired (<40%) as recommended in the national guidelines.3
Thirty two patients (30%) had a normal FEV1, 19 (18%) had mild impairment, 36 (33%) moderate impairment, and 21 (19%) severe impairment of FEV1. There was no difference in age between the four groups (table 1) and the ratio of men to women was similar in all groups except those with severe impairment of FEV1where men predominated (p = 0.0035). Median consumption of cigarettes measured in pack years was not significantly different between the four groups but there were more ex-smokers among those with severe impairment of FEV1 (p = 0.02) and a larger proportion (81%) of patients with severe impairment of FEV1 were receiving long term inhaled steroids (p<0.0005).
Table 2 shows the mean values for FEV1, FVC, and relaxed VC for each of the four groups. The FEV1 showed the expected differences between the groups classified by the BTS criteria but both relaxed and forced vital capacity were preserved within the normal range in patients with mild and moderate disease. However, the mean value for (F)VC (percentage predicted) for these patients was at the lower end of the normal range and significantly lower than for patients without impairment of FEV1 (difference of the means for FVC and VC between patients with mild and no impairment of FEV1 15.4 percentage points (95% CI 7.5 to 23.3, p = 0.0001) and 14.9 percentage points (95% CI 6.7 to 23.0, p = 0.0003); difference of the means for FVC and VC between patients with moderate and no impairment of FEV1 21.1 percentage points (95% CI 14.1 to 28.1, p<0.0001) and 17.1 percentage points (95% CI 9.7 to 24.6, p<0.0001)). Patients with severe disease had average values for FVC and VC below the normal range (difference in the means for FVC and VC 41.5 percentage points (95% CI 33.2 to 49.7, p<0.0001) and 37.3 percentage points (95% CI 29.2 to 45.4, p<0.0001) compared with patients with a normal FEV1).
Pre-bronchodilator spirometric data for 108 patients separated by degree of impairment of FEV1
Impairment of the FEV1/FVC or FEV1/VC ratios worsened with the severity of disease (table 2). In the group of 32 patients without impaired FEV1 13 had an abnormal FEV1/VC ratio (<70%) ranging from 46.6% to 68.8% but only 11 had an abnormal FEV1/FVC ratio.
Post-bronchodilator spirometry
One hundred and six patients completed spirometric tests after the inhalation of both bronchodilators. For patients with no impairment of FEV1 and an FEV1/VC ratio of ⩾70% the difference between the mean pre- and post-bronchodilator value for FEV1 was 181 ml (95% CI 121 to 240, p<0.0001); for those with no impairment of FEV1 but an FEV1/VC ratio of <70% the difference between the means was 317 ml (95% CI 125 to 509, p = 0.0001); and for those with mild, moderate, and severe disease the differences in the means were 258 ml (95% CI 203 to 314, p<0.0001), 352 ml (95% CI 286 to 419, p<0.0001), and 250 ml (95% CI 185 to 314, p<0.0001), respectively.
The difference between the mean pre- and post-bronchodilator VC was 137 ml (95% CI 50 to 223, p = 0.0007) for patients with no impairment of FEV1 and an FEV1/VC ratio of ⩾70%; 242 ml (95% CI 71 to 413, p = 0.001) for patients with no impairment of FEV1 and an FEV1/VC ratio of <70%; 310 ml (95% CI 213 to 407, p<0.0001) for patients with mild disease; 453 ml (95% CI 348 to 558, p<0.0001) for patients with moderate disease, and 505 ml (95% CI 365 to 646, p<0.0001) for patients with severe disease.
When disease severity was assessed using the post-bronchodilator FEV1 (% predicted value), 43 patients (41%) were classified as normal whereas 33 patients (31%) were classified as mildly impaired, 17 (16%) as moderately impaired, and 13 (12%) as severely impaired.
