Article Text

Abstract
BACKGROUND Exhaled levels of nitric oxide (NO) are raised in asthma but the relationship between exhaled NO levels and a direct measure of airway inflammation has not been investigated in asthmatic patients treated with inhaled steroids.
METHODS The relationship between exhaled NO levels, clinical measures of asthma control, and direct markers of airway inflammation were studied in patients with asthma treated with and without inhaled corticosteroids. Thirty two asthmatic patients (16 not using inhaled steroids and 16 using inhaled beclomethasone dipropionate, 400–1000 μg/day) were monitored with respect to measures of asthma control including lung function, symptom scores, medication usage, and variability of peak expiratory flow (PEF) for one month. Measurements of exhaled NO and fibreoptic bronchoscopy were performed at the end of the monitoring period. Bronchial mucosal biopsy specimens were stained with an anti-MBP antibody for quantification of eosinophils.
RESULTS There was no significant difference in lung function, symptom scores, or medication usage between the two groups, but there was a significant difference in PEF variability (8.7 (1.2)% in steroid naive patients versus 13.6 (1.9)% in steroid treated patients, p<0.05) and exhaled NO levels (9.9 (3.5) ppb in steroid naive patients versus 13.6 (2.0) ppb in steroid treated patients, p<0.05). There was no correlation between exhaled NO and mucosal eosinophils, or between NO and conventional measures of asthma control. There was a significant correlation between mucosal eosinophils and lung function (r = –0.43, p<0.05).
CONCLUSIONS Exhaled NO levels do not reflect airway mucosal eosinophilia and these markers reflect different aspects of airway inflammation. The clinical usefulness of exhaled NO needs to be determined in prospective longitudinal studies.
- nitric oxide
- asthma
- eosinophils
- airway inflammation
Statistics from Altmetric.com
Asthma is a chronic inflammatory disease of the airways and studies of bronchial mucosal biopsy specimens have shown the presence of a chronic inflammatory process with correlations between the degree of airflow obstruction as measured by forced expiratory volume in one second (FEV1) and the number of mucosal eosinophils. Asthma severity and control are usually measured in terms of symptoms, medication usage, and lung function such as peak expiratory flow (PEF). Monitoring the inflammatory process, determination of the severity of the disease, and requirements of anti-inflammatory therapy needed to optimise and control asthma may be important aspects of asthma management in the future. Currently the assessment of asthma and of its control is based on “conventional” measurements including reported symptom scores, medication usage, serial PEF monitoring, and measurements of FEV1. However, there are potential drawbacks with these conventional methods. Isolated measurements of FEV1 in the clinic do not reflect the chronology of asthma control, and PEF charting, though reflecting changes with time more accurately, is often not performed reliably.1 Furthermore, bronchodilator treatment may improve symptoms and lung function temporarily, while having no effect on the underlying inflammatory process. Methods of monitoring airway inflammation more directly have been developed in the hope that these may improve the long term management of asthma.
At present, bronchial biopsy specimens from proximal airways obtained through a fibreoptic bronchoscope are the most direct method of measuring airway inflammation and have been proposed as a “gold standard” against which other methods should be compared.2 Because of the difficulties associated with this invasive method there has been a growing interest in developing less invasive methods for monitoring inflammation such as measurements of nitric oxide (NO) in exhaled breath3 and of eosinophils in induced sputum.4 These methods have been validated, are well tolerated, and are reproducible, making them potential candidates for use in the clinical setting. We have previously found correlations between exhaled NO levels and other markers of inflammation in patients with mild asthma not using inhaled steroids.5 In the present study we have examined a group of patients with more severe asthma, including those using inhaled steroids, in order to examine whether exhaled NO levels can predict asthma severity and eosinophilic inflammation in the airways.
Methods
PATIENTS
Thirty two asthmatic subjects (table 1) who fulfilled the diagnostic criteria of asthma from the American Thoracic Society were recruited for the study.6 All were atopic, defined by positive skin prick tests to common allergens. Sixteen of the patients had mild asthma and were not previously or currently being treated with inhaled corticosteroids, and 16 stable but symptomatic patients were receiving treatment with inhaled steroids (400–1000 μg beclomethasone dipropionate (BDP)/day). All patients took inhaled salbutamol for intermittent relief of wheeze. None of the subjects studied had received oral corticosteroids during the preceding 12 months. Current smokers or ex-smokers of more than five pack years were excluded.
