Article Text

Abstract
Background Patients with chronic obstructive pulmonary disease (COPD) who are not severely hypoxaemic at rest may experience significant breathlessness on exertion, and ambulatory oxygen is often prescribed in this circumstance despite a lack of conclusive evidence for benefit. This study aimed to determine whether such patients benefit from domiciliary ambulatory oxygen and, if so, which factors may be associated with benefit.
Methods This was a 12 week, parallel, double-blinded, randomised, placebo-controlled trial of cylinder air versus cylinder oxygen, provided at 6 l/min intranasally, for use during any activity provoking breathlessness. Patients underwent baseline measurements of arterial blood gases and lung function. Outcome measures assessed dyspnoea, health-related quality of life, mood disturbance, functional status and cylinder utilisation. Data were analysed on an intention-to-treat basis, p≤0.05.
Results 143 subjects (44 female), mean±SD age 71.8±9.8 years, forced expiratory volume in 1 s (FEV1)1.16±0.51 lites, Pao2 9.5±1.1 kPa (71.4±8.5 mm Hg) were randomised, including 50 patients with exertional desaturation to ≤88%. No significant differences in any outcome were found between groups receiving air or oxygen. Statistically significant but clinically small improvements in dyspnoea and depression were observed in the whole study group over the 12 weeks of the study.
Conclusion In breathless patients with COPD who do not have severe resting hypoxaemia, domiciliary ambulatory oxygen confers no benefits in terms of dyspnoea, quality of life or function. Exertional desaturation is not predictive of outcome. Intranasal gas (either air or oxygen) may provide a placebo benefit.
Clinical trial number ACTRN12605000457640.
- Oxygen therapy
- chronic obstructive pulmonary disease
- ambulatory oxygen
- ambulatory oxygen therapy
Statistics from Altmetric.com
Introduction
Chronic obstructive pulmonary disease (COPD) is a leading cause of disability and death globally, characterised by progressive breathlessness, loss of function and, in its later stages, chronic hypoxaemia. Correction of hypoxaemia with long-term continuous oxygen therapy increases life expectancy and is a mainstay of treatment.1 2
Many patients with COPD, without resting hypoxaemia, experience significant breathlessness on exertion and, in some cases, ambulatory oxygen is prescribed. Such prescription is usually contingent upon demonstration of both relief of exertional desaturation and symptomatic benefit during a laboratory-based test. However, improvements in exercise capacity and dyspnoea with supplemental oxygen may also be observed in patients who do not desaturate on exertion3 4 and are hypothesised to result from reduced dynamic hyperinflation.5 6
Although studies in the clinic or laboratory setting have demonstrated modest increments in exercise capacity with supplemental oxygen, the use of domiciliary ambulatory oxygen is not strongly evidence based.7 Studies designed to examine its use have conflicting findings and are limited by small sample sizes.8–13 Lilker et al reported no change in dyspnoea, subjective assessment of activity or distance walked per day in nine patients with resting hypoxaemia randomised to air or oxygen in a 10 week crossover study,8 and Lacasse et al reported no impact on health-related quality of life (HRQoL) or exercise tolerance in a study comparing additional ambulatory air or oxygen in patients on long-term continuous oxygen therapy.9 Nonoyama et al reported no improvement in HRQoL after ambulatory oxygen compared with air in 27 patients with exertional desaturation over three pairs of 2 week treatments.10 Sandland and colleagues demonstrated no improvements over 8 weeks in physical activity levels, HRQoL or time away from home with oxygen versus air in 20 patients following completion of pulmonary rehabilitation.11
McDonald et al examined 26 patients, some with exertional desaturation, in a 6 week crossover trial of ambulatory air and oxygen, and found a statistically significant but clinically small improvement in exercise capacity after oxygen compared with air, but no difference in HRQoL.12 In contrast, in a study of 41 patients with COPD and exertional desaturation, Eaton et al reported no difference in exercise capacity or dyspnoea after oxygen compared with air, but statistically significant, albeit clinically small, improvements in HRQoL, anxiety and depression.13
Given the limitations and differing results of these previous studies, our aim was to perform a large, adequately powered study to determine the effects of domiciliary ambulatory oxygen in patients with COPD and exertional dyspnoea, without severe resting hypoxaemia; with or without exercise desaturation. The primary outcome measure was dyspnoea. Secondary outcomes were HRQoL, mood disturbance, functional status and gas utilisation. A further aim was to identify factors which might predict any observed benefit.