Reversibility
One hundred and six patients underwent reversibility testing, of whom 19 (18%) had a normal FEV1 (⩾80% predicted) and no evidence of airflow obstruction (FEV1/VC ⩾70%); 13 (12%) had a normal FEV1 but an impaired FEV1/VC ratio of <70%; 18 (17%) had severe impairment of FEV1, 35 (33%) had moderate impairment, and 21 (20%) had mild impairment of FEV1. The BTS guidelines define a significant bronchodilator response as an increase in FEV1of at least 200 ml and 15% from the baseline value. Such a response to either salbutamol or ipratropium bromide alone was seen in three patients (23%) with a normal FEV1 and airflow obstruction, in seven patients (39%) with mild impairment, in 19 (54%) with moderate impairment, and in eight (38%) with severe impairment of FEV1. The absolute bronchodilator response showed a wide range (fig 1) and in 11 patients the FEV1 increased to above 80% of the predicted value from a median pre-bronchodilator FEV1 of 72.2% (IQR = 65.2–76.7) to 83.5% (IQR = 81.1–86.5).

Number of patients with significant reversibility (⩾200 ml and ⩾15% over the baseline value) of FEV1categorised by the size of the response. Results are given for subjects who responded to salbutamol or ipratropium bromide alone (four subjects responded to both bronchodilators).
Another parameter used to assess bronchodilator reversibility is the VC, where a significant bronchodilator response is defined as an increase of at least 330 ml.12 We found such a response in VC in two patients (15%) with a normal FEV1 and FEV1/VC ratio of <70%; in seven patients (39%) with mild impairment of FEV1, in 16 (46%) with moderate impairment and in 11 patients (52%) with severe impairment of FEV1. Overall, 14 (39%) of the 36 patients with a VC response did not show a significant change in FEV1 to the same bronchodilator.
Static lung volumes
Static lung volumes and gas diffusion were measured in 107 patients and the results are summarised in table 3.
Static lung volumes and gas diffusion for 107 patients separated by degree of impairment of FEV1
The residual volume was significantly increased, both as an absolute value and when expressed as a percentage of the predicted value, as the severity of FEV1 impairment increased. This was associated with an increase in the RV/TLC ratio indicating increasing air trapping. The carbon monoxide transfer factor (Tlco) was significantly reduced only in the group with severely impaired FEV1 (difference in means 2.16 mmol/min/kPa (95% CI 0.96 to 3.37, p = 0.0004) compared with those in whom there was no impairment of the FEV1) whereas the transfer coefficient (Kco) was reduced in both those with moderate and severe impairment of FEV1 (difference in the means 0.31 mmol/min/kPa/l (95% CI 0.06 to 0.56, p = 0.0073) and 0.34 mmol/min/kPa/l (95% CI 0.079 to 0.61, p = 0.0061), respectively, compared with patients with mildly impaired FEV1).
HRCT SCANNING
Normal parenchymal appearances were reported for 39 (35%) scans and 17 (15%) scans had evidence of both emphysema and bronchiectasis.
Emphysema
Emphysematous change was identified on 56 (51%) high resolution CT scans which was confined to the upper lobes in 41 (73%). It was extensive, affecting the lower lobes and, in some instances, the middle lobe and lingula in 15 patients (27%). Patients with radiological evidence of emphysema had a significantly higher consumption of cigarettes than those without (median pack years 51 (IQR 30–79) and 35 (IQR 17–62), respectively, p<0.05).
Bronchiectasis
Bronchiectasis was noted on 32 (29%) high resolution CT scans and typical examples are shown in fig 2. Among the patients with bronchiectasis the disease was cystic in five patients (15.5%), varicose in four (12.5%), and tubular in 23 patients (72%). Twenty six of these 32 patients had a history of smoking but all the lifelong non-smokers (n = 6) had bronchiectasis which was tubular in five (table4).

Representative scans of (A) tubular, (B) varicose, and (C) cystic bronchiectasis with the abnormal areas arrowed.
HRCT appearances in 108 patients separated by degree of impairment of FEV1
Pulmonary nodules
Unsuspected pulmonary nodules were seen on nine (8%) scans. A biopsy sample was taken from one and was found to be a resectable adenocarcinoma, and one patient was diagnosed with mediastinal small cell lung cancer six months after the initial scan although the nodule remained unchanged. Five of the patients have had repeat scans which have shown no change over 6–18 months; in one patient the nodule was no longer visible on the repeat scan and the remaining patient declined a further scan.
