Article Text

Abstract
Over the past 30 years there has been an epidemic of both obesity and asthma in the western world. A large body of robust epidemiological data has linked obesity with the development and severity of asthma in both children and adults and weight reduction with improvements in asthma severity and symptoms. However, it remains unsettled whether this relationship is causal or confounded by some other factor(s) as mechanistic and physiological studies have produced heterogeneous and at times conflicting findings. This review examines the clinical and epidemiological relationship between obesity and asthma and the purported mechanisms that may link these two processes together.
Statistics from Altmetric.com
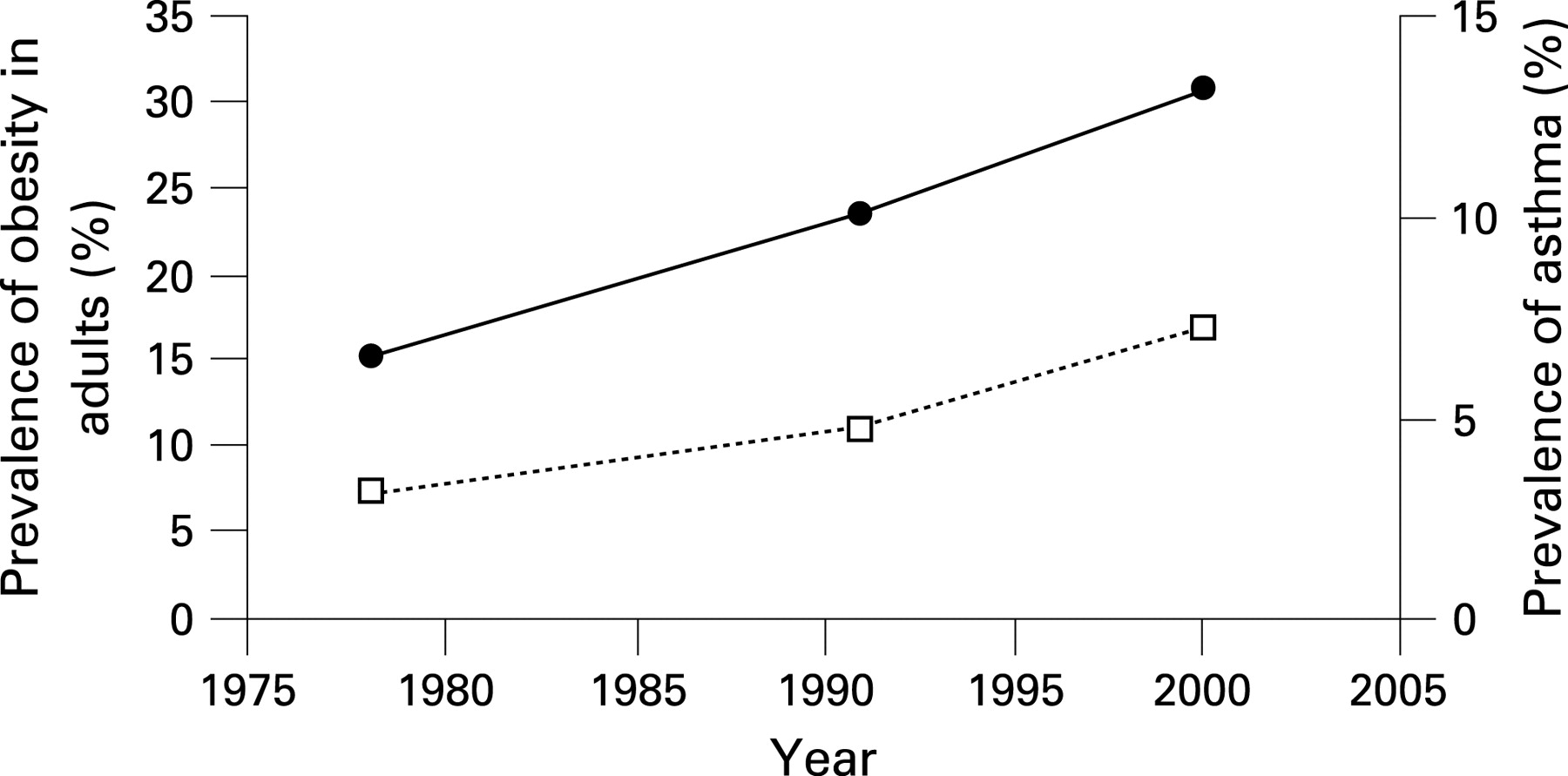
Globally, there is an epidemic of obesity with more than 1 billion overweight and 300 million obese adults worldwide.1 Obesity is also a major problem among children. In the USA alone there are 22 million children under 5 years of age who are overweight and, since 1980, the number of overweight children has doubled while the number of overweight adolescents has more than tripled.1 Concurrently, the prevalence of asthma has experienced a similar dramatic increase, with rates being nearly 2.5 times greater today than they were 20 years ago (fig 1).2 Whether this association is causal or coincidental remains unsettled, and a major challenge in understanding the nature of the relationship between obesity and asthma has been to determine whether obesity truly modifies asthma risk or phenotype or simply leads to a set of clinical and physiological perturbations that mimic asthma.
In this qualitative review we will critically examine the epidemiological data linking obesity with asthma and the purported mechanisms linking these two conditions. To identify relevant studies for this review, we searched PUBMED using key words “asthma” and “obesity”. This review will address a number of specific questions related to the asthma/obesity interaction which are currently being addressed by investigators worldwide, including:
