Article Text

Abstract
BACKGROUND Sputum eosinophil counts and exhaled nitric oxide (NO) levels are increased in asthma and both measurements fall in response to corticosteroids.
METHODS Exhaled NO levels and sputum eosinophil counts were assessed as non-invasive markers of the response to an oral steroid in 37 patients (19 women) with stable chronic asthma (mean (SD) age 48.6 (12.2) years, asthma duration 25.9 (17.3) years, and baseline forced expiratory volume in one second (FEV1) 76.3 (21.9)% predicted). Spirometric tests, with reversibility to a β agonist (2.5 mg nebulised salbutamol), and induced sputum (using nebulised 3% saline) were performed at recruitment and following treatment with 30 mg prednisolone/day for 14 days.
RESULTS Baseline NO levels correlated with the percentage improvement in FEV1from baseline to the post-steroid, post-bronchodilator value (r s = 0.47, p = 0.003), with an NO level of >10 ppb at baseline having a positive predictive value of 83% for an improvement in FEV1 of ⩾15% (sensitivity 59%, specificity 90%). Sputum eosinophilia (⩾4%) had a positive predictive value of 68% (sensitivity 54%, specificity 76%) for an increase in FEV1 of ⩾15%. A combination of sputum eosinophilia and increased NO levels resulted in a positive predictive value of 72% and a negative predictive value of 79% (sensitivity 76%, specificity 75%).
CONCLUSION Exhaled NO levels and sputum eosinophilia may be useful in predicting the response to a trial of oral steroid in asthma.
- airway inflammation
- nitric oxide
- induced sputum eosinophilia
- asthma
- corticosteroids
Statistics from Altmetric.com
Asthma is characterised by episodic reversible airway narrowing with associated bronchial hyperreactivity and the involvement of inflammation is well recognised, even in mild disease. The aim of treatment is to control symptoms and to optimise lung function, with inhaled steroids being central to the management through their effect on airway inflammation. The “gold standard” for assessing reversibility of lung function would be a trial of steroid treatment (oral prednisolone for two weeks) but this may be inappropriate in some individuals because of coexistent disease, or declined by others for various reasons. In addition, a two week steroid trial with lung function testing before and after treatment is time consuming, so a predictor of steroid response would have clinical application.
Both induced sputum eosinophil counts and exhaled NO concentrations have been used as non-invasive markers of asthmatic airway inflammation.1-4 They therefore appear appropriate for this study, the aim of which was to assess the potential of non-invasive markers of airway inflammation in predicting response to an oral steroid trial in asthma.
Methods
PATIENTS
The study was prospective, recruiting patients through the respiratory outpatient clinic and community contacts. All had a diagnosis of asthma, according to the criteria established by the American Thoracic Society, for at least five years and had had no acute exacerbation within the preceding month. All were non-smokers or, if ex-smokers, had stopped at least five years earlier and had smoked a maximum of 10 pack years. The study was approved by the West ethics committee, Western Infirmary, Glasgow. All volunteers gave informed consent.
STUDY DESIGN
The study involved two visits separated by a two week course of oral prednisolone at a dose of 30 mg/day. Each visit involved spirometric tests (Vitalograph Ltd, Buckingham, UK), reversibility to 2.5 mg nebulised salbutamol, measurement of exhaled nitric oxide concentrations, and induced sputum. On a third visit a histamine inhalational challenge was performed.
MEASUREMENTS
Exhaled nitric oxide
Exhaled nitric oxide measurements were performed using a Logan Research analyser (Logan Research Ltd, Rochester, Kent, UK) operating on the principle of chemiluminescence. The technique used is that recommended by the European Respiratory Society Task Force.5 An increased concentration of exhaled NO was defined as ⩾10 ppb on the basis of our own experience and other work.5
Sputum induction
Sputum induction was performed following assessment of reversibility to salbutamol using a modification of the method described by Pin et al.1 The sample was collected in a sterile container and transferred to the laboratory on ice as quickly as possible, and in all cases in less than two hours.
