Article Text

Abstract
Intrathoracic extramedullary haematopoiesis (EMH) is a rare entity that is usually asymptomatic. A 44 year old man with alpha-thalassaemia is described who developed dyspnoea and massive left sided haemothorax. The haemoglobin disorder was established by Hgb H staining and haemoglobin electrophoretic studies. The DNA analysis revealed it to be a case of double heterozygous terminal codon mutation with the genotype ααCS/ααT. Computed tomographic scanning and magnetic resonance imaging of the thorax showed multiple paravertebral masses which were found by thoracoscopic biopsy to be extramedullary haematopoiesis. Although no additional sclerosing pleurodesis or low dose radiation therapy was given, the lung expanded well and there has been no recurrence of haemothorax to date.
- extramedullary haematopoiesis
- haemothorax
- thalassaemia
Statistics from Altmetric.com
Extramedullary haematopoiesis (EMH) occurs as a compensatory phenomenon to several haematological diseases including thalassaemia, myelofibrosis, and hereditary spherocytosis. Intrathoracic EMH is a rare entity which is often located in the lower thoracic paraspinal area and is usually asymptomatic. We describe the case history of a patient who presented with alpha-thalassaemia complicated by haemothorax.
Case report
The patient, a 44 year old man, had a history of alpha-thalassaemia for some years. The disorder was diagnosed by positive haemoglobin H staining and haemoglobin electrophoretic studies (Hgb H 10.3%). DNA analysis showed a double heterozygous terminal codon mutation with genotype ααCS/ααT(CS = constant spring; T = terminal codon mutation other than CS). Bone marrow aspiration cytology revealed erythroid hyperplasia. He was admitted in February 1996 with left sided chest pain and dyspnoea for several days. There was no history of trauma. We were unable to obtain a family history of haematological disorder.
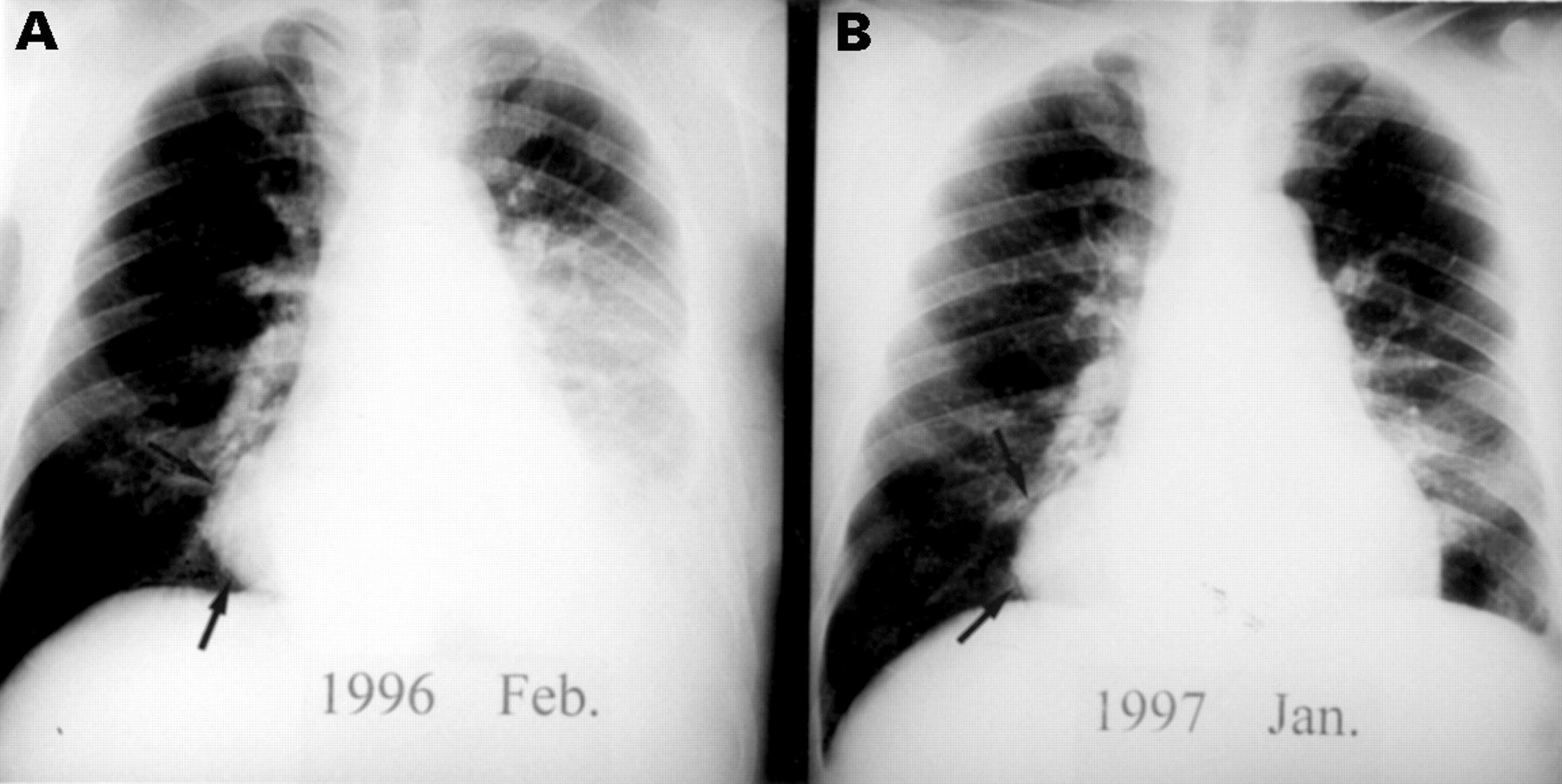
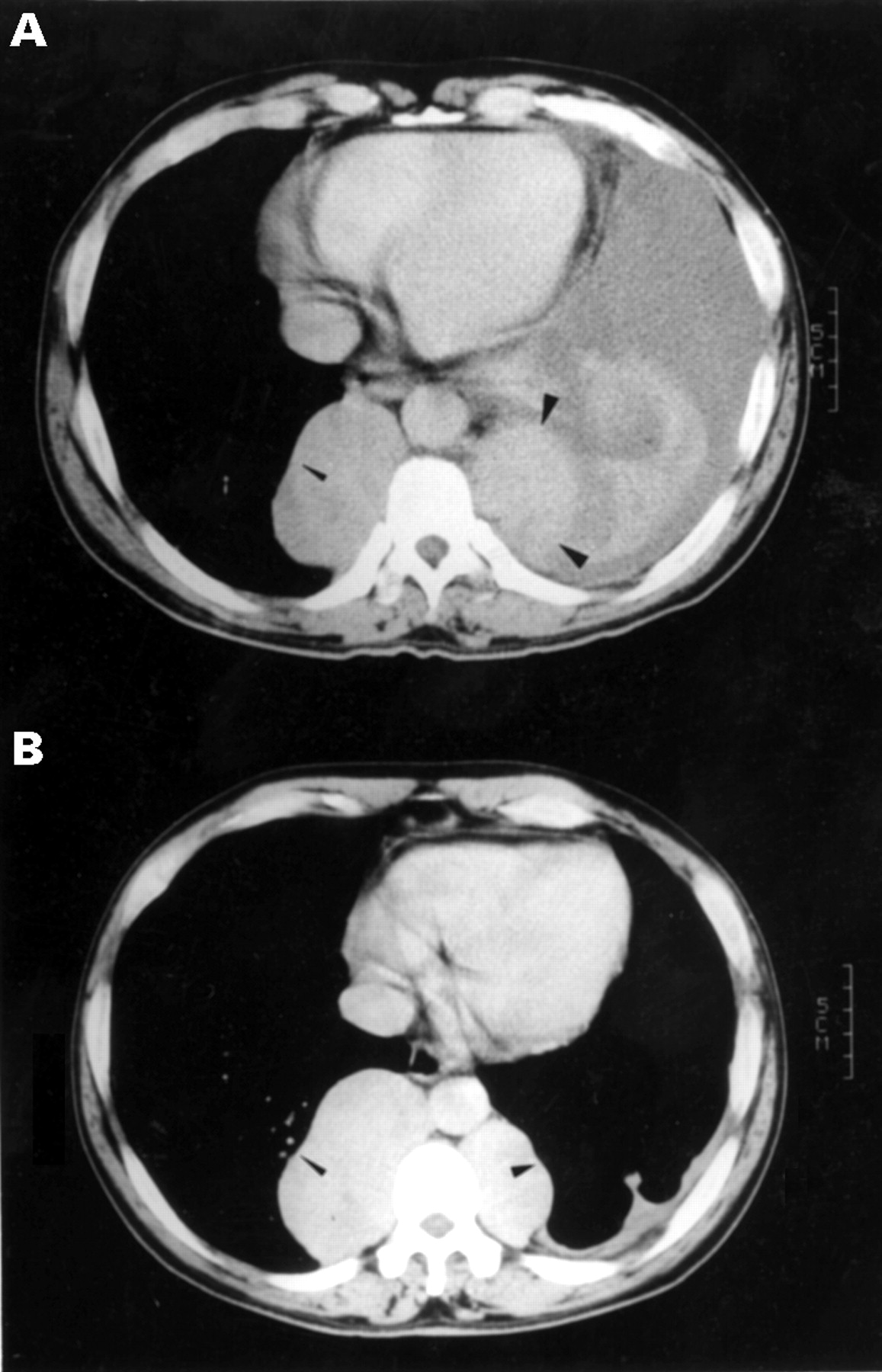
Physical examination revealed a blood pressure of 146/76 mm Hg, pulse rate of 95/min, respiratory rate of 19/min, pale conjunctiva, icteric sclera, diminished left sided breathing sounds, and marked hepatosplenomegaly. Initial haematological examination showed a haemoglobin level of 6.8 g/dl, haematocrit value of 27.1%, mean corpuscular volume (MCV) of 71.9 fl, mean corpuscular haemoglobin concentration (MCHC) of 25.1 g/dl, red blood cell count of 3.7 × 106/mm3, white blood cell count of 14 × 103/mm3, and platelet count of 2.7 × 105/mm3. Serum biochemical analysis gave the following values: iron 140 μg/dl, ferritin 374 ng/ml, total iron binding capacity (TIBC) 187 μg/dl, and total bilirubin 4.6 mg/dl. Chest radiography showed a massive left sided pleural effusion and