RELATIONSHIP BETWEEN LUNG FUNCTION AND HRCT SCANNING
Both lung function tests and CT scans were normal in only 10 patients (9%). The proportion of patients with a normal scan was similar in the groups of patients categorised by degree of FEV1 impairment . Similarly the proportion of patients with emphysema or bronchiectasis did not differ significantly between the four groups.
Patients with extensive emphysema had more severe impairment in both FEV1 and gas transfer than patients with limited emphysema (table 5). Patients with varicose or cystic bronchiectasis were also found to have severe impairment of FEV1 and this was greater than in patients with tubular disease (table5).
Lung function for patients with radiological evidence of emphysema or bronchiectasis
SPUTUM COLOUR IN THE STABLE STATE AND BRONCHIECTASIS
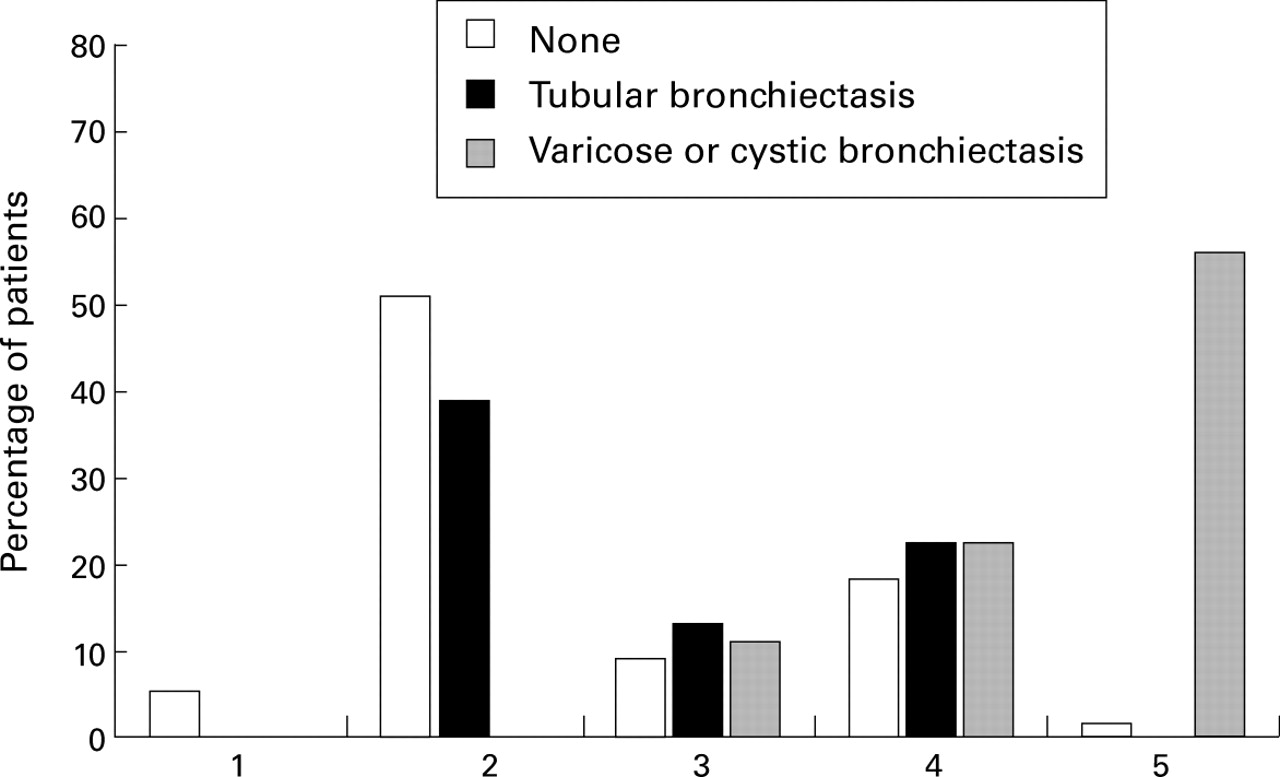
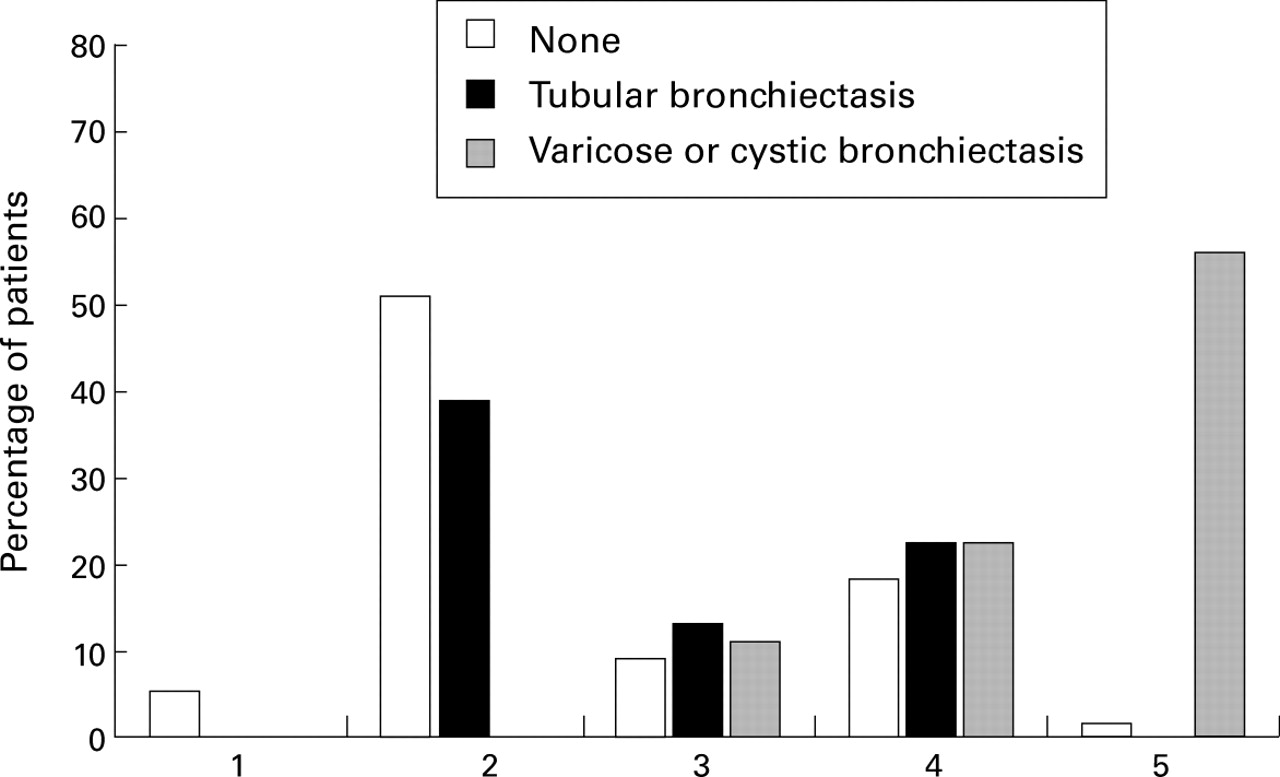
Ninety one patients (83%) provided a spontaneously expectorated sputum sample. Of the remaining 19 patients who were unable to expectorate sputum on the day of the assessment, six had radiological evidence of tubular and one had evidence of varicose bronchiectasis. Sputum colour for the patients with and without radiological evidence of bronchiectasis is shown in fig 3. The patients with bronchiectasis had a higher sputum number in the stable clinical state than the non-bronchiectatic group (p = 0.0006) although the range was wide (median number for bronchiectasis 3 (IQR 2–4) compared with 2 (IQR 2–3) for those without bronchiectasis). Mucopurulent sputum, assigned the number 5, occurred significantly more frequently in the patients with cystic and varicose bronchiectasis than in the patients with tubular bronchiectasis (p = 0.0011, Fisher's exact test). Indeed, when these patients were excluded, the distribution of sputum colour was similar for patients with or without tubular bronchiectasis (fig 3).
