Article Text

Abstract
Background The lung clearance index (LCI) derived from the multiple breath inert gas washout (MBW) test reflects global ventilation distribution inhomogeneity. It is more sensitive than forced expiratory volume in 1 s (FEV1) for detecting abnormal airway function and correlates closely with structural lung damage in children with cystic fibrosis, which shares features with primary ciliary dyskinesia (PCD). Normalised phase III slope indices Scond and Sacin reflect function of the small conducting and acinar airways, respectively. The involvement of the peripheral airways assessed by MBW tests has not been previously described in PCD.
Methods A cross-sectional MBW study was performed in 27 children and adolescents with verified PCD, all clinically stable and able to perform lung function tests. LCI, Scond (n=23) and Sacin (n=23) were derived from MBW using a mass spectrometer and sulfur hexafluoride as inert marker gas. MBW indices were compared with present age, age at diagnosis and spirometry findings, and were related to published normative values.
Results LCI, Scond and Sacin were abnormal in 85%, 96% and 78% of patients with PCD and in 81%, 93% and 79%, respectively, of 13/27 subjects with normal FEV1. LCI and Sacin correlated significantly while Scond did not correlate with any other lung function parameters. None of the lung function measurements correlated with age or age at diagnosis.
Conclusions PCD is characterised by marked peripheral airway dysfunction. MBW seems promising in the early detection of lung damage, even in young patients with PCD. The relationship of MBW indices to the outcome of long-term disease and their role in the management of PCD need to be assessed.
- MBW
- lung clearance index
- lung
- spirometry
- cross-sectional studies
- cystic fibrosis
- paediatric lung disaese
- paediatric physician
- exhaled airway markers
- paediatric asthma
- bronchiectasis
- imaging/CT MRI etc
- rare lung diseases
- asthma
- lung physiology
Statistics from Altmetric.com
- MBW
- lung clearance index
- lung
- spirometry
- cross-sectional studies
- cystic fibrosis
- paediatric lung disaese
- paediatric physician
- exhaled airway markers
- paediatric asthma
- bronchiectasis
- imaging/CT MRI etc
- rare lung diseases
- asthma
- lung physiology
Introduction
Primary ciliary dyskinesia (PCD) is a rare congenital disease characterised by defective ciliary function, which leads to impaired mucociliary clearance and consequently to recurrent and chronic upper and lower airway infections.1 2 Patients with PCD most often present with persistent rhinitis and chronic productive cough, but the heterogeneous nature of the disease makes early diagnosis difficult.3 A recently published longitudinal study from our centre suggested that PCD is a disease which seriously compromises lung function already at preschool age with a highly variable course of forced expiratory volume in 1 s (FEV1) and forced vital capacity (FVC) even after early diagnosis.4 However, traditional spirometry is mostly sensitive in detecting proximal airway disease, which may have limitations as early lung damage in PCD may be of peripheral origin. This is supported by a case report in which two of three patients with PCD who had infant pulmonary lung function performed demonstrated values suggestive of primary pathology in smaller peripheral airways.5
PCD lung disease shares several features with cystic fibrosis (CF): clinical findings include chronic productive cough and, although less frequent, colonisation by Pseudomonas aeruginosa (PA),6 and radiological changes include bronchiectasis, mucus plugging and peribronchial thickening.7 However, although data on early structural changes in PCD lung disease are lacking, it is reasonable to suggest that PCD may resemble CF in which initial lung damage has been shown to start in the peripheral airways.8 In CF, spirometry has traditionally been used to monitor lung function, but several studies have shown spirometry to be insensitive in tracking early progressive lung disease.9–12 The lung clearance index (LCI), derived from a multiple breath inert gas washout test (MBW), is a measure of global ventilation inhomogeneity (VI) and small airway dysfunction. LCI has been shown to detect lung damage in CF more readily than other pulmonary function tests9 13 and to be predictive of subsequent lung function when measured at preschool age.10 In addition, determination of concentration normalised phase III slope (SnIII) indices allows assessment of VI arising in the small conductive airway zone (Scond) and more peripherally close to or within the acinar airway zone (Sacin).14 Peripheral airway function assessed by LCI, Scond and Sacin in children and adolescents with PCD has not been previously reported.