Does obesity increase the risk of developing asthma?
If yes, by what mechanism(s)?
Is the effect of obesity primarily on asthma phenotype as it relates to severity or response to therapy?
Are the clinical and physiological abnormalities observed in many obese patients truly asthma or simply reflections of mechanical effects of increased body mass on the lungs?
While conclusive answers to these questions remain elusive, an enlarging body of work has begun to shed light on this important problem.
OBESITY AS A MODIFIER OF ASTHMA RISK
Numerous cross-sectional and case-control studies have shown a significant relationship between obesity and asthma, although there is variability in this literature with regard to how the diagnosis of asthma is ascertained (eg, based on historical data vs physiological characterisation).3–11 For instance, in a well performed case-control study from Sweden, Rönmark et al reported that obesity (defined as a body mass index (BMI) ⩾30 kg/m2) increased the odds of asthma (confirmed by bronchoprovocation testing) by 2.7-fold compared with normal body weight (BMI 20–24.9 kg/m2). The odds increased by 2.0 in overweight individuals (BMI 25–29.9 kg/m2), independent of age and sex.12 In a similar study, Young et al reported that being overweight increased the risk of asthma (defined by self-report and use of a bronchodilator or corticosteroids) by 40%, and obesity increased the risk by 2–3.8-fold.11 Cross-sectional studies have yielded similar results. For instance, Sin et al,13 using data from the Third National Health and Nutrition Examination Survey (NHANES III), demonstrated a dose-dependent relationship between self-report of asthma and BMI, independent of many confounding factors. However, case-control or cross-sectional studies are limited in that the directionality of the relationship cannot be determined and they are more susceptible to the introduction of bias.
