Article Text

Abstract
Background: The relationship between the shuttle walk test and peak oxygen consumption in patients with lung cancer has not previously been reported. A study was undertaken to examine this relationship in patients referred for lung cancer surgery to test the hypothesis that the shuttle walk test would be useful in this clinical setting.
Methods: 125 consecutive patients with potentially operable lung cancer were prospectively recruited. Each performed same day shuttle walking and treadmill walking tests.
Results: Shuttle walk distances ranged from 104 m to 1020 m and peak oxygen consumption ranged from 9 to 35 ml/kg/min. The shuttle walk distance significantly correlated with peak oxygen consumption (r = 0.67, p<0.001). All 55 patients who achieved more than 400 m on the shuttle test had a peak oxygen consumption of at least 15 ml/kg/min. Seventy of 125 patients failed to achieve 400 m on the shuttle walk test; in 22 of these the peak oxygen consumption was less than 15 ml/kg/min. Nine of 17 patients who achieved less than 250 m had a peak oxygen consumption of more than 15 ml/kg/min.
Conclusion: The shuttle walk is a useful exercise test to assess potentially operable lung cancer patients with borderline lung function. However, it tends to underestimate exercise capacity at the lower range compared with peak oxygen consumption. Our data suggest that patients achieving 400 m on the shuttle walk test do not require formal measurement of oxygen consumption. In patients failing to achieve this distance we recommend assessment of peak oxygen consumption, particularly in those unable to walk 250 m, because a considerable proportion would still qualify for surgery as they had an acceptable peak oxygen consumption.
- FEV1, forced expiratory volume in 1 second
- Kco, carbon monoxide transfer coefficient
- Tlco, carbon monoxide transfer factor, V˙o2peak, peak oxygen consumption
- lung function
- lung cancer
- shuttle walk test
- oxygen consumption
- surgery
Statistics from Altmetric.com
- FEV1, forced expiratory volume in 1 second
- Kco, carbon monoxide transfer coefficient
- Tlco, carbon monoxide transfer factor, V˙o2peak, peak oxygen consumption
Surgery remains the treatment of choice for resectable lung carcinoma with respect to curability. However, some surgical patients have a poor postoperative outcome, usually due to the presence of co-existing disease, especially chronic obstructive pulmonary disease (COPD). To assist the prediction of surgical outcome, a range of cardiopulmonary exercise tests have been used. These include maximal exercise tests, full lung function, and walk tests.
A number of studies have suggested that cardiopulmonary exercise testing is one of the most valuable parameters for the evaluation of risk assessment in lung cancer surgery.1–5 It provides the best index of functional capacity and global oxygen transport/consumption (V˙o2), as well as estimating both cardiac and pulmonary reserve not available from other modalities. However, cardiopulmonary exercise testing is often poorly available in Europe.
The 10 metre shuttle walk test is a standardised, externally paced, incremental and progressive field test which is readily available in most hospitals. It is a reproducible measure of functional capacity in patients with chronic airflow limitation.6 In patients with COPD the shuttle walk test has been shown to be closely correlated with V˙o2max.7 However, there are no data comparing the relationship between shuttle walk distance and V˙o2peak in patients with lung cancer. These data are necessary as many patients with bronchogenic carcinoma do not have COPD and may therefore have different respiratory physiology.
In the selection of patients for lung cancer surgery, both the British Thoracic Society (BTS)8 and American College of Chest Physicians (ACCP)9 suggest that all patients with borderline lung function and with predicted postoperative forced expiratory volume in 1 second (FEV1) or carbon monoxide transfer factor (Tlco) of less than 40% should undergo exercise testing before surgery. However, the scientific rationale for this strategy is rather vague. In those patients who subsequently undergo shuttle walk testing and fail to complete 250 metres, it is recommended that surgery should not be attempted.8,9 This is because it is believed that failure to achieve this distance would predict a V˙o2max of less than 10 ml/kg/min and thus a high risk of poor postoperative outcome. The basis of this prediction between shuttle walk distance and oxygen consumption originates from work using the regression equation developed by Singh et al.7 However, Singh’s study population was small and all the patients had COPD so it does not necessarily reflect the lung cancer patient population. Indeed, only limited data are available on the ability of the shuttle walk test to predict oxygen consumption.10
A prospective study was therefore performed to examine the relationship between the shuttle walk test and oxygen consumption specifically in preoperative lung cancer patients with both normal and borderline lung function.
