Article Text

Abstract
BACKGROUND Cystic fibrosis is characterised by oxidative stress in the airways. Isoprostanes are prostaglandin isomers formed by free radical catalysed peroxidation of arachidonic acid. 8-Isoprostane is increased in interstitial lung diseases, asthma, chronic obstructive pulmonary disease, and adult respiratory distress syndrome. Exhaled nitric oxide (NO) and carbon monoxide (CO) are biomarkers of inflammation and oxidative stress in the airways, respectively.
METHODS Concentrations of 8-isoprostane in the breath condensate of 10 normal subjects and 19 patients with stable cystic fibrosis were measured using an enzyme immunoassay (EIA). Breath condensate is a non-invasive method of collecting airway secretions. Exhaled nitric oxide (NO) and carbon monoxide (CO) levels were measured by a chemiluminescence analyser.
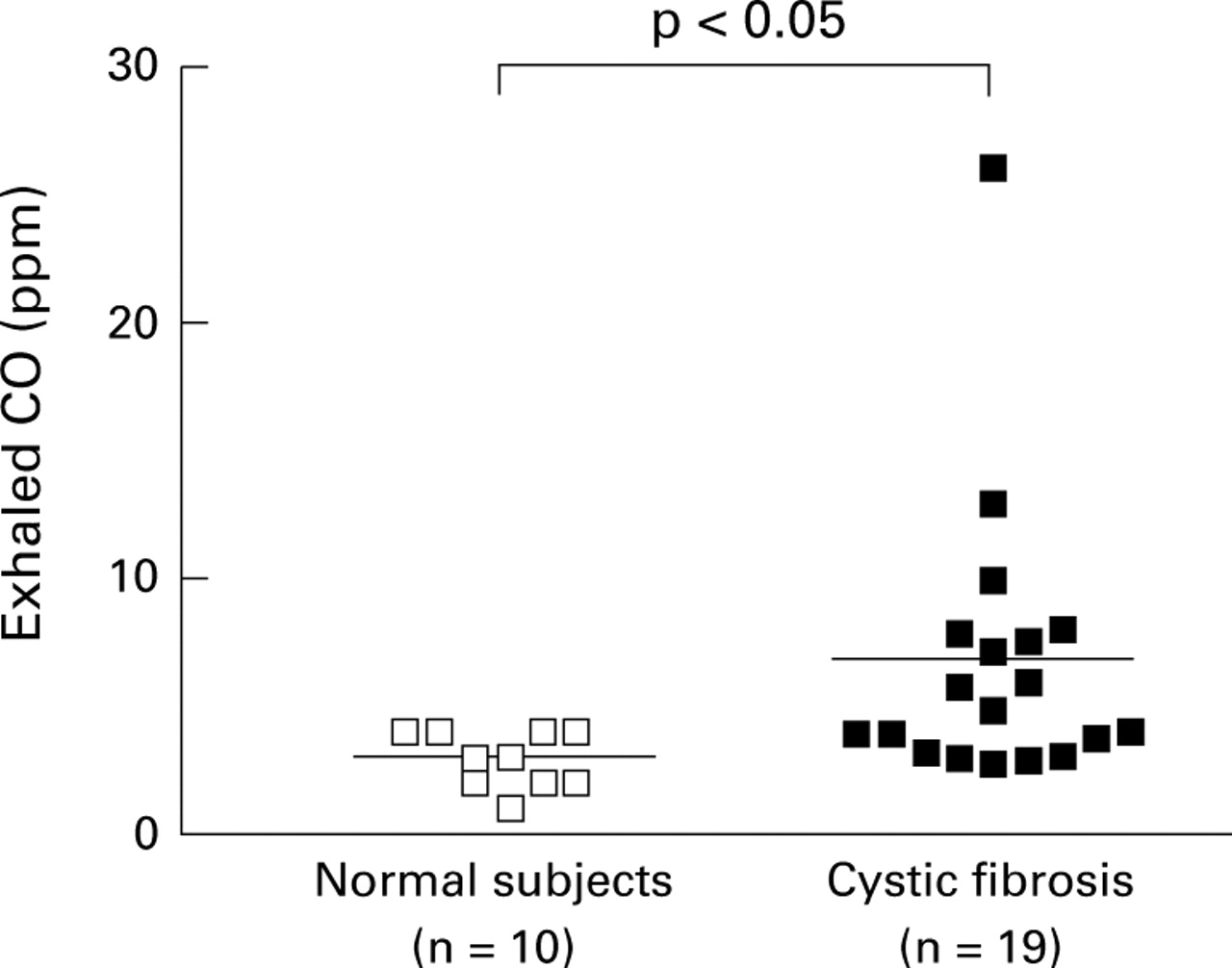
RESULTS Concentrations of 8-isoprostane in the breath condensate of patients with stable cystic fibrosis were increased about threefold compared with normal subjects (42.7 (4.5) pg/ml vs 15.2 (1.7) pg/ml; p<0.005, 95% CI 14.6 to 40.9). 8-Isoprostane concentrations were negatively correlated with forced expiratory volume in one second in patients with cystic fibrosis (r = −0.61; p<0.005). Exhaled CO was also increased in patients with cystic fibrosis compared with normal subjects (6.7 (1.2) ppm vs 2.9 (0.3) ppm; p<0.05, 95% CI 0.2 to 7.4). 8-Isoprostane concentrations were significantly correlated with CO levels (r = 0.66; p<0.002).
CONCLUSIONS The results of this study show that oxidative stress is increased in cystic fibrosis and may be quantified by measuring 8-isoprostane concentrations in breath condensate.
- cystic fibrosis
- 8-isoprostane
- oxidative stress
Statistics from Altmetric.com