Methods
Design
Following research ethics approval this prospective, parallel, double-blinded, randomised controlled trial recruited patients with COPD and assigned them randomly to cylinder air or cylinder oxygen using a computer-generated sequence and concealed allocation. Study personnel and participants were blinded to group allocation. Cylinders were of identical appearance, weighed 4.2 kg filled, were provided with a trolley/stroller and delivered gas at a flow rate of 6 l/min via the Impulse Elite conservation device (AirSep Corporation, Buffalo, New York, USA). Verbal and written instructions required patients to use cylinders inside and outside the home during exertional activities that induced breathlessness. No recommendations were provided regarding duration of use, activity or exercise. Written instructions were provided regarding cylinder use and replacement procedures.
Participants
Clinically stable ex-smokers with COPD on optimal medical treatment, having Pao2 >7.3 kPa at rest breathing room air and moderate to severe exertional dyspnoea (Medical Research Council Dyspnoea Scale grade ≥314), were recruited through database screening and advertisement. Exclusion criteria were current participation in a Pulmonary Rehabilitation Programme, current domiciliary oxygen use, significant communication or locomotor difficulties, or other severe medical conditions. Patients with Paco2 >6.0 kPa underwent repeat arterial blood gas analysis after breathing oxygen at 6 l/min, at rest, for 30 min, and were excluded if Paco2 increased by more than 0.7 kPa.
Procedures
Arterial blood gases, pulmonary function tests and dyspnoea rating on both the Baseline Dyspnoea Index and the Medical Research Council scales were measured at trial entry only. Pulmonary function tests were performed according to American Thoracic Society guidelines15 16 using the SensorMedics Vmax Series Lung Function System (SensorMedics Corporation, Yorba Linda, California, USA), and validated predicted values for spirometry,17 transfer factor18 and thoracic gas volumes.19 Volume response to hyperoxia was determined by measuring the difference between resting inspiratory capacity breathing 21% oxygen and 44% oxygen.20
Following a 2 week run-in period to confirm clinical stability, all other assessments were performed prior to randomisation. This test battery was repeated 4 weeks (mid-trial) and 12 weeks later (end-study). Dyspnoea was assessed using the dyspnoea domain of the Chronic Respiratory Disease Questionnaire (CRDQ)21 and the Baseline/Transition Dyspnoea Index (BDI/TDI).22 HRQoL was examined using the CRDQ total score21 and the Assessment of Quality of Life Utility Index (AQoL)23 and mood disturbance using the Hospital Anxiety and Depression Scale (HADS).24 Functional capacity was measured using standardised tests of 6 min walk distance (6MWD) breathing cylinder air in a single-blinded manner.25 Functional performance was measured objectively using the activity count from a waist-mounted pedometer (Yamax Digiwalker, model SW-700, Yamax Corporation, Tokyo, Japan) and subjectively from diary-reported time spent outside the home and time spent standing or walking.26 Gas utilisation was expressed as number of cylinders used (calculated from gas pressure in returned cylinders) and as hours of use from self-reported diary data.
Sample size
Power calculations determined that 154 participants were required to provide a power of 0.8, at an α level of 0.05, to detect the minimal important difference (MID) in the primary outcome measure, the dyspnoea domain of the CRDQ, of 2.5 units,27 allowing for 20% attrition. Sample sizes of 142 and 130 participants, respectively, were determined to be required with regard to CRDQ total score (MID of 10 units27) and 6MWD (MID of 54 m28).