{kind=link}
{kind=link}
{kind=link}
Number of patients with sputum colour in each of the number categories. The patients are divided into those with no bronchiectasis, those with tubular bronchiectasis, and those with varicose or cystic bronchiectasis.
Discussion
This paper describes the physiological and radiological features of patients in primary care who were diagnosed as having COPD by their general practitioner. Formal lung function testing indicated that the FEV1 was in the normal range in 30% of the patients, suggesting that COPD is overdiagnosed in primary care if the BTS criteria for the diagnosis are applied, since these are based on the degree of impairment of FEV1 alone. However, among the patients with a normal FEV1, 41% had evidence of airflow obstruction with an FEV1/VC ratio of <70% which indicates that airflow obstruction was present in many of the patients with an FEV1 in the “normal” range and demonstrates the value of measuring the vital capacity when assessing patients with COPD. In the remaining patients in whom the FEV1 was reduced a range of impairment was found with 18% having mild, 33% moderate, and 19% severe impairment.
The national guidelines suggest that patients with mild disease are pre-symptomatic within the community.3 It would be predicted therefore that the patients studied here who presented to their general practitioner with an acute exacerbation of COPD would have moderate or severe disease. However, since 48% of the study patients had mild or no impairment of the FEV1, it appears that these patients require the use of health care resources more often than expected.
Our study may have overestimated the proportion of patients with mild and moderate disease in the community since we did not include patients who were thought to require treatment with oral corticosteroids or hospital admission. Two studies from Europe support the supposition that such patients may have had more severe disease. In a retrospective analysis of pre-discharge spirometric tests in 112 patients admitted to hospital with an infective exacerbation of COPD, 73% had an FEV1 of less than 50% of the predicted value.16 In addition, a recent study from Spain found that general practitioners prescribed oral corticosteroids in 43% of exacerbations in patients with predominantly moderate and severe COPD.17 However, there is no similar published information on the proportion of patients with acute exacerbations treated with oral corticosteroids in primary care in the UK. Overall, the proportion of patients with mild disease presenting to their general practitioner with an exacerbation is probably smaller than we have found. Nevertheless, the results described here still indicate that such patients do present themselves to the health care sector and clearly this would be an important group to identify and in whom to instigate preventative measures such as smoking cessation.
The determination of bronchodilator reversibility is important to establish the best achievable value for the FEV1, to direct treatment, and to identify patients with a large increase who are predominantly asthmatic. In addition, the post-bronchodilator FEV1 has been shown to relate more closely to survival than the pre-bronchodilator value.18 ,19 In our study group 72% of patients had a post-bronchodilator FEV1 of >60% of the predicted value, which implies a relatively good prognosis in the majority. However, most of our patients were elderly and survival has been shown to be worse in patients over the age of 65.19
In guidelines on the management of COPD various criteria are proposed to define a significant bronchodilator response and there is no agreement on the degree of response that indicates an underlying diagnosis of asthma.3 ,4 ,7 The summary of the national guidelines, which was sent to general practitioners, suggests that a substantial increase in the FEV1 of >500 ml may indicate an underlying diagnosis of asthma. Only five patients studied here showed such a response, suggesting that few asthmatics are mistakenly diagnosed as having COPD. However, this low incidence of asthmatic response could reflect the development of fixed airflow obstruction in previous asthmatic subjects with time, as most of the patients were elderly.
There is a consensus that patients with COPD can have a limited degree of bronchodilator reversibility and this was confirmed in the current study. A significant increase in the FEV1 (>200 ml) was found in just under half of the patients which is higher than the 36% reported previously by Nisar et al.20
The patients in our study with reversibility had a range of FEV1 responses to bronchodilators and more improved following a β2 agonist than with an anticholinergic agent, which is generally regarded as the bronchodilator of choice in COPD. The latter finding is probably explained by the sequence in which we administered the bronchodilators and it is likely that a higher proportion of patients would have shown a response to the anticholinergic agent if it had been administered alone. Nevertheless, our findings suggest that β2 agonists have a useful role in the treatment of airflow limitation in COPD.