All samples were processed without the laboratory staff being aware of the clinical information relating to the individual subject, and the procedure followed was similar to that described by Popovet al.6 Sputum eosinophilia was defined as ⩾4% eosinophils, consistent with previous work.7
Histamine inhalational challenge
Bronchial hyperresponsiveness to histamine was established using doubling doses of inhaled histamine from 0.0625 to 16 mg/ml.8 The test was performed within a few days of completion of the steroid trial.
STATISTICAL ANALYSIS
Descriptive statistics were summarised as mean, median, and standard deviation. A clinically significant improvement in best forced expiratory volume in one second (FEV1) following the steroid trial and bronchodilator was defined as a ⩾15% increase as a percentage of the baseline value. Correlations between exhaled NO concentrations, sputum eosinophilia, and increase in FEV1were assessed using Spearman rank correlation coefficients. Ranked correlations were also assessed between NO, eosinophilia, and bronchial hyperresponsiveness (logPC20). The predictive values for each test were determined using 2 × 2 contingency tables, permitting calculation of positive and negative predictive values, and sensitivity and specificity.
Results
Thirty seven asthmatic subjects (19 women) of mean (SD) age 48.6 (12.2) years, asthma duration 25.9 (17.3) years, and baseline FEV1 76.3 (21.9)% predicted were recruited into the study. All but one was taking inhaled steroids with a median dose equivalent to 800 μg beclomethasone (interquartile range 400–1000 μg).
Despite being on inhaled steroids, 12 of the patients (32%) had an increased level of NO. Of the 30 patients producing sufficient sputum for analysis, 11 (37%) had sputum eosinophilia. There was no significant correlation between the inhaled steroid dose and baseline exhaled NO levels (r s = –0.21, p = 0.22) or between the inhaled steroid dose and baseline sputum eosinophil count (r s = 0.17, p = 0.36). After treatment with oral steroids there was a statistically significant correlation between baseline NO levels and percentage change in FEV1 (r s = 0.47, p = 0.003), but the scatter was such that the change in FEV1 could not be predicted by baseline NO alone. No correlation was seen between baseline sputum eosinophil count and improvement in FEV1(r s = 0.19, p = 0.30).
Of those patients with an increased NO level at baseline, 83% developed an increase in FEV1 of ⩾15% after oral steroids (positive predictive value of 83%, table 1). For sputum eosinophilia the positive predictive value was 64% but the sensitivity of these tests was low at 59% and 54%, respectively. We combined the tests, dividing the group on the basis of having one or other marker increased or neither marker increased. The resulting positive predictive value was 72% with an improved sensitivity of 76%. The negative predictive value was 79% (specificity 75%) such that, of those subjects with a normal exhaled NO level and sputum eosinophilia of <4%, 79% had an improvement in FEV1 of <15%.