posterior mediastinal masses (fig 1). Computed tomographic scanning of the chest revealed multiple lobulated paravertebral masses over the T spine with good contrast enhancement (fig 2). Magnetic resonance imaging of the thorax showed elongated lobulated paraspinal masses with isointensity to muscle on T1-weighted images and hyperintensity on T2-weighted images. Thoracocentesis revealed a bloody effusion with a protein level of 6500 mg/dl, sugar 5 mg/dl, red blood cell count 3.4 × 106/mm3, white blood cell count 2 × 104/mm3, and negative cytological results. Video-assisted thoracoscopy disclosed several lobulated reddish tumour masses over the lower paravertebral region and a large amount of bloody effusion. The pathological findings of a biopsy specimen of the tumour obtained by thoracoscopy revealed normal haematopoietic tissue with normal maturation process of three lineage cells.

Chest radiograph showing (A) massive left sided pleural effusion and posterior mediastinal masses (arrow) and (B) one year later only the posterior mediastinal mass (arrow) is seen without recurrence of the effusion.

{kind=link}
{kind=link}
Computed tomographic scan of the chest showing (A) massive left sided pleural effusion and multiple lobulated paravertebral masses with well enhanced contrast (arrowheads) and (B) one year later only multiple lobulated paravertebral masses (arrowhead) were found.