METHODS
Patients
125 consecutive patients with potentially resectable lung cancer (81 men) of mean age 69 years (range 42–85) were prospectively recruited. Forty one (33%) had borderline lung function (FEV1 <1.5 l for lobectomy and FEV1 <2.0 l for pneumonectomy). Exclusion criteria included unstable angina, recent myocardial infarction (within 6 weeks), and disorders that might influence exercise performance physically such as severe back pain. The local ethics committee approved the study and all patients gave informed consent.
The shuttle walking and treadmill walking tests were performed on the same day, at least 4 hours apart. The patients were fully familiarised with both tests before the start. All patients also underwent full pulmonary function tests according to the guidelines of the Association of Respiratory Technology and Physiology.11 Follow up data were analysed 12 months after surgery.
Shuttle walking test
The shuttle walking test was performed using methods established by Singh et al.6 Patients walked between two cones 10 metres apart at an incrementally increasing pace. Each increment was signalled by a fully calibrated audiocassette. To assist, the operator accompanied the patient throughout the test. The end point was reached when the patient could no longer maintain the required speed or became too breathless to proceed further. Using a pulse oximeter (Minolta Pulsox 3i), oxygen saturation and heart rate were recorded every 30 seconds throughout the test.
The Borg breathlessness score12 was also recorded at the beginning and end of the test. A note of the recovery time and the reason for terminating the shuttle walk were also recorded.
Cardiopulmonary exercise test (V˙o2 test)
The cardiopulmonary exercise test was performed using the Oxycon-Pro Exercise System Viasys Healthcare with the Standardized Exponential Exercise Protocol (STEEP) as described by Northridge et al,13 with the exception of an additional 1 minute warm up period. The STEEP protocol was devised to allow a single protocol to be selected for subjects with a wide range of exercise capacities which could be applied to the treadmill. The protocol commenced at a low workload and was increased exponentially by 15% every minute. The treadmill protocol involved changes in either gradient or speed, but never both simultaneously.
The test lasted a maximum of 20 minutes, of which the patient exercised for 16 minutes and 4 minutes were taken up with baseline measurements and recovery. Patients were required to exercise for as long as possible until they were sign and/or symptom restricted. The ECG was monitored throughout the test, and oxygen and carbon dioxide were measured from the expired air. The Borg breathlessness score12 and the reason for terminating the test were also recorded.
Three V˙o2 values measured in the final 30 seconds of the exercise phase were averaged to obtain the V˙o2peak. We defined the oxygen consumption as V˙o2peak rather than V˙o2max since V˙o2max is usually obtained from the maximum oxygen consumption during the plateau stage of exercise in healthy subjects. However, in many patients it is often difficult to maintain this plateau stage of exercise, so in our patients V˙o2peak is considered more useful and not significantly different from V˙o2max.14
Statistical analysis
The baseline characteristics are presented as mean (SD) values. The Student’s t test was used for subgroup comparisons of these measurements. Pearson’s correlation coefficients were used to assess the associations between measurements of respiratory physiology and exercise capacity. In those patients who underwent surgery, survival time was measured from the date of the procedure to the date of death and was censored at 15 August 2005 for surviving patients. Kaplan-Meier survival rates were estimated and compared using a log rank test. Receiver operating characteristic (ROC) curves were used to assess the value of the shuttle walk test on 12 month survival in patients who underwent surgery. The Wilcoxon test was used to assess whether the area under the ROC curve was significantly greater than 0.5.
RESULTS
All patients completed the study. Baseline characteristics, FEV1, FEV1 % predicted, Tlco % predicted, Kco % predicted, shuttle walk distance, V˙o2peak, and V˙o2peak % predicted are shown in table 1. Shuttle walk distances ranged from 60 m to 1020 m (mean 400 m). During the walk, mean desaturations of 0–14% were recorded. Changes in Borg score ranged from 0 to 6 (mean 2.3). V˙o2peak ranged from 9 to 35 ml/kg/min (mean 18.3 ml/kg/min); 44.3–189% of normal predicted (mean 84%).