Patient demography and clinical physiological data
STUDY DESIGN
The study was a cross sectional study comparing the conventional indices of asthma control with other markers of inflammation—namely, exhaled levels of NO and eosinophil counts in bronchial biopsy specimens. Patients were asked to record their PEF twice daily and to chart their symptom scores (0–3) and rescue β2 agonist usage for four weeks. Symptom scores were defined as follows: 0 = none, 1 = mild (few symptoms not troublesome), 2 = moderate (symptoms troublesome), 3 = severe (not able to carry out normal duties). Lung function (FEV1) and exhaled NO levels were measured prior to fibreoptic bronchoscopy. The study was approved by the Royal Brompton Hospital ethics committee and all patients gave their informed consent.
LUNG FUNCTION TESTS
Baseline spirometric parameters were recorded from the best of three attempts using a dry wedge spirometer (Vitalograph, Buckingham, UK), with measurements not varying by more than 5% or 0.2 litres being acceptable. All patients abstained from using their inhaled β2 agonists and from caffeine-containing beverages for 12 hours before the test. PEF measurements were recorded by patients at home with a mini-Wright peak flow meter (Clement Clarke, Harlow, UK) and charted in a peak flow and symptom diary card.
NITRIC OXIDE MEASUREMENTS
Exhaled NO was measured using a chemiluminescence analyser before spirometry (Model LR2000, Logan Research, Rochester, UK) with a sensitivity from 1 ppb to 100 ppm NO, an accuracy of ±0.5 ppb, and a response time of <2 s to 90% of full scale. In addition, the analyser also measured carbon dioxide, expiration flow and pressure, and the exhaled volume in real time. The analyser was fitted with a biofeedback display unit to provide visual guidance for the subject to maintain the pressure and exhalation flow within a certain range (3 (0.4) mm Hg and 5–6 l/min for end exhaled NO measurements), hence improving test repeatability and enhancing patient cooperation. The sampling rate was 250 ml/min for all measurements. The analyser was calibrated daily using NO-free certified compressed air to set absolute zero and then a certified concentration of NO in nitrogen of 90 ppb and 500 ppb (BOC Special Gases, Surrey Research Park, Guildford, UK), and certified 5% CO2 (BOC). Ambient air levels of NO were recorded and the absolute zero was adjusted before all measurements. For the exhaled measurements, subjects exhaled slowly from total lung capacity over 20–30 s with an exhalation flow of 5–6 l/min. NO was sampled from a side arm attached to the mouthpiece. The mean value of the last 100 measurements, acquired with an interval of 0.04 s, was taken from the point corresponding to the plateau of end exhaled (CO2 reading 5–6%), representing the lower respiratory tract sample. Results of the analyses were computed and graphically displayed on a plot of NO and CO2 concentrations, pressure, and flow against time. The mean of three separate measurements of NO was used for analysis. Full methodological details have been previously published.7
FIBREOPTIC BRONCHOSCOPY
Subjects attended the bronchoscopy suite at 08.30 hours after having fasted from midnight and were pretreated with 0.6 mg intravenous atropine and 5–10 mg midazolam intravenously. Oxygen (3 l/min) was administered via nasal prongs throughout the procedure and oxygen saturation was monitored with a digital oximeter. After local anaesthesia of the upper airways and larynx with 4% lidocaine a fibreoptic bronchoscope (Olympus BF10 Key-Med, Southend, UK) was passed through the nasal passages into the trachea. Four segmental and subsegmental mucosal biopsy samples were taken.
BRONCHIAL BIOPSY AND PROCESSING OF TISSUES
Bronchial mucosal biopsy specimens were immediately placed in optimal cutting media (OCT), snap frozen in isopentane precooled with liquid nitrogen, and stored at –70°C. Frozen sections (6 μm) of the bronchial biopsy specimens were cut on a cryostat and placed on poly-l-lysine coated microscope slides. In order to stain for the presence of inflammatory cells, a mouse monoclonal anti-human major basic protein antibody (MBP, Monosam, Bradsure Biological, Loughborough, UK) was used to identify eosinophils. Following the primary antibody, a biotinylated rabbit anti-mouse immunoglobulin (1:100) followed by peroxidase conjugated avidin (1:200) was used. Chromogen fast diaminobenzidine was used for five minutes and the slides were counterstained with haematoxylin and mounted on mounting medium (DPX).