Two recent studies have shown that bronchodilators reduce pulmonary hyperinflation even in the absence of a significant change in FEV1, and that measurements of reduced pulmonary hyperinflation are better predictors of therapeutic benefit.21 ,22 The value of assessing changes in parameters which indirectly measure reduced air trapping is shown by the fact that, in our study, 39% of the patients in whom the VC had increased significantly in response to bronchodilators did not have a significant increase in the FEV1.
An important finding of our study was the high prevalence of radiological bronchiectasis among patients diagnosed with COPD. CT scanning with a high resolution algorithm is now the investigation of choice to confirm a diagnosis of bronchiectasis13 and, using generally accepted criteria,13 ,14 we found that almost one third of the patients had bronchiectasis. It is likely that bronchiectasis is generally underdiagnosed, particularly in smokers where cough and sputum production are assumed to be due to cigarette smoke and COPD.23 In secondary care Currieet al found an incidence of bronchiectasis of 70% by bronchography and Smith et alreported an incidence of 68% by HRCT scanning.24 ,25However, both of these studies were based on patients referred for investigation of cough and sputum production and most were non-smokers, which may explain the high incidence.
In our study most of the patients with bronchiectasis were smokers and were clinically indistinguishable from the group as a whole. Smithet al 25 suggested that production of purulent sputum in the stable clinical state was highly suggestive of bronchiectasis. Our study supports this observation in cystic and varicose bronchiectasis which was a feature of most patients (83%) with sputum production classified as colour number 5. However, patients with tubular bronchiectasis could not be differentiated on clinical grounds or by sputum characteristics and thus may represent a different aetiological and clinical type of bronchiectasis from that recognised by traditional methods. Clearly, further studies are required to determine morbidity and prognosis in this radiological subgroup.
HRCT scanning is also sensitive and accurate in the diagnosis of emphysema26 and we found that half of the patients had radiological evidence of emphysema which was related to heavier cigarette smoking, as has been reported by others.27 ,28In the present study we made no attempt to quantify the degree of emphysema but, when present, it was usually confined to the upper lobes. In this group there was no relationship with the degree of FEV1 impairment and 75% had a Tlco in the normal range. In contrast, the 15 patients with emphysema involving the lower lobes showed more severe impairment of FEV1 and Tlco which is consistent with the study by Gurneyet al 27 who suggested that extensive emphysematous destruction of the upper lobe could occur before lung function was impaired.
Nine percent of our scans showed the presence of an unexpected pulmonary nodule. So far (two years later) only two patients have had a firm diagnosis of carcinoma made and one has proved resectable. The remaining nodules remain unchanged which suggests they are benign; however, this view has been challenged29 and the patients continue to be under review as they remain at increased risk from malignancy due to smoking. The relatively high rate of detection of nodules has implications for both the patients and health care providers and further studies are indicated to determine the cost effectiveness of HRCT scanning in screening and management of patients with COPD.
In conclusion, our study confirms that COPD in primary care is a heterogeneous disease. One third of patients with this diagnosis do not fulfil the proposed criteria3 (which emphasises the need for spirometric measurements of a high standard) and the remainder have a wide range of lung function impairment. Bronchiectasis is present in a significant proportion of patients although the implications of this finding remain unknown. However, the results of our study suggest that more careful characterisation of COPD patients in primary care is required to determine the applicability of current therapeutic guidelines and when drawing conclusions from clinical trials conducted in this population.
Acknowledgments
We thank all general practitioners for referring their patients for participation in this study. We also thank Mrs B Leung, Mrs K Verbeet and Mrs M Henson for their involvement in the recruitment and care of the patients.
References
Footnotes
Funding: This study was funded by an unrestricted educational grant from GlaxoWellcome.