Patients with cystic fibrosis have increased oxidative stress and a reduced antioxidant capacity.1 ,2 The frequent bronchopulmonary infections that are characteristic of cystic fibrosis activate and increase the numbers of neutrophils recovered from lungs of patients with cystic fibrosis.3 Activated neutrophils are the major source of free radicals.4 Biomarkers of oxidative stress are increased in plasma,5 bronchoalveolar lavage (BAL) fluid,6 and sputum of patients with cystic fibrosis,7 supporting a pathophysiological role for free radicals in this disease. Definitive evidence for this role has been hampered by the limitations of currently available methods to measure oxidative stress in vivo.8
Isoprostanes have recently been used to quantify oxidative stress in vivo. Measurements of these compounds in biological fluids may provide a quantitative index of oxidant stress in vivo.8Isoprostanes are free radical catalysed products of arachidonic acid formed in situ in the cell membrane phospholipids, from which they are cleaved by phospholipase A2.9 ,10 Due to their stability, specificity for lipid peroxidation, in vivo production, and relative abundance in biological fluids, the isoprostanes are among the most reliable biomarkers of lipid peroxidation and oxidative stress.8 8-Isoprostane, a member of the F2 isoprostane class, has been detected in plasma and urine in humans and its levels are increased in pathophysiological conditions in which oxidative stress is increased, such as cigarette smoking and scleroderma.10-13 We have found increased concentrations of 8-isoprostane in the BAL fluid of patients with interstitial lung diseases.14 8-Isoprostane concentrations are also increased in the urine of patients with chronic obstructive pulmonary disease (COPD) and in exhaled breath condensate in patients with adult respiratory distress syndrome (ARDS) and asthma.15-17Recently, increased 8-isoprostane concentrations were reported in the plasma of patients with cystic fibrosis.18
In this study we have compared 8-isoprostane concentrations in the breath condensate of patients with stable cystic fibrosis with those in normal subjects. Breath condensate is a non-invasive method of collecting airway secretions.19 The aim of this study was to provide a non-invasive approach to direct measurement of oxidant stress in the lungs of patients with cystic fibrosis.