Analyses
Level of statistical significance was set at p≤0.05. Demographic data were compared using χ2 or t tests. Intention-to-treat analyses were performed. TDI scores and cylinder utilisation data were analysed using t tests to compare treatment means at weeks 4 and 12 postrandomisation. Other outcome measures were analysed using two-way, repeated measure analysis of variance, with treatment allocation and time as the two explanatory variables.
Variables selected a priori to identify subgroups which might benefit differentially from domiciliary ambulatory oxygen were exertional desaturation,25 severity of airflow obstruction, gender, severity of dyspnoea,29 and volume5 or exercise28 response to hyperoxia. Data were analysed using analysis of covariance (ANCOVA), with week 12 values as the response variable, the corresponding value at baseline as the covariate and each of the subgroup variables as an explanatory factor, in addition to treatment (air or oxygen). All ANCOVA models initially included an interaction term between the subgroup variable and the treatment, but these were omitted if found to be not statistically significant (p>0.05). In most cases the analysis was repeated after a small number of extreme outliers was omitted. Omission of the outliers did not change the outcome of the test (p≤0.05 or p>0.05). and only the results with the outliers omitted are presented.
Results
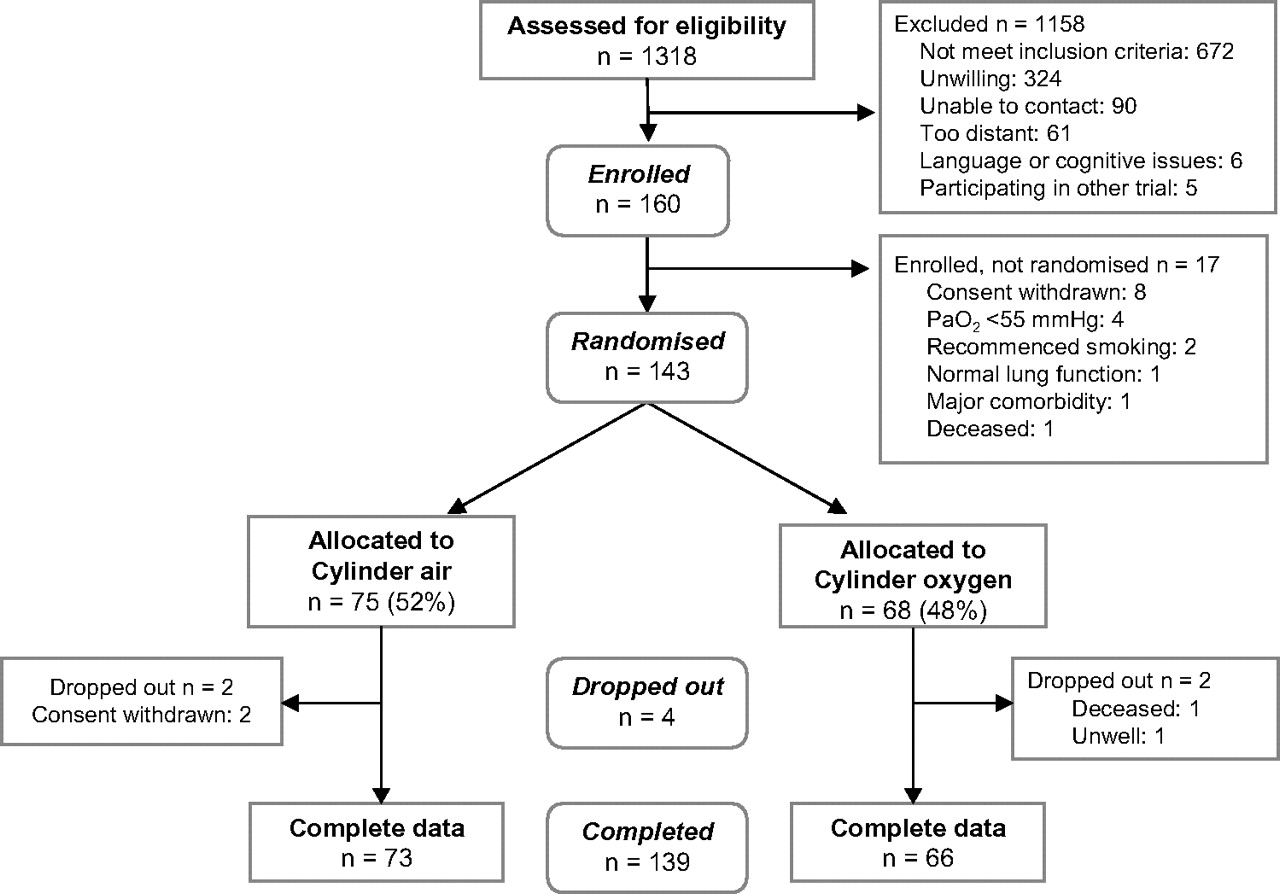
Of 160 patients enrolled, 143 (44 females) proceeded to randomisation and 139 completed the study (figure 1). Patients had moderate to severe COPD (FEV1 mean±SD 1.16±0.51 litres). With the exception of a statistically significant but clinically small difference in transfer factor, there were no significant differences between air and oxygen groups at baseline (table 1). Exertional desaturation was demonstrated in 35% of participants (table 1). At baseline, there was a statistically significant but clinically trivial acute improvement in 6MWD for the group as a whole when breathing cylinder oxygen (mean increase±SD, compared with 6MWD using cylinder air, 10.7±38.7 m, p=0.001). This increase was not significantly greater for the subgroup of desaturators as a whole (13.8±28.4 m, p<0.001), compared with the total group (p=0.596).
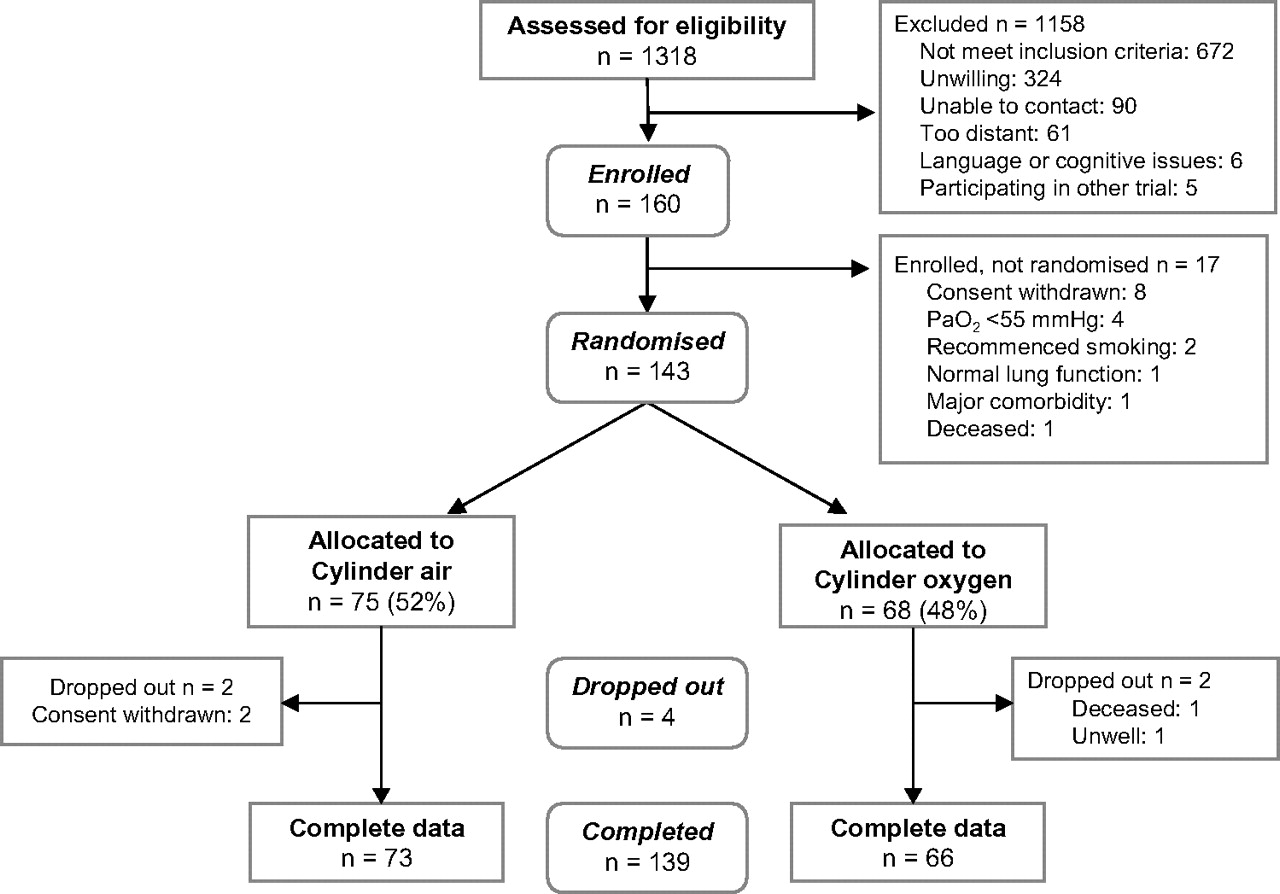
Flow diagram showing the number of subjects screened, enrolled and who completed the study.
Demographic data for treatment groups