CELL COUNTS
Counts of positive cells were made on all sections. The number of MBP positive cells were expressed as the number per high power field. At least four fields at ×400 magnification were examined on each biopsy specimen for the specimen to be considered of adequate quality and counts included. One field was defined as a length of intact epithelium of 175 μm together with an area of 175 × 175 μm2 beneath the epithelium representing the subepithelium. The use of 175 μm is based on the measuring graticule of the microscope at ×400 magnification (Zeiss, Germany). Counts were expressed as the total number of MBP positive cells in the epithelium and subepithelium. All counts were made by two experienced observers unaware of the clinical status or origin of the sections. The coefficient of variation between the two observers was less than 10%.
DATA ANALYSIS
Data are presented as medians (range). We used the Mann-Whitney U test to compare the parameters between the two groups. Correlations between the various inflammatory parameters were also assessed with Spearman correlation tests.8
Results
PATIENT DEMOGRAPHY
The characteristics of the two groups of 16 patients enrolled in the study are shown in table 1. The steroid naive group was younger than the steroid treated group (median ages 27.8 (range 22.1–38.2) and 34.3 (25.4–45.2) years, respectively; p<0.05). Baseline lung function (FEV1) in the two groups was 94.2 (78.8–110.9) and 86.8 (51.0–107.8)% predicted, respectively, with no statistically significant difference between them.
SYMPTOM SCORES, PEAK FLOW VARIABILITY, AND RESCUE β2 AGONIST USAGE
Median symptom scores were 0.1 (range 0.00–0.80) in the steroid naive group and 0.4 (0.00–2.00) in the steroid treated group. Rescue β2 agonist medication usage was 0.4 (0.0–3.2) puffs and 1.4 (0.0–10.9) puffs/day salbutamol, respectively. Median morning PEF was 492 (377–616) l/min in the steroid naive group and 463 (241–645) l/min in the steroid treated group. Median PEF variability (amplitude % max) was 7.5 (2.0–17.0)% and 13.1 (1.5–25.5)%, respectively. Only the difference in peak flow variability was significant between the two groups (p<0.05).
EXHALED NO AND EOSINOPHIL NUMBERS IN AIRWAY BIOPSY SPECIMENS
There was a significant difference in exhaled NO levels between the two groups (table 1). The median exhaled NO levels in the steroid naive and steroid treated patients were 12.5 (3.70–29.30) and 6.90 (2.50–61.00) ppb, respectively. Sixteen biopsy specimens in the steroid naive group and 13 in the steroid treated group were of adequate quality for eosinophil counts. There was no difference in the number of mucosal eosinophils between the two groups (1.1 (0.0–7.5) and 2.3 (0.0–6.8) cells/high power field, respectively).