Methods
PATIENTS
Ten healthy subjects and 19 patients with stable cystic fibrosis were included in the study (table 1). Patients with cystic fibrosis were attending an outpatient clinic at the Royal Brompton Hospital in London for a regular (six monthly) check up and did not present with chest infections or any other specific problems. The study groups were matched for age. All study subjects were screened for active smoking by measuring urinary conitine levels (data not shown) and none was found to smoke. Patients with cystic fibrosis had typical clinical features of the disease, including a positive sweat chloride test, and all were chronically infected with Pseudomonas aeruginosa. Patients infected withBurkholderia cepacia were excluded from the study. Five patients were being treated with inhaled glucocorticoids (beclometasone dipropionate 0.8–2 mg/day, budesonide 2 mg/day, fluticasone 1 mg/day) and five patients were taking oral glucocorticoids (prednisolone 4–15 mg/day). Patients treated with oral steroids had poorer lung function (mean (SE) forced expiratory volume in one second (FEV1) 28.9 (3.5)% predicted) than patients treated with inhaled steroids (FEV1 45.7 (5.0)% predicted) or steroid naive patients (FEV1 60.9 (3.3)% predicted). One patient treated with inhaled steroids and two treated with oral steroids had allergic bronchopulmonary aspergillosis. Two other patients had arthritis. None of the steroid naive patients had allergic bronchopulmonary aspergillosis or arthritis. Treatment accepted for the study consisted of antibiotics (flucoxacillin, colomycin, gentamicin, tobramycin) and bronchodilators (β2 adrenergic drugs, anticholinergics). Five patients were taking DNAse (Dornase alfa) 2.5 mg/day. No patient was receiving ibuprofen or macrolides.
Patient characteristics
Informed consent was obtained from all subjects and the study was approved by the ethics committee of the Royal Brompton Hospital and Harefield Trust.
PULMONARY FUNCTION
Pulmonary function tests were performed on the same day as the measurement of NO and CO. FEV1 and forced vital capacity (FVC) were measured using a dry spirometer (Vitalograph Ltd, Buckingham, UK) and the best value of the three manoeuvres was expressed as a percentage of the predicted value.
8-Isoprostane was measured within two weeks of the breath condensate sample collection.
MEASUREMENT OF EXHALED 8-ISOPROSTANE
Breath condensate samples were collected using a specially designed glass condensing chamber. The condensing chamber contained a double wall glass and the inner side of the glass was cooled by ice. Breath condensate was collected between the two glass surfaces. Exhaled air entered and left the chamber through one-way valves at the inlet and at the outlet, keeping the chamber closed. After rinsing their mouths, subjects breathed tidally through a mouthpiece connected to the condenser for 15 minutes while wearing noseclips. Approximately 1 ml of condensate was stored at –70°C in a 2 ml sterile plastic tube.19
8-Isoprostane concentrations in breath condensate were measured by a specific enzyme immunoassay (EIA) kit (Cayman Chemical, Ann Arbor, Michigan, USA). Samples were collected and stored at –70°C until assayed. The assay has been validated to obtain a high correlation (0.95) between added known amounts of 8-isoprostane and the concentration measured by EIA. This assay was directly validated by gas chromatography/mass spectrometry. The antiserum used in this assay has a 100% cross reactivity with 8-isoprostane, 0.2% each with prostaglandins PGF2α, PGF3α, PGE1 and PGE2, and 0.1% each with 6-keto-PGF1α. The detection limit of the assay is 4 pg/ml. The kit has been used to measure 8-isoprostane concentrations in breath condensate and in BAL fluid.15 ,18
The possible influence of the ventilation rate on 8-isoprostane concentrations in breath condensate was assessed. Normal volunteers breathed at 14 and 28 breaths/min for 15 minutes keeping the same tidal volume. There was no difference in the concentration of 8-isoprostane in the two samples collected from the same patient at the different ventilation rates (15.8 pg/ml and 12.5 pg/ml, n = 6).
The intra-assay and interassay coefficients of variation were 5% and 6%, respectively. Saliva contamination of breath condensate was ruled out by measuring amylase concentrations which were undetectable in six samples tested.