The aim of our study was to assess peripheral airway function in children and adolescents with PCD using MBW and to compare the findings with spirometry. We hypothesised that PCD lung disease is characterised by marked peripheral dysfunction, and that abnormal ventilation distribution is a frequent finding despite normal spirometry. Some of the study results have been previously reported in abstract form.15
Methods
Design of study
This was a cross-sectional prospective study. All patients had lung function and MBW tests performed at their routine annual review at the National Danish PCD Center. Management is according to previous publications from the same centre.4
Study patients
Patients with a diagnosis of PCD aged ≤18 years were eligible for the study. All patients had a consistent history of symptoms characteristic of PCD,16 17 and basic tests to rule out CF and immunodeficiency were performed. Nasal nitric oxide measurement (nNO) was used as a preliminary screening test, although without necessarily excluding patients with a high suspicion of PCD.18 Furthermore, functional studies on ciliary beat pattern and frequency analysis using video recording and electron microscopy (EM) analysis of ciliary ultrastructure were key diagnostic tests.1 Functional studies were performed twice, at least one month apart. Patients had to be considered in a stable clinical condition on the day of MBW measurement.
Measurements
MBW
Tidal breathing sulfur hexafluoride (SF6) washout was performed in all patients using a mass spectrometer (AMIS 2000, Innovision, Odense, Denmark) for gas analysis, as previously described.13 The LCI and the concentration normalised slope III indices (Sacin and Scond) were calculated. LCI was calculated as the number of lung volume turnovers (TO; ie, the cumulative expired volume divided by the functional residual capacity, FRC) needed to lower the end-tidal tracer gas concentration to less than 1/40th of the starting concentration.13 The mean LCI result from three MBW measurements in each patient was used for analysis. The concentration normalised slope of phase III (SnIII) for each subsequent breath during MBW was determined to calculate Scond and Sacin. The phase III slope was converted to SnIII by dividing the slope by the mean gas concentration over the slope to allow for gas dilution. The SnIII was further multiplied by tidal volume (VT) giving the SnIII × VT in order to account for inter-individual differences in lung size and breathing pattern.19 The SnIII × VT was used in all subsequent analyses and is henceforth referred to as SnIII in this paper. For determination of Scond and Sacin, SnIII and TO values for each subsequent breath from the three washouts were first averaged. For each breath, SnIII was then plotted against the corresponding TO value. Scond was defined as the rate of SnIII increase between TO 1.5 and 6.0. Sacin was defined as the first breath SnIII value minus the convection-dependent inhomogeneity contribution to this value (ie, Scond × TO for the first breath). MBW results from this study were compared with data previously collected in healthy Swedish schoolchildren obtained using identical equipment, software and procedures.13 20 The authors performing and calculating the MBW tests have undergone training and been under continual supervision by the Swedish laboratory. Further technical details and reference values of the MBW technique are provided in the online supplement and elsewhere.20
Statistical analysis
Lung function was expressed as z-scores, which were calculated as (measured value − predicted value)/RSD from the reference population.22 The upper limit of normal (ULN) was defined as the predicted mean plus 1.96 RSD for MBW variables and the lower limit of normal (LLN) as predicted mean minus 1.96 RSD for spirometry variables. MBW parameters were correlated to spirometry parameters, age and age at diagnosis using a linear regression model. A p value of <0.05 was accepted as statistically significant. SAS V.9.2 (SAS Institute) was used for statistical analyses.
Results
Twenty-seven patients with PCD from the National Danish PCD cohort were included in the study; all patients had LCI measurements performed. SnIII indices could not be calculated in four patients owing to irregular breathing patterns. In two patients spirometry was performed on a separate day because of technical problems and the dataset closest in time to the date of the MBW test (5 weeks later) was used instead. Both patients were clinically stable on the day spirometry was performed, and spirometry showed stable measurements over time.
Three patients did not have a conclusive abnormal ciliary beat pattern and frequency during the investigation. One had clinical signs and symptoms of PCD, situs inversus, hydrocephalus, repeated abnormal pulmonary radioaerosol mucociliary clearance tests,23 borderline abnormal nNO, low exhaled NO measurements <5 ppb, but conflicting functional studies not certain of abnormal beat pattern and an EM without classical ultrastructural defects. Two other patients did not have a conclusive ciliary function test as they both refused to participate in further functional studies after the initial one: one patient had classical clinical PCD, extremely low nNO and classical abnormal EM; the other had classical clinical PCD and an abnormal EM and very low nNO. In addition, the latter had a brother with PCD with identical EM presentation and immotile cilia on functional studies. Demographic and diagnostic characteristics are shown in table 1.