CORRELATION ANALYSES
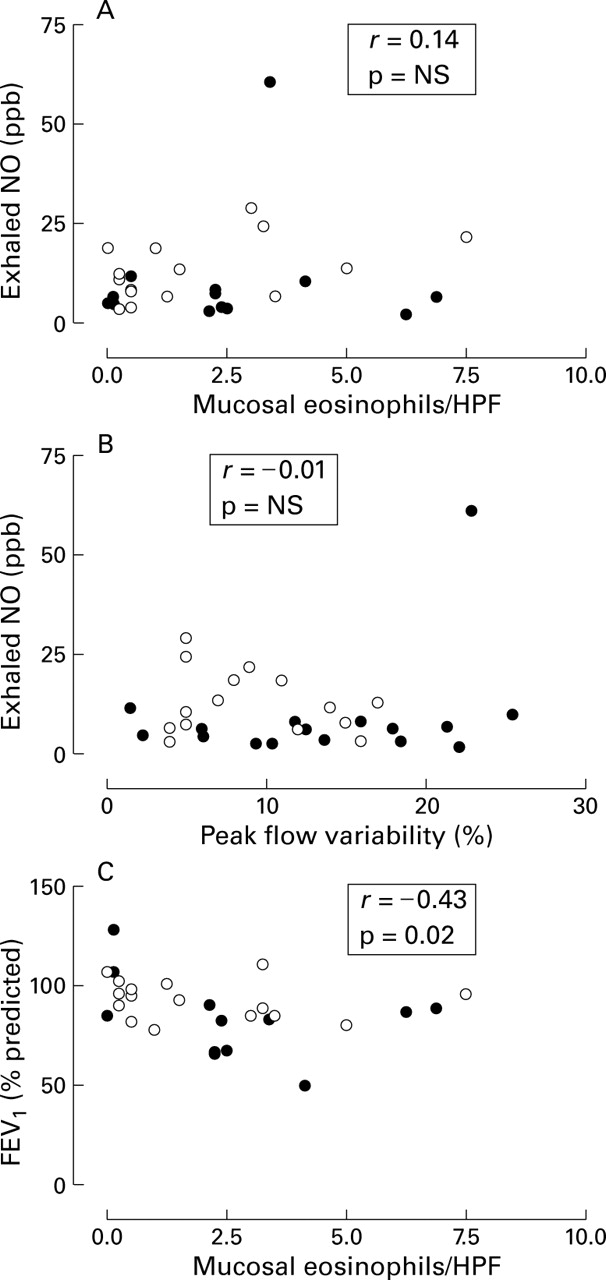
Correlations between the conventional measures, exhaled NO levels, and histological indices were sought (table 2). There were no significant correlations between exhaled NO levels and mucosal eosinophils or conventional indices of asthma control (fig 1A and B), but there was a weak correlation between mucosal histology and lung function (FEV1 % predicted, r = –0.43, p<0.05; fig 1C) and mean morning peak flow (r = –0.41, p<0.05). No other significant relationships between airway eosinophils and conventional measures of asthma control were observed. Within the conventional measures of asthma control there were significant correlations between symptoms and rescue β2 agonist usage (r = 0.45, p<0.01), rescue β2 agonist usage and lung function (r = –0.48, p<0.01), medications and mean morning PEF (r = –0.48, p<0.05), and rescue β2 agonist usage and peak flow variability (r = 0.43, p<0.05). There was a significant correlation between peak flow variability and mean morning PEF (r = –0.42, p<0.05), and between lung function and peak flow variability (r = –0.70, p<0.01). We also analysed the two groups independently but found no significant correlations within the small numbers in each group.
Correlation matrix

{kind=link}
(A) Correlation between mucosal eosinophils and exhaled levels of NO (r = 0.14, NS). Open circles represent steroid-naive patients; closed circles represent steroid treated patients. (B) Correlation between peak flow variability and exhaled levels of NO. (C) Correlation between mucosal eosinophils and FEV1 % predicted (r = –0.43, p<0.05).
Discussion
In this study we have investigated the correlations between conventional measures of asthma control (symptoms, spirometry, PEF measurements) and two other methods of assessing airway inflammation in patients with mild to moderate asthma. We found no correlations between exhaled NO levels and airway eosinophils, or between exhaled NO levels and conventional measures of asthma control. However, there was a significant correlation between airway eosinophils and lung function.
Attempts have been made to define asthma severity based upon several parameters including symptoms, impairment of activity, lung function, airway hyperresponsiveness, hospitalisation, and use of rescue β2 agonists. Although there is no unified agreement on the classification of asthma severity, a combination of asthma symptoms and lung function has been used as a guide. However, this assessment is less distinct following treatment with anti-inflammatory medications and the overall severity of asthma should include adequate asthma control using minimum medication.9 The asthma phenotypes that we have defined included patients with mild asthma and those with asthma of moderate severity. We chose these patients believing that they represented a spectrum of patients with clinically mild to moderate disease likely to be encountered in the clinical setting. However, the invasive nature of bronchoscopy mitigated against studying inflammation in those with more severe asthma. Notwithstanding this criticism, which indeed applies to most studies involving invasive assessments of inflammation, these patients gave us a range of both clinical and inflammatory indices that are representative of mild to moderate asthma. Patients treated with inhaled steroids had similar levels of symptoms, medication usage, and lung function but there was a significant difference in PEF variability and exhaled NO levels. Exhaled levels of NO did not correlate with indices of asthma control or with mucosal eosinophils. These results indicate that exhaled NO levels do not directly reflect the eosinophilic inflammatory response in asthma, and they are not an indicator of asthma control in currently used conventional terms. There was a small but significant difference in the levels of exhaled NO between patients using inhaled anti-inflammatory medications. Our results further suggest that bronchial mucosal histology, which is probably the most direct measure of inflammation in asthma, also correlated poorly with conventional parameters, though there was a significant correlation with lung function.