A more robust method of determining causation in the relationship between obesity and asthma is through longitudinal cohort studies. Table 1 summarises the published longitudinal studies of asthma and obesity. Using data from the Nurses’ Health Study, Camargo et al14 prospectively evaluated the relationship between body weight and the incidence of self-reported physician-diagnosed asthma in women. As in the case-control studies, these investigators found a significant relationship between BMI and the incidence of asthma, with obesity increasing the asthma risk by 2.7–3.8-fold and overweight increasing the risk by 50–70%. More importantly, they showed that participants who reported weight gains of ⩾5 kg during a 4-year span experienced an increased risk of asthma in a dose-dependent manner.14 In the Danish Twin Registry Study, Thomsen et al15 reported that the incidence of new cases of self-reported asthma over 8 years was 4.3% in Danish adults aged 20–40 years, with a linear relationship between baseline BMI and incident asthma in both men and women. Interestingly, up to a BMI threshold of 31 the risk of asthma was always higher in women than in men, but beyond this threshold the risk of asthma increased exponentially in men but only linearly in women. Nystad et al,16 using data from a population-based study of 135 000 Norwegians who were followed for 21 years, found that on average for every one unit increase in BMI above 20 kg/m2 the risk of self-reported asthma increased by 10% in men and 7% in women. In addition to these examples, there have been several other longitudinal studies which have evaluated this relationship.16–21 Beuther and Sutherland performed a meta-analysis of these prospective epidemiological studies and reported that, in aggregate, these studies demonstrated a dose-dependent relationship between BMI and the incidence of asthma,22 with overweight increasing the odds of incident asthma by 38% (odds ratio (OR) 1.38 (95% confidence interval (CI) 1.17 to 1.62)) and obesity increasing the odds by 92% compared with normal body weight (OR 1.92 (95% CI 1.43 to 2.59)). In aggregate, while these findings suggest that overweight and obesity do increase the risk of developing asthma, the reliance in many of the cited studies on self-reported rather than physiologically-defined asthma leaves open the possibility that participants are experiencing respiratory symptoms for reasons other than asthma.
ANIMAL MODELS OF THE EFFECT OF OBESITY ON AIRWAY INFLAMMATION AND FUNCTION
The aforementioned observations from the epidemiological literature suggest a causal relationship between obesity and asthma, but these studies have been unable to shed significant light on potential mechanistic underpinnings. In attempts to evaluate relevant mechanisms, obese mice have been used to describe potential mechanisms by which obesity might modulate airway inflammation and/or function. Commonly studied are genetic models of obesity, including mice with genetic deficiencies in leptin production (ob/ob mouse) or the leptin receptor (db/db mouse), or deficiency in carboxypeptidase E production (Cpefat mouse). In each of these mouse models there is innate enhancement of airway hyper-responsiveness (AHR), as well as ozone or ovalbumin-induced airway inflammation (or sensitisation) and responsiveness that is greater than that observed in lean wild-type controls, suggesting that increased BMI in humans may predispose to AHR, a cardinal feature of asthma.23–26 However, although increased AHR is observed in obese mice, lung inflammation may not be the mechanism by which this occurs. A recent report by Johnston et al23 paradoxically showed fewer inflammatory cells (eg, eosinophils and lymphocytes) in the bronchoalveolar lavage fluid following ovalbumin sensitisation in obese compared with lean mice. Ozone exposure, on the other hand, consistently increased lung inflammation more in the obese mice than in the lean animals.24 Additionally, adipokines appear to play a prominent role in modulating the risk of asthma in animal models. Whereas leptin augments the inflammatory response in the lungs and increases bronchial responsiveness,27 adiponectin decreases lung inflammation and reduces bronchial responsiveness in mice.28
OBESITY, ATOPY AND AIRWAY INFLAMMATION IN HUMANS
A number of human studies have assessed the relationship between allergic and/or airway inflammation and obesity, a relationship that can be hypothesised in part because of the relationship between obesity, systemic inflammation and metabolic and cardiovascular disorders.29 Atopy is an important host factor in the development of asthma, and it has been hypothesised that obesity is associated with an increased likelihood of atopy. To evaluate this relationship, Huang et al studied 1459 eighth-grade students in Taiwan and found that there was a dose-dependent relationship between BMI and the risk of atopy in girls but not in boys.30 They also found that the prevalence of AHR increased with increasing BMI, but only in atopic girls, a finding which was later duplicated by Jang et al.31 There are, however, some dissenting studies. For example, von Mutius et al (using NHANES III data) failed to find a significant relationship between BMI and atopy among US children aged 3–14 years, although there was a significant relationship between BMI and asthma and between BMI and the use of asthma medications.32 Eneli et al found no significant relationship between allergy or hay fever and BMI.33 However, in children aged 7–14 years, Schachter et al34 found that the risk of atopy increased significantly with BMI only in girls but not in boys, but the relationship was fairly modest in magnitude. Obese girls were also more likely to be wheezy and to complain of a cough than lean girls. In boys the BMI made no difference to these symptoms.