Demographic and diagnostic characteristics of study population
Lung function results are summarised in table 2. Mean (SD) absolute values of MBW variables in patients with PCD were all markedly abnormal compared with normal reference values: LCI=9.48 (2.20) vs 6.33 (0.43), ULN=7.17; Scond=0.076 (0.024) vs 0.018 (0.006), ULN=0.030; and Sacin=0.236 (0.115) vs 0.086 (0.025), ULN=0.135. LCI was above the ULN in 84% of patients (23/27), while 96% (22/23) and 78% (18/23) had abnormal Scond and Sacin, respectively.
Spirometry and multiple breath inert gas washout (MBW) measurements
The relationships between LCI and the SnIII indices Sacin and Scond are shown in figure 1A and B. LCI correlated to Sacin (R2=0.45; p<0.001) but not to Scond. Scond peaked at an LCI of about 10 z-scores, subsequently decreasing with increase in disease severity (as measured by LCI). Sacin and Scond did not correlate (figure E1 in online supplement).

(A) Scond and (B) Sacin versus LCI z-scores in 23 patients with primary ciliary dyskinesia. The dashed horizontal lines denote the upper limits of normality for LCI (mean plus 1.96 SD) and the dashed vertical lines denote the upper limits of normality (mean plus 1.96 SD) for Sacin and Scond, respectively. LCI, lung clearance index; Scond and Sacin, normalised phase III slope indices (see text for explanation).
Mean values of spirometry parameters across the cohort were within or close to normal limits; 52% (14/27) had abnormal FEV1 and 15% (4/27) had abnormal FVC.
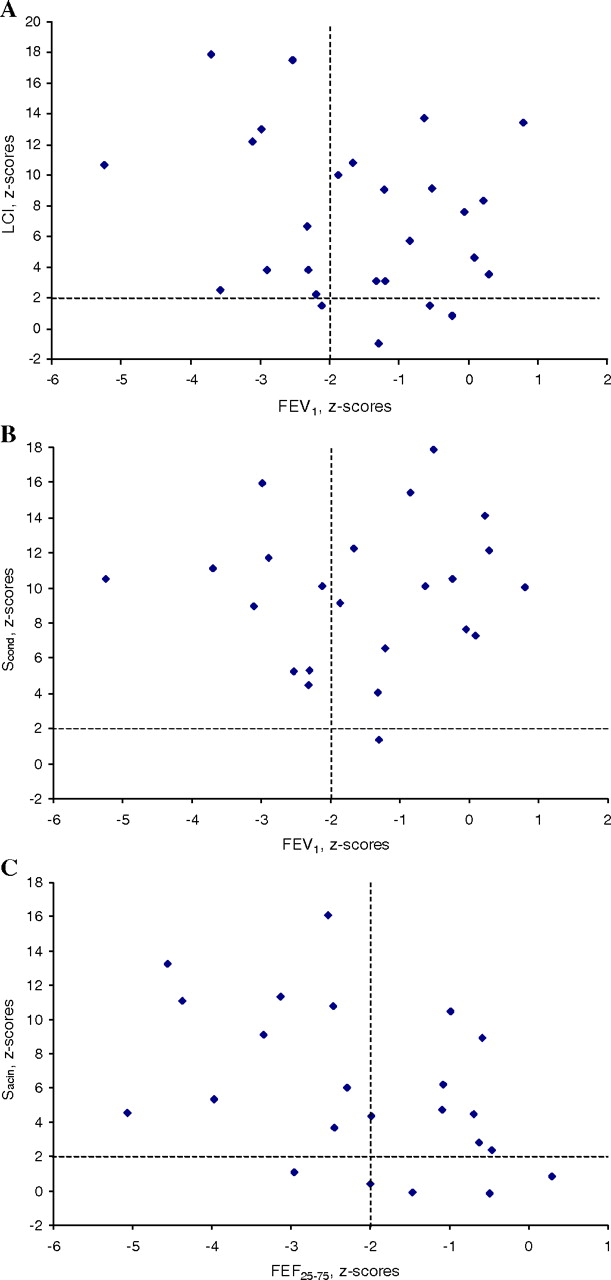
LCI did not show a statistically significant correlation with either FEV1 or FVC. LCI, Scond and Sacin were abnormal in 81% (13/16), 93% (13/14) and 79% (11/14), respectively, among the 13/27 patients with normal FEV1 (figure 2A–C). Normal LCI excluded the presence of abnormal FEV1, with the exception of a marginally reduced FEV1 (−2.1 z-scores) in one patient. In addition, this patient had Sacin within the normal range while Scond was elevated at more than 10 z-scores. When relating SnIII indices to spirometry parameters, neither Sacin nor Scond correlated with FEV1 or FVC.