The patient was discharged in fair condition three weeks later without additional preventive sclerosing therapy or low dose radiation therapy. Follow up chest radiography revealed almost complete reabsorption of the left sided haemothorax and there has been no recurrence of bleeding to date.
Discussion
Alpha-thalassaemia is caused by deletion or mutation of α-globin genes. In order of increasing severity they are α-thalassaemia-2 trait (–α/αα), α-thalassaemia-1 trait (––/αα) (–α/–α), Hb H disease (––/–α), and Hb Barts (––/––). Haemoglobin constant spring (HbCS) is a common non-deletional α-thalassaemia mutation and is an important cause of HgH-like disease in south-east Asia.1 The genotype ααCS/ααT established in our patient by polymerase chain reaction is an uncommon genotype of Hg H disease. Extramedullary haematopoiesis usually develops as a compensatory response in various anaemias including thalassaemia, sickle cell anaemia, and myelofibrosis. It usually occurs in the blood forming organs outside the bone marrow such as the spleen, liver and lymph nodes, but it is also found more rarely as a mass-like lesion within the thorax. Intrathoracic EMH commonly develops in the posteroinferior mediastinum, but has also been reported in the anterior mediastinum. It is usually asymptomatic and can be found by microscopic examination,2 but it may also present as a single or multiple large tumour with occasional symptoms of spinal cord compression3 or haemothorax.2 ,4-6
As far as we are aware, only four patients with intrathoracic EMH complicated with haemothorax have been previously reported in the English literature. Smith et al 4 reported a case of thalassaemia intermedia who developed intrathoracic EMH and haemothorax which was treated with local radiation therapy to prevent recurrent bleeding. Muthuswamy and colleagues5 described a patient with hereditary spherocytosis who presented with post-traumatic intrathoracic haemorrhage due to intrathoracic EMH. Kupferschmid and colleagues2 reported a case of myelofibrosis with intrathoracic EMH. The complicated massive haemothorax did not respond to tetracycline pleurodesis and was ultimately controlled with low dose radiation therapy. Bartlett et al 6 described a case of agnogenic myeloid metaplasia with haemothorax. The intrathoracic EMH, confirmed by a technetium-99 bone marrow scan, was treated successfully with low dose irradiation to prevent recurrent haemothorax. In the case presented here, thoracoscopic biopsy and decortication were performed not only for tissue diagnosis of the posterior mediastinal mass but also for better lung expansion.
Various non-invasive diagnostic procedures are advocated to establish the diagnosis of EMH. These include contrast enhanced computed tomography,7 magnetic resonance imaging of the thorax,8 technetium-99 sulphur colloid radionuclide bone marrow scanning,9 cytological study of the pleural fluid, and fine needle aspiration examination which may carry a risk of haemorrhagic complications. Computed tomographic scanning of intrathoracic EMH typically reveals smoothly marginated mass(es) with homogenous soft tissue over the lower paravertebral regions without bony erosion. A radionuclide bone marrow scan may demonstrate activity in the mass.9
Treatment of intrathoracic EMH is usually unnecessary except in the presence of complications. Because the haematopoietic tissue is highly radiosensitive, low dose radiation has been suggested as an effective method for controlling symptomatic spinal cord compression10 and haemothorax.2 ,4 ,6 In our patient, because it was the first episode of haemothorax and there was good expansion of the lung after tube thoracostomy, we did not apply local radiation therapy. To date there has been no evidence of recurrent haemothorax.
In conclusion, based on the characteristic radiographic findings and radionuclide marrow scanning, it is important to recognise the possibility of intrathoracic EMH as a differential diagnosis of non-traumatic haemothorax, especially in patients with bone marrow insufficiency or chronic haemolytic anaemia. Although radiation therapy or sclerosing pleurodesis is suggested for recurrent haemothorax, tube thoracostomy with regular follow up is an alternative effective treatment in intrathoracic EMH with massive haemothorax.