With regard to airway inflammation, Todd et al35 studied induced sputum from 727 adults and found that BMI was not significantly associated with increased inflammation in the airways in individuals with or without asthma. McLachlan et al36 found that while exhaled nitric oxide levels were raised in those with asthma, there was no significant relationship between either BMI or percentage body fat and exhaled nitric oxide levels. Interestingly, in this study the investigators found that the risk of airflow obstruction and asthma were related to obesity in women but not in men, which could not be explained by differences in airway markers of inflammation.36
EFFECTS OF OBESITY ON PULMONARY PHYSIOLOGY
Obesity adversely impacts lung volumes and is associated with reductions in both forced vital capacity (FVC) and forced expiratory volume in 1 s (FEV1).37 The impact of obesity on lung volumes has been well studied by Jones and Nzekwu.38 They evaluated lung function tests in 373 individuals without lung disease and found that the greatest impact on expiratory reserve volume (ERV) was by raised BMI, with linear declines in ERV with increasing BMI. The ERV of individuals with BMI >40 kg/m2 was only 25% of predicted (fig 2). Vital capacity, total lung capacity, residual volume, and functional residual capacity also fell with increasing BMI, less so than ERV. The FEV1 to FVC ratio—a robust sign of airflow obstruction—did not change with increasing BMI, indicating that spirometric evidence of restriction (and not obstruction) is a characteristic physiological finding in obesity.

{kind=link}
{kind=link}
In obesity, reduced lung volumes lead to reduced peripheral airway diameter, a phenomenon which over time perturbs smooth muscle function,39 potentially increasing both airway obstruction and AHR. Despite this observation, the clinical data on obesity and AHR are conflicting. In a study of 11 277 participants in the European Community Respiratory Health Survey (ECRHS), AHR increased with increasing BMI in men but not women,40 and in a case-control study BMI was associated with the development of AHR.41 In contrast, Schachter et al showed that, in a group of 1971 adults, BMI was associated with a diagnosis of asthma and symptoms of dyspnoea and wheeze but was not associated with either airflow obstruction or AHR.42 Another study of 5984 children showed that obesity was associated with asthma symptoms and inhaler use but not AHR.43 Thus, while it is apparent that obesity leads to a number of physiological perturbations that could cause respiratory symptoms, physiological studies do not uniformly support the conclusions that obesity leads to airflow obstruction, AHR or asthma.