Data are presented as mean (SD) for all variables except exertional desaturation, where number (percentage) of cases within each group is reported. Similarly, observed p values for t tests comparing group means are reported for all variables except exertional desaturation where the χ2 comparing proportions is presented. Exertional desaturation was defined as SpO2≤88% at the end of a 6 min walk test (6MWT) breathing cylinder air.
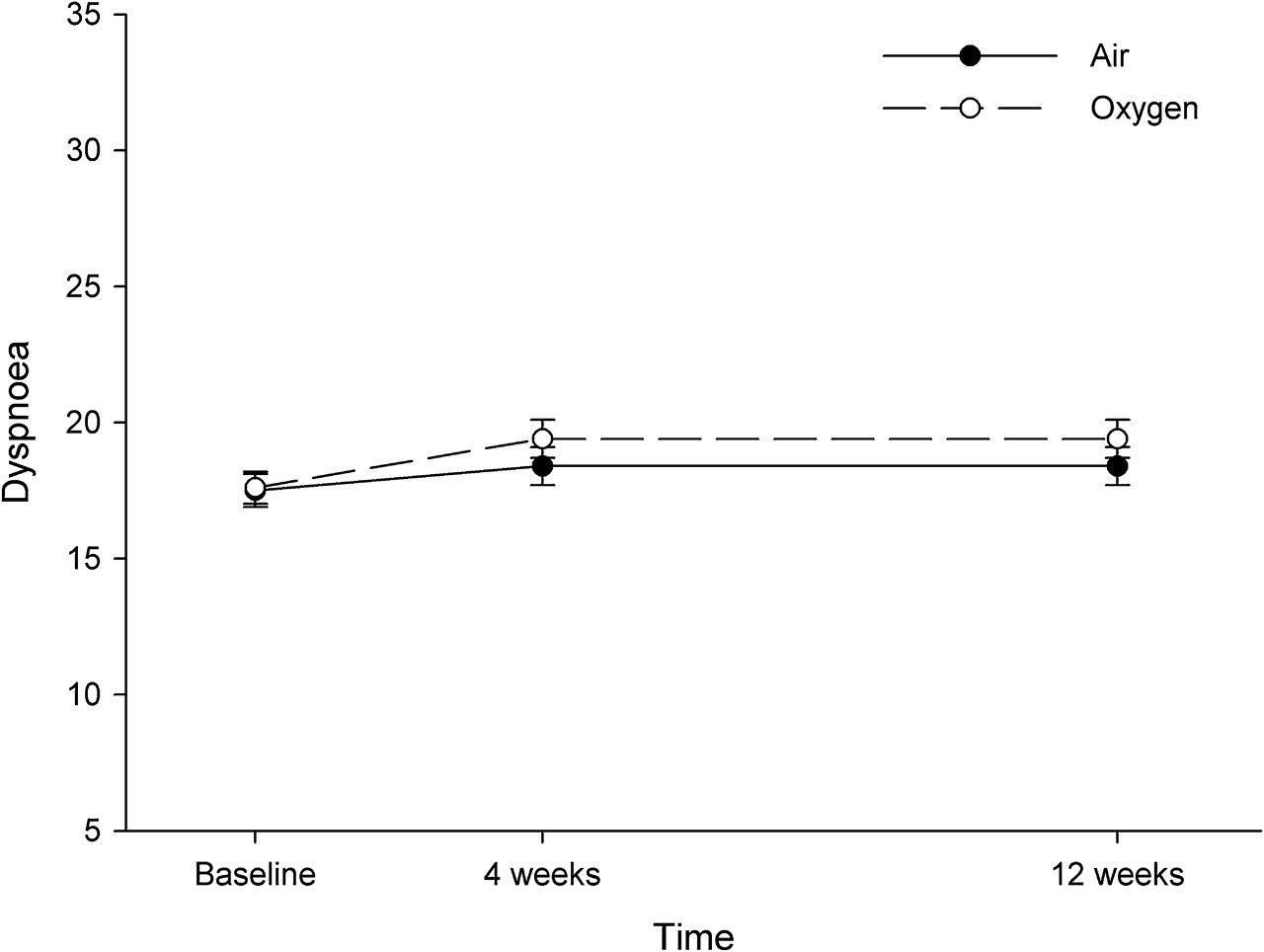
No significant differences were found between air and oxygen groups for CRDQ dyspnoea (figure 2), HRQoL or the functional outcome measures over the time of the study (tables 2 and 3). There were no differences between groups for TDI scores at either week 4 or week 12 (p=0.5 and 0.7, respectively).

{kind=link}
{kind=link}
Effect of treatment on dyspnoea.
Quality of life and mood outcomes
Functional capacity and performance outcomes
In participants overall, statistically significant improvements (mean, 95% CIs) were found over the study period for CRDQ dyspnoea scores (1.3, 0.6 to 2.1) and HADS depression scores (0.6, 1.0 to 0.2). The TDI demonstrated no significant change in dyspnoea in participants overall at week 4 (0.4, 0.1 to 0.6) or week 12 (0.3, −0.1 to 0.6).
The mean±SD number of cylinders used over 12 weeks was 8.0±8.9, and 82.6% of participants used ≤12 cylinders. There were no significant differences between air and oxygen groups for mean number of cylinders used (air group 7.2, oxygen group 8.9, p=0.245) or for self-reported hours of use at week 4 (p=0.445) or at week 12 (p=0.697). A survey of participants at study completion found that 46% of the oxygen group and 45% of the air group would have preferred to cease using cylinders altogether, and an additional three (air group) were undecided (p=0.254). Only 38 participants (28%) reported that their cylinders helped their breathing, and 62 (50%) reported difficulties with the apparatus including poor portability and difficulty changing the regulator.
Although no overall differences were observed between the air and oxygen groups, analyses were performed to examine whether participants with particular baseline characteristics may have been more sensitive to any benefit from oxygen. These analyses, summarised in table 4, showed that any improvement in the dyspnoea domain of the CRDQ that may have been attributable to oxygen was not predicted by exertional desaturation, severity of airflow obstruction or dyspnoea, volume or exercise response to hyperoxia or gender (p>0.05 in all cases) (table 4).