{kind=link}
{kind=link}
(A) LCI z-scores from MBW versus FEV1 in 27 patients with primary ciliary dyskinesia (PCD). (B) Scond and (C) Sacin from MBW versus FEV1 z-scores in 23 patients with PCD. The dashed horizontal lines denote the upper limits of normality for lung clearance index, Scond and Sacin (mean plus 1.96 SD) and the dashed vertical lines denote the lower limits of normality (mean minus 1.96 SD) for FEV1. FEV1, forced expiratory volume in 1 s; LCI, lung clearance index; MBW, multiple breath inert gas washout; Scond and Sacin, normalised phase III slope indices (see text for explanation).
The inclusion of spirometry results performed for two patients on a different date from the MBW did not have any effect on the statistical analysis with regard to FEV1 and FVC. Correlations between lung function parameters are summarised in table E1 in the online supplement.
There was no significant correlation between any of the lung function parameters and age or age at diagnosis, respectively. Table E2 in the online supplement shows correlations between MBW indices and age and age at diagnosis.
Comparisons between MBW parameters and FEF25–75 and FEV1/FVC ratio are given in the online supplement.
Discussion
This is the first report presenting data from MBW findings in a cohort of well-characterised children and adolescents with PCD. We found that MBW was more frequently abnormal than FEV1, the currently accepted spirometry surrogate marker of disease severity. Abnormal LCI was found in nearly all patients, including those with normal FEV1. Additionally, Scond was abnormal in all but one patient and Sacin in more than three-quarters of the patients, implying involvement of small airways even beyond the conducting airway zone. MBW parameters did not correlate with FEV1 or FVC. Measures of spirometry were on average all within or close to normal values and half the patients had normal FEV1, while the indices of VI were considerably elevated. Our findings show that PCD lung disease is characterised by marked peripheral dysfunction which, in most cases, is not detectable by spirometry.
The results of this study are consistent with previous publications showing that MBW is more sensitive than spirometry in detecting pulmonary diseases such as CF.9 12 13 24 25 To our knowledge, the only other information to date on MBW data in PCD is an abstract by Ives et al who investigated adult patients with PCD, thus making direct comparison with our study difficult.26
In a recent large longitudinal study in the Danish PCD cohort published from our centre4 we found a high degree of variation in the course of lung function after diagnosis. This variation could not be linked to age or to the level of lung function (ie, spirometry findings) at the time of diagnosis, with the conclusion that early diagnosis and initiated treatment, even in a tertiary centre, does not protect against decline in lung function.4 This is in line with the current study where we did not find any relationship between the degree of VI and age at diagnosis of PCD. Possible explanations are that (1) our current monitoring and management of patients with PCD is based on extrapolation of CF care which may not be sufficient; and (2) changes in spirometry values are unable to detect early lung damage as implied by our study. The latter may cause a delay in intensification of treatment when needed.