Medical and surgical studies of weight loss in individuals with asthma have provided an experimental model system to test the effects of weight loss on lung function and airway inflammation. These studies have shown that weight loss can lead to improvements in both clinical and physiological parameters. In an observational study of 14 obese patients with asthma before and after an 8-week very low calorie diet, weight loss reduced diurnal peak flow variability, increased functional residual capacity and improved measures of airflow limitation.44 In a similarly designed 6-month medical weight loss study of 58 obese women (24 of whom had asthma), weight loss improved FEV1 and FVC but did not affect AHR.45 Finally, in an experimental study of two groups of 19 patients with obesity and asthma, the group randomised to supervised medical weight loss had improved lung function, asthma symptoms and health status compared with controls.46 Similar observations have been made in studies of bariatric surgical patients; severely obese patients who received this surgery experienced improvements in both asthma symptoms and lung function, demonstrating an improvement of approximately 5% in FEV1 and 8% in FVC with a 22% reduction in body weight (from 115 to 89 kg). Interestingly, the exhaled nitric oxide concentrations did not change after surgery despite improvements in asthma control and lung function, suggesting that weight loss does not modify lung inflammation.47
ROLE OF SEX AND CO-MORBIDITIES IN THE OBESITY/ASTHMA RELATIONSHIP
It has been hypothesised that variables such as differential expression of sex hormones or body fat distribution may be important in the obesity/asthma relationship as some studies have suggested effect modification of this relationship by sex, with a greater risk of developing asthma in obese women than in obese men. In the ECRHS, Chinn et al48 found that the incidence of asthma over about 9 years of follow-up was approximately 70% higher in women than in men and 2.2 times higher in the obese subjects (BMI ⩾30 kg/m2) than in the non-obese participants. Importantly, whereas obesity was not associated with an increased incident risk of asthma in men, it was associated with a nearly threefold increase in the risk in women.48 Similarly, using data from the 1970 British Cohort Study, Shaheen et al9 showed that BMI was associated with an increased risk of asthma in women but not in men. Luder et al7 demonstrated that, in women, the prevalence of asthma was significantly increased in those with a BMI 25 kg/m2 or higher (BMI 25–27.5: OR 1.76; BMI 27.5–29.9: OR 2.45; BMI ⩾30: OR 2.67) compared with the reference category of BMI 22–24.9 kg/m2. In men the prevalence of asthma was increased in the lowest weight category, BMI <22 kg/m2 (OR 3.05) and in the highest category, BMI ⩾30 kg/m2 (OR 2.92, 95% CI 1.39 to 6.14). In one of the few studies to associate body fat distribution and asthma risk prospectively, Romieu et al showed that the transition from a leaner body silhouette to one that was progressively more android (suggesting predominantly abdominal fat distribution) was associated with a substantial increase in asthma risk.20 However, despite the suggestion of a differential risk in men and women arising out of individual studies, a meta-analysis by Beuther and Sutherland22 found that sex-dependent differences in the strength of the obesity/asthma relationship were abolished when multiple studies were analysed, with a similar effect of body weight on incident asthma in both men and women (OR 1.46 (95% CI 1.05 to 2.02) vs OR 1.68 (95% CI 1.45 to 1.94), p = 0.232 for the comparison). These conflicting data, combined with a need for more work in this area, leave unresolved the precise role of sex-specific variables in modulating the differential asthma risk in women compared with men.
Obesity increases the risk of both gastro-oesophageal reflux disease (GERD)49 and sleep disordered breathing (SDB), and at least two epidemiological investigations offer insight into the possible effects of these disorders on the obesity/asthma relationship. In a questionnaire study of over 16 000 participants in the ECRHS, Gunnbjornsdottir et al18 found that both self-reported GERD symptoms and self-reported asthma symptom onset increased in prevalence with increasing BMI. Despite this, when GERD was controlled for, obesity remained significantly related to the onset of asthma. To address the role of SDB in the obesity/asthma relationship, Sulit et al50 studied 788 children and found that, although both SDB and obesity were each independently associated with asthma and wheeze, adjustment for the effect of SDB did not modify the strength of the relationship between obesity and asthma. While there are still many unanswered questions about the interactions among these disorders, these two studies suggest that GERD and SDB do not fully account for the association between obesity and asthma.
From the standpoint of the practising physician, it can be challenging to determine whether respiratory symptoms in obese patients are due to co-morbid asthma or are simply due to altered respiratory mechanics as described above. In the obese patient in whom asthma is suspected, a detailed physiological evaluation which includes not just spirometry but also lung volumes and AHR is warranted to better define the nature and magnitude of the physiological impairment. In addition, alternative causes of dyspnoea related to obesity must be considered, including cardiovascular disease, systemic hypertension with attendant left ventricular diastolic dysfunction, pulmonary hypertension in the setting of obstructive sleep apnoea and/or obesity hypoventilation syndrome. It is also important to consider disorders that can mimic asthma (eg, vocal cord dysfunction), which are often treated with but are unresponsive to systemic glucocorticoids and which paradoxically cause additional weight gain.