Baseline variables which were examined to determine if there was a differential benefit from ambulatory oxygen compared with ambulatory air
The secondary outcome measures, CRDQ total score, outings time, pedometer count, stand/walk time, 6MWD on cylinder air, AQoL Utility Index, HADS-anxiety and HADS-depression scores were similarly analysed. From the 64 such analyses carried out, a statistically significant interaction between the treatment and one of the subgroup factors was observed in four cases. These were: interaction between treatment and severity of airflow obstruction (p=0.016) and between treatment and exercise response to hyperoxia (p=0.027) for the (log-transformed) pedometer count, interaction between treatment and exercise response to hyperoxia for the (square-root transformed) HADS-anxiety score (p=0.003) and interaction between treatment and level of desaturation (p=0.047) for the AQoL Utility Index.
Discussion
This is the largest reported parallel, double-blinded, randomised controlled study of the effects of domiciliary ambulatory oxygen in patients with COPD and significant exertional breathlessness. Just over one-third of patients desaturated to ≤88% with exertion. Although, as in previous studies, there were small acute improvements in exercise capacity with oxygen compared with air during initial in-laboratory tests, these improvements fell far short of the 35–54 m, described as the MID for the 6MWT.28 30 We found no improvement in dyspnoea, HRQoL, functional capacity or performance with domiciliary use of cylinder oxygen compared with cylinder air, no difference in gas usage between groups and no factors which were predictive of benefit in any subgroup overall.
We observed statistically significant improvements in CRDQ dyspnoea score and depression in participants during the study regardless of which gas they received. These changes were less than those accepted to be of clinical importance and are similar to those reported by Nonoyama et al.10 They suggest either a benefit from nasal gas insufflation, regardless of whether it is with air or oxygen, or a placebo effect.
Four of the ANCOVA results in the current study suggested an interaction between baseline factors and treatment. However, three of these results lack biological plausibility. Participants who had more severe airflow limitation performed worse with oxygen, and those able to increase their 6MWD with oxygen at baseline had a lower pedometer count and were more anxious when randomised to receive oxygen during the study. In contrast, the significant interaction between treatment and baseline exertional desaturation for the AQoL Utility Index suggested a potential benefit in the subgroup of ‘desaturators’ randomised to oxygen. Although this last result is consistent with the findings of a previous study,13 no main effect for treatment or subgroup was observed for any of the analyses of the CRDQ dyspnoea score, the primary outcome of the study (tables 2 and 4). Additionally, all other domains of the CRDQ and the CRDQ total score, a disease-specific HRQoL measure, showed no benefit from oxygen. Analysis of the results of the current study did not include any correction for multiple testing and thus the statistically significant interactions should be interpreted with caution.
The mean use of eight cylinders over 12 weeks represents an average of 40 min of gas use per day, which is comparable with that in previous studies where outcomes were remarkably consistent despite differences in apparatus used.8–10 Fifty per cent of participants reported difficulties with their apparatus, suggesting perhaps that any perceived benefits from using the gas were outweighed by negative factors relating to cylinder usage. Other reported barriers to use included fear of dependence (5 participants), embarrassment (5 participants) and an inability to change the regulator (5 participants).