MEASUREMENT OF EXHALED NITRIC OXIDE
Exhaled NO was measured using a chemiluminescence analyser (model LR2000; Logan Research, Rochester, UK), sensitive to NO in concentrations from 1 to 5000 ppb (by volume) and with a resolution of 0.3 ppb, which was designed for online recording of exhaled NO concentrations as previously described.20 The analyser was calibrated using a certified NO mixture (436 ppb) in nitrogen (BOC Special Gases, Guildford, UK). Measurements of exhaled NO were made by slow exhalation (5–6 l/min) from total lung capacity for 20–30 seconds against a resistance (3 (0.4) mm Hg) to prevent nasal contamination.
MEASUREMENT OF EXHALED CARBON MONOXIDE
Exhaled CO was measured by an electrochemical CO monitor sensitive to CO from 0 to 500 ppm by volume, adapted for online recording of CO concentrations and integrated with the chemiluminescence analyser (LR2000, Logan Research, Rochester, UK) to control exhalation parameters. The subjects exhaled slowly from functional vital capacity with a constant flow (5–6 l/min) against a resistance (3 (0.4) mm Hg) over 20–30 seconds into the analyser. Two successive recordings were made and mean values were used in all calculations. Ambient CO levels were recorded before each measurement.
STATISTICAL ANALYSIS
For parametric data the Student's unpairedt test was used to compare groups. Linear regression analysis was used to assess the relationship between 8-isoprostane concentrations in breath condensate and exhaled gases or FEV1. All data were expressed as mean (SE) values and p values of <0.05 were considered significant.
Results
The clinical data of the healthy subjects and patients with cystic fibrosis are summarised in table 1. 8-Isoprostane was measurable in breath condensate of healthy subjects (15.2 (1.7) pg/ml) and was increased 2.8-fold in patients with cystic fibrosis (42.7 (4.5) pg/ml; p<0.005, 95% CI 14.6 to 40.9; fig 1). Concentrations of 8-isoprostane in breath condensate were similar in untreated patients (37.7 (6.4) pg/ml, n = 9) and those treated with inhaled (45.1 (11.8) pg/ml, n = 5; p = 0.56) or oral steroids (49.4 (6.1) pg/ml, n = 5; p = 0.26). We also measured exhaled NO and CO in the same study groups as biomarkers of airway inflammation and oxidative stress, respectively. NO was significantly decreased in patients with cystic fibrosis compared with healthy subjects (6.5 (0.6) ppb vs 4.4 (0.6) ppb, 95% CI –3.9 to –0.2, p<0.03; fig 2) whereas exhaled CO was increased in the patients with cystic fibrosis (2.9 (0.3) ppm vs 6.7 (1.2) ppm, p<0.05; fig 3). NO levels were similar in steroid naive patients (4.3 (0.7) ppb, n = 9) and in patients treated with inhaled (4.9 (0.9) ppb, n = 5, p = 0.83) or oral steroids (3.7 (1.1) ppb, n = 5, p = 0.57). There was no difference in CO levels between untreated patients (5.3 (1.1) ppm, n = 9) and those treated with inhaled (10.3 (4.0) ppm, n = 5, p = 0.15) or oral steroids (5.5 (1.4) ppm, n = 5, p = 0.90). The concentration of 8-isoprostane in breath condensate was negatively correlated with FEV1(r = –0.61; p<0.005, fig 4A) and positively correlated with exhaled CO levels (r = 0.66; p<0.002, fig 4B) in patients with cystic fibrosis. No correlation was found between age, sex, FVC, or exhaled NO levels and the concentration of 8-isoprostane in breath condensate (data not shown).

Concentrations of 8-isoprostane in breath condensate of normal subjects and patients with cystic fibrosis. The horizontal bars indicate mean levels.

Concentrations of nitric oxide (NO) in exhaled air of normal subjects and patients with cystic fibrosis. The horizontal bars indicate mean levels.

Concentrations of carbon monoxide (CO) in exhaled air of normal subjects and patients with cystic fibrosis. The horizontal bars indicate mean levels.

{kind=link}
{kind=link}
{kind=link}
{kind=link}
(A) Correlation between 8-isoprostane concentrations in breath condensate and forced expiratory volume in one second (FEV1) in patients with cystic fibrosis (r = –0.61; p<0.005). (B) Correlation between 8-isoprostane concentrations in breath condensate and carbon monoxide in exhaled air in patients with cystic fibrosis (r = 0.66; p<0.002).