Baseline characteristics and lung function values
Fifty five of the 125 patients achieved more than 400 m on the shuttle test, all of whom had a measured V˙o2peak of ⩾15 ml/kg/min. Seventy of the 125 patients failed to achieve 400 m on the shuttle walk test; in 22 of these patients (31.5%) the V˙o2peak was <15 ml/kg/min. Seventeen patients achieved less than 250 m on the shuttle walk test, nine of whom had a V˙o2peak of >15 ml/kg/min while 16 of the 17 had a V˙o2peak of >10 ml/kg/min.
The maximum heart rate ranged from 77 to 185 beats/min. No significant arrhythmias were recorded during the tests. All patients had a recovery time (time to return to pre-exercise oxygen saturation and Borg score) of less than 4 minutes. No adverse effects were noted. Two patients developed significant ST changes (⩾1 mm ST elevation or depression) without symptoms; they were referred for coronary angiography which confirmed significant coronary artery disease. Table 2 shows the reasons for stopping exercise tests.
Reasons for stopping exercise tests
There was a significant correlation between shuttle walk distance and V˙o2peak (r = 0.67, p<0.001; fig 1), but the correlation between shuttle walk distance and V˙o2peak % predicted was weak (r = 0.30). There was a moderate correlation between actual V˙o2peak and FEV1 (r = 0.49) and between shuttle walk distance and FEV1 (r = 0.5). There was no significant correlation between oxygen saturation and Borg score (r = 0.10) or between oxygen saturation and shuttle walk distance (r = 0.063). There was moderate correlation between shuttle walk distance and change in Borg score (r = 0.33).

Correlation (r = 0.67) between shuttle walk distance (m) and peak oxygen consumption (V˙o2peak, ml/kg/min).
The relationship between shuttle walk distance and V˙o2peak was the same in patients with normal lung function as in those with borderline pulmonary function. Forty three patients whose FEV1 was considered adequate for lung cancer surgery (according to the guidelines) could not achieve 400 m on the shuttle walk test. There was no statistically significant association between lung function tests (FEV1 or FEV1/VC%) and either V˙o2peak or shuttle walk distance (table 3).
Correlation between shuttle walk distance, peak oxygen consumption (V˙o2peak) and lung function
The final decision to operate was taken in the multidisciplinary team meeting, depending on physiological data, co-morbidity, and cardiothoracic surgical opinion. The reason for non-operation was upstaging in 86% (for example, after positron emission tomography) and 14% were excluded for co-morbidity (for example, heart disease or poor respiratory reserve secondary to COPD).