The underlying mechanisms for dyspnoea and exercise limitation in COPD are complex, and improvements in exercise performance and dyspnoea with hyperoxia are probably multifactorial, relating to altered perception of dyspnoea, reduced ventilatory demand, improved respiratory and peripheral muscle function and possible cardiovascular effects.6 We chose dyspnoea rather than exertional desaturation as our main inclusion criterion in order to explore mechanisms other than relief of hypoxaemia which may explain improvements in dyspnoea with ambulatory oxygen. Our finding that exertional desaturation was not predictive of benefit is important given that this frequently forms the basis for ambulatory oxygen prescription, despite previous studies suggesting that the degree of exercise desaturation does not predict benefit.12 31 Our finding of a significant interaction between treatment and level of desaturation for the AQoL Utility Index may arguably temper the strength of our findings, but this may also represent a type 1 error. Importantly, no effect on disease-specific HRQoL was observed. It remains possible that there may have been too few people in our subgroup of ‘desaturators’ to detect a benefit from ambulatory oxygen. However, this subpopulation of 50 subjects represents a greater number of ‘desaturators’ than were present in either of the two previous studies which specifically examined this question10 13 and which also failed to show a convincing benefit from oxygen therapy.
Hyperoxia is believed to reduce dyspnoea during exercise by reducing ventilatory demand and delaying the onset of dynamic hyperinflation. Previous studies suggest that this may occur in a dose-dependent fashion, up to a fraction of inspired oxygen of 0.5 or a flow of 6 l/min of 100% oxygen.4 We chose a flow rate of 6 l/min in order to maximise this effect and because the lower flow rates used in previous studies may have provided inadequate relief from exercise-induced desaturation.8–10
Our study has limitations, some of which relate to all such studies using currently available portable or ambulatory apparatus. The filled cylinder weight of 4.2 kg, which was necessary to ensure adequacy of oxygen supply using a flow rate of 6 l/min, may have discouraged use in breathless patients, despite their being supplied with a trolley. Lighter weight systems might provide greater ease of carriage but have the disadvantage of requiring more frequent replacement or filling. The high flow rate may have proved a disincentive to use through drying or discomfort at the nares; however, no patients complained specifically of this issue. Confining this study only to patients who desaturated may have yielded different results. However, this seems unlikely given the similar negative results in studies by Nonoyama et al10 and to a lesser extent Eaton et al,13 both of which were confined to patients who desaturated with exertion, as well as the negative results in the study by Lacasse et al of even more severely hypoxaemic patients.9 Previous studies have demonstrated a lack of correlation between desaturation and acute benefit from supplemental oxygen and others have suggested alternative mechanisms for benefit from oxygen such as changes in operating lung volumes, hence our rationale for choosing breathlessness rather than desaturation as the criterion for entry to our study. We believe the results of the current study are applicable to breathless patients with COPD on maximal treatment, with or without exercise desaturation. They may not pertain to those with significant resting hypoxaemia fulfilling criteria for long-term oxygen therapy.
Conclusion
This randomised controlled trial found that domiciliary ambulatory oxygen provided no additional benefit over air in terms of dyspnoea, quality of life or function in patients with COPD experiencing exertional dyspnoea without severe resting hypoxaemia. Of six factors examined (gender, exertional desaturation, severity of airflow obstruction, severity of dyspnoea, volume or exercise response to hyperoxia), none was predictive of therapeutic benefit. Our findings do not support the use of domiciliary ambulatory oxygen as a treatment for dyspnoea in this group of patients and challenge the use of exertional desaturation as a primary criterion for its prescription. Our results were suggestive but not conclusive of placebo benefits from having domiciliary gas cylinders.
Acknowledgments
The authors wish to acknowledge and thank Anthony D'Aloisio, Jeremy Friedman, Nadia Gagliardi, Chrissie Risteski and Sherine Yousef for their assistance.
References
Supplementary materials
{kind=link}
{kind=link}
Footnotes
Funding National Health and Medical Research Council, Northern Clinical Research Centre, Victorian Tuberculosis and Lung Association, Austin Hospital Medical Research Foundation, Institute for Breathing and Sleep, Austin Hospital, Australia Finkel Foundation, Air Liquide, Boehringer Ingelheim.
Competing interests None.
Ethics approval This study was conducted with the approval of the Austin Hospital Medical Research Ethics Committee and the Northern Hospital Medical Research Ethics Committee.
Provenance and peer review Not commissioned; externally peer reviewed.
Linked Articles
- Airwaves