Discussion
8-Isoprostane, the most well characterised compound belonging to the F2-isoprostanes, a group of prostaglandin F2αstereoisomers, is formed in vivo by reactive oxygen species (ROS) peroxidation of arachidonic acid, independent of the action of cyclo-oxygenase.11 Although 8-isoprostane can be produced by cyclo-oxygenase-1 and/or cyclo-oxygenase-2 activity in some cells and tissues, both in vitro and in vivo,21-23 its production in vivo in humans is mainly derived from lipoperoxidation due to ROS.16 For this reason, measurement of 8-isoprostane levels in biological fluids has been considered an ideal method of quantifying oxidative stress in different pathophysiological conditions.9
In this study we have shown that 8-isoprostane is measurable in the breath condensate of normal subjects. The levels of 8-isoprostane in these subjects were similar to those found in the breath condensate by Montuschi et al 17 using gas chromatography/mass spectrometry. Patients with cystic fibrosis had 8-isoprostane levels 2.8-fold higher than normal subjects, indicating that oxidative stress, as reflected by 8-isoprostane concentrations in breath condensate, is increased in patients with cystic fibrosis. These results are in agreement with a recent study which reported increased plasma concentrations of 8-isoprostane in patients with cystic fibrosis.18 Measurement of 8-isoprostane in plasma reflects systemic oxidative stress, whereas measurement of 8-isoprostane in the exhaled breath condensate is more likely to reflect lipoperoxidation that occurs in the lungs. Although numbers are small, subgroup analysis suggests that there was no difference in 8-isoprostane levels between untreated patients with cystic fibrosis and those treated with steroids. However, sample size and lack of homogeneity prevent definite conclusions on the role of glucocorticoids in modulating 8-isoprostane concentrations in breath condensate. Larger numbers and homogeneous groups are needed to confirm or refute these preliminary findings. In contrast to other inflammatory airway diseases such as interstitial lung diseases and COPD,15 ,168-isoprostane levels in breath condensate were inversely correlated with FEV1 in patients with cystic fibrosis, suggesting that an increase in oxidant stress may lead to a deterioration of lung function.
Consistent with other studies,24 ,25 exhaled NO levels were lower and CO levels were higher in patients with cystic fibrosis than in normal subjects. The low exhaled NO values could be due to the trapping effect of the viscous airway secretions in these patients or to a scavenging effect on NO as a result of enhanced ROS formation.26 ,27 A deficiency in inducible NO synthase could also account for this finding.28 Unlike other respiratory diseases such as asthma in which exhaled NO reflects airway inflammation,29 low NO levels in patients with cystic fibrosis preclude the possibility of using it as a biomarker of inflammation in this disease. Exhaled CO, another biomarker of inflammation and oxidative stress, is increased more than twofold compared with normal subjects, further supporting a role for ROS in the pathophysiology of cystic fibrosis. The significant correlation between 8-isoprostane in breath condensate and exhaled CO indicates that these two biomarkers may have a similar biological significance in reflecting overproduction of ROS in cystic fibrosis. A similar increase in 8-isoprostane and CO levels was previously reported in patients with severe asthma.18 Considering the protective role of hemoxygenase activation, enhanced CO production could represent a mechanism to counteract the oxidative damage.30 Large controlled studies are required to establish the role of steroid treatment in modulating exhaled CO levels. Nothing is known about the possible role of 8-isoprostane as a mediator of oxidative stress in cystic fibrosis, although this compound may have a role in the pathophysiology of oxidant damage due to its biological actions.9
In conclusion, we have shown that lipid peroxidation and oxidative stress are increased in patients with cystic fibrosis, as reflected by increased 8-isoprostane concentrations in breath condensate. Measurement of 8-isoprostane by this non-invasive approach may provide the rational basis for dose finding studies of antioxidants and an important end point in clinical trials of these drugs in cystic fibrosis.
Acknowledgments
Dr Paolo Montuschi is recipient of Research Fellowship from the National Research Council of Italy.