Results from studies in children and adults with CF suggest that SnIII analysis is of limited use in more advanced disease.27 Consistent with this view, we found Scond to be markedly elevated even in patients with mild disease, as indicated by LCI or spirometry. In our cross-sectional analysis, Scond reached a plateau and then declined with higher LCI. Scond results from differences in specific ventilation and sequential filling and emptying among lung regions sharing branch points in the conducting airway zone. This index thus reflects the ‘patchiness’ of disease distribution. With increasing disease severity, ventilation of already poorly ventilated lung units will come to an end and inter-regional differences in ventilation non-uniformity will not increase additionally. At the same time, it could be speculated that disease progression in a distal direction and the movement of the diffusion front in a proximal direction will lead to further elevated Sacin. As expected, Sacin was more closely associated with LCI in advanced disease. In severe disease, spirometric lung volumes and forced expiratory flows are also markedly reduced due to gas trapping and because poorly ventilated regions can no longer be compensated for by increased flow through non-flow-limited distal airways.28
Despite abnormal FEV1, one patient presented with normal LCI and Sacin but with highly elevated Scond. In children with asthma, Gustafsson29 has previously shown a more profound involvement of the small conductive airways, represented by markedly elevated Scond, in comparison with the other VI indices. In asthma, Scond is thus a more sensitive MBW index than LCI. The present finding could therefore be due to the presence of underlying (undiagnosed) asthma. Further studies in patients with PCD assessing bronchodilator response are consequently warranted. However, we believe that raised Scond reflects a similar patchiness of disease distribution among lung units as in asthma. The finding of markedly abnormal Sacin values in the majority of the patients with PCD suggests that PCD airway disease generally involves more peripherally located airway generations than asthma and that, in this respect, PCD resembles CF more than asthma.
In our study three patients did not have a conclusive abnormal ciliary beat pattern and frequency. Ciliary beat pattern and frequency and EM analysis play a key role in diagnosis, but PCD is likely to include a small number of phenotypes that may be manifested by subtle or no apparent structural defects and ciliary dysfunction. Consequently, studies have documented the occurrence of normal ciliary structure30–32 and function30 in patients with verified PCD. All three patients had abnormal MBW parameters while FEV1 and FVC were within the normal range (see table E3 in online supplement).
Limitations of the study
One limitation of our study is the lack of Danish MBW reference material. Instead, we used Swedish normative data as reference which were obtained using exactly the same equipment, software and procedures. In addition, the authors performing and calculating MBW tests have undergone training and have been under continual supervision by the Swedish laboratory in order to affirm the quality of the measurements.
MBW changes in PCD might reflect retained mucus in the airways resulting in VI. If so, MBW measures could improve following coughing, airway clearance manoeuvres or aerobic exercise. This study would be strengthened with additional information about variability in MBW measures in PCD, such as day-to-day variability, morning versus afternoon variability, before and after controlled coughs or before and after airway clearance manoeuvre. Furthers studies on these important methodological aspects are needed.
Abnormalities of peripheral airway function might reflect potentially reversible PCD lung pathology. Owing to their sensitivity to peripheral airway dysfunction, MBW tests have the potential to be used to signal the need for and to monitor the effects of early intervention and more aggressive treatment with the aim of preventing irreversible lung damage. As PCD is associated with a progressive and continuous impact on both physical and mental health,33 identification of children with early lung damage could lead to earlier and more aggressive intervention and, consequently, a better prognosis and quality of life over time.
In conclusion, our study demonstrates for the first time that MBW measures of peripheral airway function are abnormal in young patients with PCD, being far more frequent findings than abnormal spirometry. The study shows that PCD lung disease is characterised by marked peripheral dysfunction and that MBW is a promising and feasible method for early detection of airway disease in PCD. Further prospective controlled longitudinal studies assessing the utility of MBW in the management of PCD and their importance for long-term outcome are warranted.
Acknowledgments
The authors thank members of the staff at the Danish PCD Center and Pediatric Pulmonary Service at Copenhagen University Hospital and the families who participated in the study.
References
Supplementary materials
Supplementary Data
This web only file has been produced by the BMJ Publishing Group from an electronic file supplied by the author(s) and has not been edited for content.
Files in this Data Supplement:
- Download Supplementary Data (PDF) - Manuscript file of format pdf
- Download Supplementary Data (PDF) - Manuscript file of format pdf
- Download Supplementary Data (PDF) - Manuscript file of format pdf
- Download Supplementary Data (PDF) - Manuscript file of format pdf
Footnotes
Funding This study has been funded by The John and Birthe Meyer Foundation, Queen Louise Children's Hospital Research Trust and Aase and Ejnar Danielsen Foundation.
Competing interests None.
Ethics approval Ethics approval was provided by the Danish National Committee on Biomedical Research Ethics.
Provenance and peer review Not commissioned; externally peer reviewed.