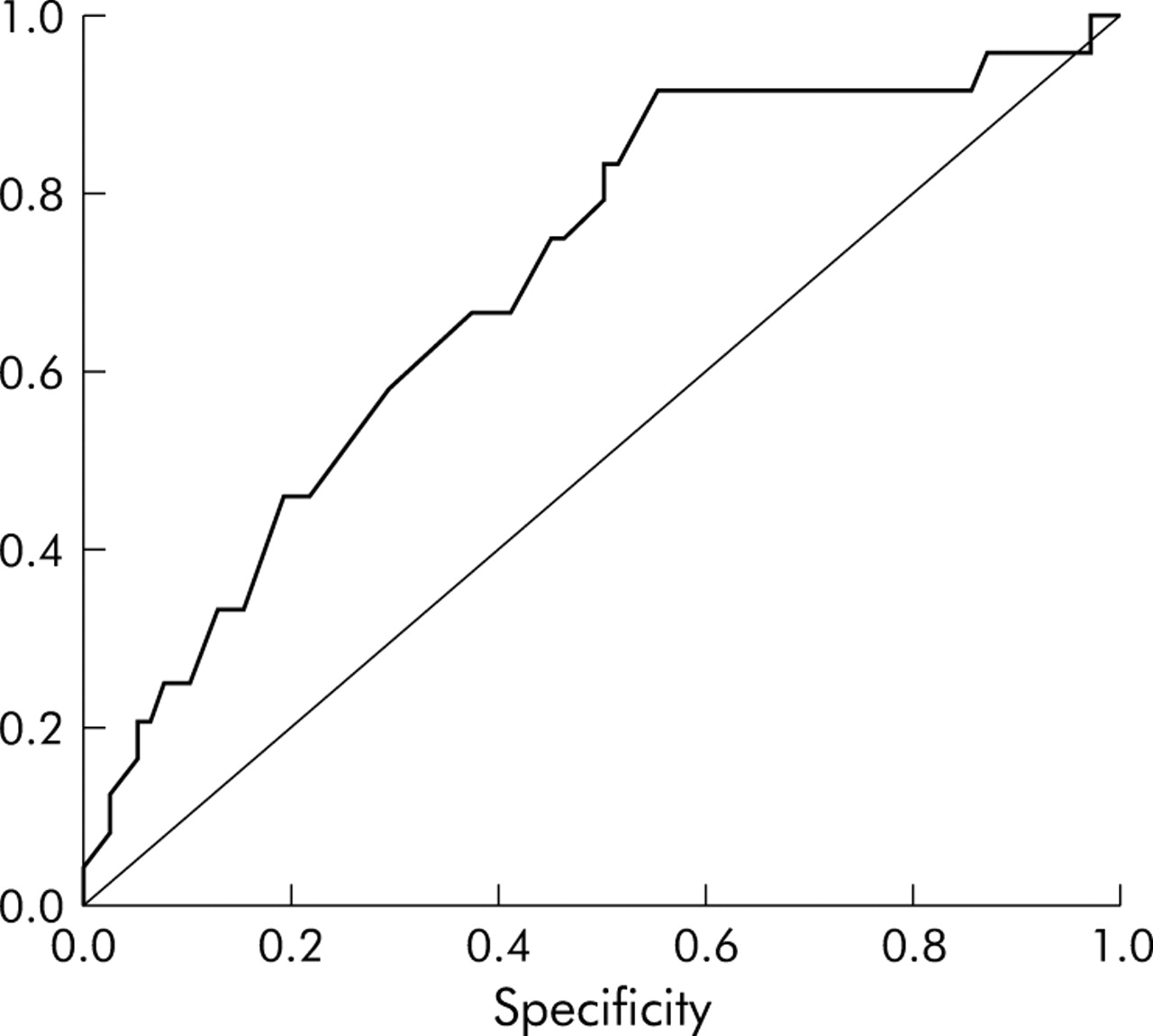
Of the 100 patients with a V˙o2peak of ⩾15 ml/kg/min, 85 had surgery. At 1 year after surgery 69 of the 85 (81%) had survived. Of the 25 patients with V˙o2peak of <15 ml/kg/min, 17 had surgery and at 1 year nine of them (53%) had survived. The mean (SD) V˙o2peak in those who survived 1 year after surgery was 19.5 (4.4) ml/kg/min compared with 16.9 (4.1) ml/kg/min in those who died (p = 0.013). Figure 2 shows the ROC curve for shuttle walk test against 1 year survival in patients who underwent surgery. The area under the curve is 0.70 (p = 0.003), indicating that the shuttle walk test has significant predictive value. A threshold of 400 m in the shuttle walk test had a sensitivity of 77% and specificity of 54% for 1 year survival. One year after surgery, 42 (88%) of 48 patients who achieved a shuttle walk distance of 400 m or more had survived compared with 36 of 54 (67%) of those who did not achieve 400 m (fig 3). The mean (SD) shuttle walk distance in those who survived to 1 year was 428 (135) m compared with 335 (122) m in those who died (p = 0.003).

Receiver operating characteristic curve for shuttle walk test distance against 12 month survival in patients who underwent surgery. The area under the curve is 0.70 (p = 0.003).

{kind=link}
{kind=link}
{kind=link}
Kaplan-Meier survival curve showing the survival advantage of patients achieving 400 m in the shuttle walk test compared with those who walked less than 400 m.
DISCUSSION
We have shown that the relationship between V˙o2peak and shuttle walk distance is significantly closer than the relationship between V˙o2peak and any other parameters of lung function. In addition, the relationship between shuttle walk distance and V˙o2peak was the same in patients with normal lung function as in those with borderline pulmonary function. In fact, many patients with acceptable lung function according to the guidelines failed to achieve 400 m on the shuttle walk test, and this could imply that the use of static lung function tests in this setting might be limited. Shuttle walk distance and change in the Borg breathlessness score had a weak correlation. The reason for terminating the test was mainly speed limitation in the shuttle walk test, whereas symptoms such as leg pain were the main cause for cessation on the treadmill. There was a weak correlation between shuttle walk distance and V˙o2peak percentage predicted. As there is no established predicted shuttle walk distance for each individual, we are unable to correlate the percentage predicted of these two different tests.