Value of exhaled nitric oxide, sputum eosinophilia or a combination in predicting steroid response
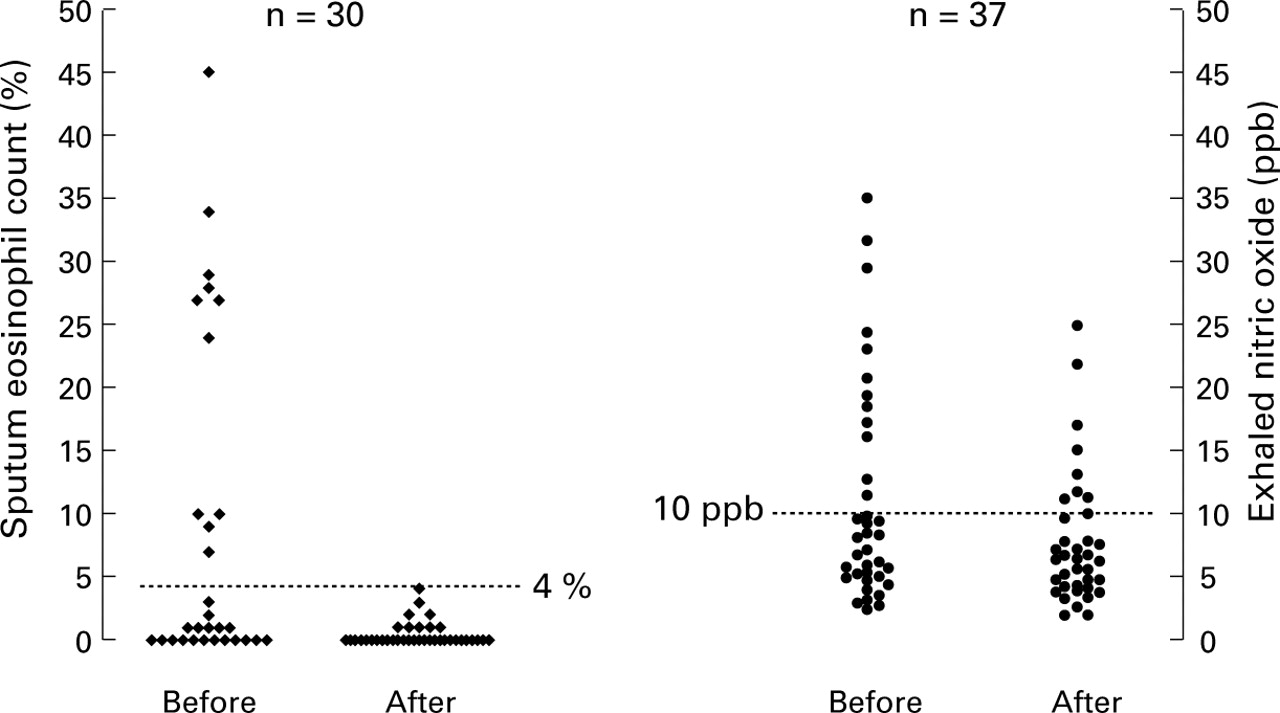
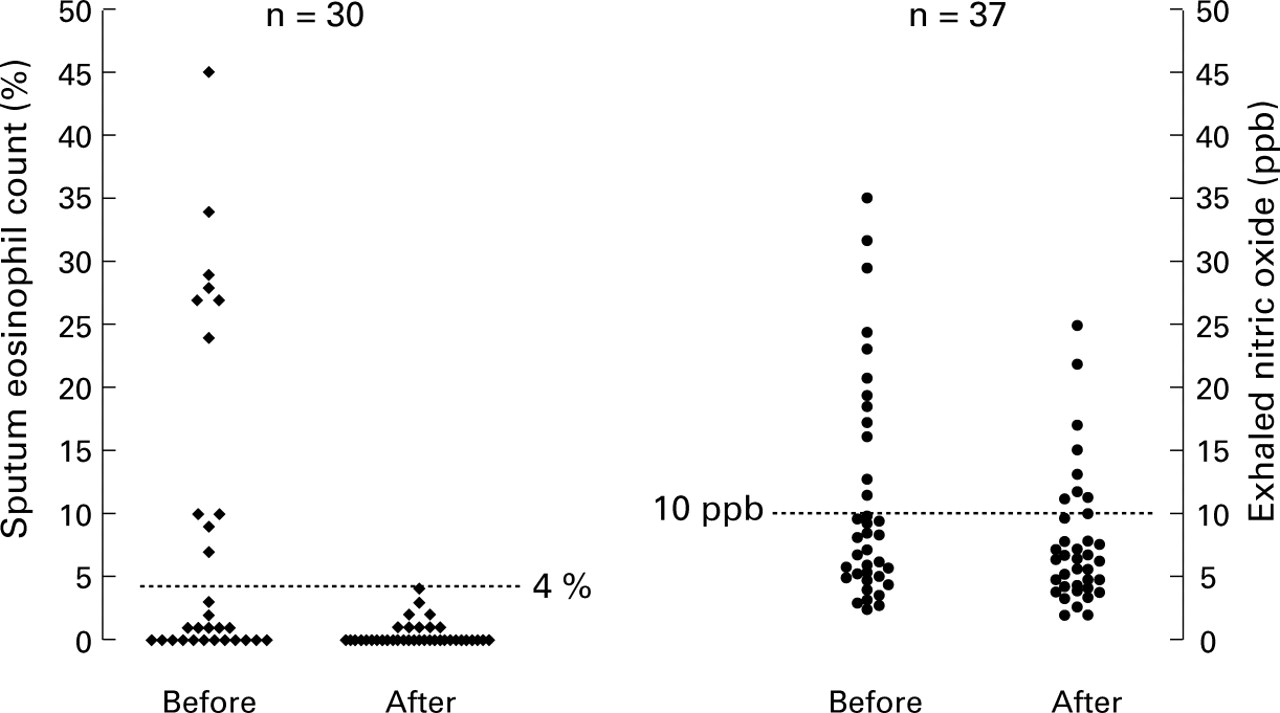
Following a trial of steroid therapy sputum eosinophilia essentially resolved but, although exhaled NO levels fell, they did not return to a normal level in all subjects (fig 1). Finally, ranked correlations were performed between NO and logPC20 and between eosinophil count and logPC20 but neither reached statistical significance (p = 0.11 and p = 0.33, respectively).
{kind=link}
Induced sputum eosinophil count and exhaled nitric oxide levels before and after the steroid trial.
Discussion
We have shown that, in a group of chronic asthmatic subjects who had not experienced a recent exacerbation, a significant proportion had raised levels of exhaled NO and sputum eosinophilia. Our results show that exhaled NO levels and sputum eosinophilia can be used to predict a response in lung function following an oral steroid trial, with a combination of these two markers producing significantly improved sensitivity and specificity. Of potential clinical applicability is the negative predictive value of this combination, with 79% of those without increased NO levels or significant sputum eosinophilia having an improvement in FEV1 of <15%.
The markers used for this study are acceptable for patients and reproducible, although both have limitations and neither alone produced a clinically acceptable positive predictive value. Induced sputum is a useful technique for studying the effects of asthma treatment on airway eosinophilic inflammation, but not all patients are able to produce a sample sufficient for analysis. Although airway inflammation is present in newly diagnosed and mild asthmatics, exacerbations may not be associated with sputum eosinophilia7 and there is evidence for the role of other inflammatory cells in asthmatic airway inflammation, particularly in patients with irreversible airflow