The internal correlations between the various conventional indices of asthma control reflect the veracity of using these conventional parameters to assess asthma severity and control. However, the failure to demonstrate relationships between these conventional measures and either exhaled NO or mucosal eosinophils could be because these measures represent different aspects of the pathophysiological processes that characterise asthma or, alternatively, it may reflect the pitfalls of the current indices being measured.
The clinical management of asthma includes monitoring lung function and symptoms. Although self-reported symptoms may be sensitive enough to detect changes in asthma control,10 some asthmatic patients have a reduced perception of respiratory sensations which may contribute to undertreatment, asthma morbidity, and mortality.11 Objective measures of lung function are not reliably performed12 and the relationship between improvement and increases in doses of inhaled steroids is relatively flat at higher doses, so that this would reduce the sensitivity of lung function measurements13 and accordingly its clinical usefulness. Airway inflammation is present in asthmatic patients whose lung function is normal and clinically well controlled without steroids. This suggests that these conventional measures may not accurately reflect inflammation within the airways.14 As there may be benefits in the early and aggressive treatment of inflammation,15 surrogate markers which seek to reflect the degree of airway inflammation better than the conventional measures currently used may aid in this.
Exhaled NO levels have been advocated as a marker of airway inflammation.3 NO has a wide array of potentially important pro-inflammatory effects in asthma including epithelial cytotoxicity, development of Th2 responses with eosinophilia, promotion of eosinophil chemotaxis, and inhibition of eosinophil apoptosis.16 The measurement of exhaled NO is completely non-invasive and can be performed repeatedly. It is possible to measure exhaled NO in children and patients with severe airflow obstruction in whom more invasive techniques are not possible. However, there is no established direct link with airway mucosal inflammation. Previously we found no significant relationship between exhaled NO levels and airway mucosal eosinophils in patients with steroid naive asthma, either before or after treatment with inhaled steroids.5 However, we found a correlation between exhaled NO levels and sputum eosinophils.17 Exhaled NO levels may reflect airway hyperresponsiveness in steroid naive patients,5-18 but these relationships are not evident in patients using inhaled steroids.18 Dupont et al 18 reported that the levels of exhaled NO in patients treated with inhaled steroids were similar to those in normal controls, but these patients still showed the continued presence of airway hyperresponsiveness which is another parameter indirectly linked to airway inflammation. These results are in keeping with our data and our patients still had evidence of mucosal inflammation despite low levels of exhaled NO. Increased levels of exhaled NO reflect inducible nitric oxide (iNOS) synthase activity in the airway epithelium, and our present data indicate that this does not correlate with the number of airway eosinophils. However, the induction of iNOS and the formation of nitrotyrosine may lead to tissue damage and inflammation.19
Bronchoscopy, although safe, is invasive and impractical for repeated day to day use to assess inflammation. Although there is a correlation between the number of eosinophils in bronchoalveolar lavage fluid and biopsy specimens and asthma severity, the correlation between mucosal eosinophils and asthma severity is weak.20 Our data are in keeping with this as we found no correlation between mucosal inflammation and conventional indices of asthma control except for a weak relationship between lung function and mucosal eosinophils.
The results of our study suggest that measurement of exhaled NO levels may not be suitable for the assessment of asthma control or airway inflammation. Using exhaled NO as a method of assessing airway inflammation requires more validation, perhaps in conjunction with induced sputum. There is also a need for more longitudinal studies involving the use of surrogate markers with conventional assessments to determine their usefulness as indicators of asthma control, which need to be distinguished from markers of inflammation.
References
Footnotes
Funding: SL is supported by Astra Draco.