Although we found there to be significant correlation between shuttle walk distance and V˙o2peak (r = 0.67; 95% confidence interval 0.56 to 0.76; n = 125), the correlation was weaker than that claimed by Singh et al (r = 0.88, n = 19).7 The reason for this difference is multifactorial. Singh’s cohort was younger, predominantly male, and all suffered from COPD rather than lung cancer. Their patients also had lower V˙o2peak and FEV1 values. In addition, our patient group was likely to have been better motivated by the incentive of curable surgery.
There is evidence that tests such as the modified shuttle walk test,15 Cooper walk run test,16 and the multi-stage shuttle run test17 correlate better with oxygen consumption than the shuttle walk test. However, these procedures require vigorous exercise and, as such, would be inappropriate to perform in our patients who are usually elderly and frequently suffer from chronic lung disease. Another walk test often used is the 6 minute walk test. However, interpretation of the distance walked in 6 minutes is currently not well standardised.18 Although the stair climbing test has been used historically as a surrogate for cardiopulmonary exercise test,19 it is not performed in standardised manner. The shuttle walk test has been shown to be reproducible and a good predictor of the impact of breathlessness on functional capacity in patients with cancer.20 We therefore chose to perform the shuttle walk test as a reliable field test on our patients.
We used the STEEP protocol as it had numerous advantages for our patient cohort and has been validated against a wide range of patients with different exercise capacities.13 This was important as 33% of our patients had borderline lung function. The STEEP protocol has also been validated in patients with coronary artery disease21 and a number of our patients had evidence of myocardial ischaemia. It also benefits from versatility as it can be used with either exercise bike or treadmill.
A correlation of 0.67 between the shuttle walk distance and V˙o2peak has possible implications for both the BTS and ACCP guidelines for selecting patients for lung cancer surgery. At present it is recommended that patients who cannot walk 250 m on the shuttle walk test need not undergo V˙o2 measurements as it is assumed that the V˙o2max would be less than 10 ml/kg/min and that therefore they would be in a high risk group for surgery. However, these recommendations appear to have come from limited data on patients with COPD.7 Our findings suggest that, if the present guidelines are adhered to with respect to the 250 m cut off, then some patients would needlessly be excluded from surgery. In our study nine patients who failed to reach 250 m had a measured V˙o2peak which exceeded 15 ml/kg/min and thus would meet the criteria for surgery. In fact, with one exception, all patients who failed to reach 250 m had V˙o2peak measurements of >10 ml/kg/min.
Our experience showed that all patients who exceeded 400 m on the shuttle walk test had V˙o2peak measurements of >15 ml/kg/min. One can therefore argue that measurement of V˙o2 in these patients is unnecessary since a V˙o2peak of >15 ml/kg/min has been shown to be quite safe for resections. Indeed, the survival data would seem to confirm the usefulness of the 400 m cut off. Although this finding may not benefit all patients, a sizeable cohort would be saved an invasive test and these patients could be investigated outside tertiary care centres. Patients undergoing complete pneumonectomy may need a more rigorous assessment regime. The predicted postoperative FEV1 has been shown to be a particularly useful parameter in this setting,22 and this could be combined with V˙o2 measurements in patients undergoing pneumonectomy.
In conclusion, the shuttle walk test is a useful and readily available exercise test that assesses potentially operable lung cancer patients with borderline lung function. In these patients, distance performance on the shuttle walk test relates significantly to V˙o2peak during treadmill testing. However, it tends to underestimate exercise capacity at the lower range compared with V˙o2peak. Our findings also suggest that patients who exceed 400 m on the shuttle walk test may not need V˙o2 assessment. In patients failing to achieve this distance we would recommend V˙o2 assessment. This is particularly important in those unable to walk 250 m as many of these subjects had a V˙o2peak in excess of 15 ml/kg/min and thus would have an acceptable surgical risk.
REFERENCES
Footnotes
-
Published Online First 21 October 2005
-
This work received funding from the Research and Development NHS Executive.
-
Competing interests: none.