obstruction.9 Asthmatic airway inflammation may therefore be a heterogeneous process of which sputum eosinophilia is only one part, and it may be that sputum eosinophilia and exhaled NO levels reflect different components of the inflammatory process. The improvement in sensitivity and specificity within this study using the combination of the two markers would be in keeping with this.
Nitric oxide is a non-specific marker of airway inflammation, being increased in conditions other than asthma—for example, bronchiectasis and cystic fibrosis. Patients with asthma have higher levels of NO than normal individuals,3 which relate to airway inflammation, and treatment with steroids produces a reduction in these levels.4 However, the range of NO levels in asthmatic patients is large with some having normal values and others having increased levels despite treatment with inhaled steroids. Whilst the latter may suggest insufficient treatment, the NO measurements following steroid treatment in this study are interesting because they show that, although levels fall, they do not return to normal in all patients despite oral steroid treatment. A dose dependent effect seems unlikely, given that all patients received a two week course of oral steroid, and the mechanism for the persistent increase in NO is unclear.
Assuming that uncontrolled inflammation results in airway remodelling,10 treatment should be aimed at controlling that process and in maximising lung function. The two markers employed in this study, although not ideal, provide some predictive value of improvement in lung function in a broad spectrum of asthmatic subjects, and suggest the potential use of such markers in predicting best lung function and hence identifying those patients in whom an increase in dose of inhaled corticosteroid may be beneficial. Addition of further markers might increase the predictive values but reduce clinical applicability.
References
Footnotes
Funding: National Asthma Campaign.