EFFECT OF OBESITY ON ASTHMA SEVERITY AND RESPONSE TO TREATMENT
Studies of the effect of BMI on asthma phenotype typically require more careful characterisation than is feasible in large-scale epidemiological studies. Smaller cohorts of asthma patients have increased our understanding in this area, although more research on this aspect of the obesity/asthma relationship is needed. Tantisira et al51 analysed data from the Childhood Asthma Management Program in which the asthma phenotype of participants was characterised using impairment domains such as symptoms and lung function, as well as by objective testing for atopy and AHR. They reported the absence of a significant relationship between BMI and asthma control domains such as school absenteeism, emergency department care, requirement for corticosteroids or hospitalisations. While a weak relationship between BMI and exertional cough or wheeze was observed, BMI did not affect eosinophil counts or IgE concentrations and, although there was a weak inverse relationship between BMI and bronchodilator reversibility (β = −0.003, p = 0.02), there was no impact of BMI on AHR. The generalisability of these data is somewhat limited, however, by the observation that most participants were prepubertal and that the median BMI was 17.1 kg/m2.
It has been hypothesised that obesity is associated with a more severe asthma phenotype, an observation supported in part by data from the TENOR study of individuals with severe asthma, in which the mean BMI in adults was 30.4 kg/m2.52 However, a 2007 report from the Severe Asthma Research Program (SARP) investigators53 indicated that obesity was not more prevalent in severe54 than in moderate asthma, leading to questions about the role of obesity as a modifier of asthma severity. It is possible, however, that the effects of obesity on prevalent asthma are exerted either through co-morbid illnesses that are associated with asthma or through mechanical effects of obesity on pulmonary physiology.
In obesity, enhancement of normal adipose tissue immune function leads to a systemic inflammatory state,55 a phenomenon which is implicated in mediating the metabolic and cardiovascular complications of obesity.56 57 Interestingly, many of the cytokines found to be elevated in obesity-related systemic inflammation (eg, tumour necrosis factor α (TNFα) and interleukin 6 (IL6)) are also associated with the development of glucocorticoid insensitivity in asthma.58 As noted previously, much of the mechanistic literature evaluating the obesity/asthma relationship has focused on the role of leptin, which shares structural homology with IL6, regulates T cell proliferation and activation, and recruits and activates monocytes and macrophages.59 In mice, exogenous leptin has been shown to enhance AHR and increase serum IgE after inhaled ovalbumin challenge,27 suggesting that leptin may have an immunomodulatory role relevant to asthma.
It is not known if systemic inflammation in obesity leads to a reduction in glucocorticoid sensitivity. However, emerging data suggest that there is potential for an interrelationship between inflammation in obesity and glucocorticoid insensitivity in that production of proinflammatory cytokines seen in obesity (TNFα, IL6) are upregulated in lung macrophages from individuals with glucocorticoid-insensitive asthma,60 suggesting that the cytokine environment described in obesity may modify the therapeutic response to glucocorticoids. Two post hoc analyses of clinical trial data support this. Peters-Golden et al analysed data from four trials of montelukast and beclometasone and showed that the clinical response (defined by asthma control days) to beclometasone declined as BMI increased.61
It is also reasonable to speculate that the increased TNFα level in obesity may be relevant to the treatment of obese subjects with asthma. A recent clinical trial showed that the increased expression of membrane-bound TNFα, TNFα receptor 1 and TNFα converting enzyme in peripheral blood mononuclear cells from patients with severe asthma was associated with glucocorticoid insensitivity.54 This study also suggested a beneficial effect of the soluble TNFα receptor etanercept in these patients, as shown by improvements in AHR, FEV1 and asthma-related quality of life,62 raising the possibility that controller agents other than corticosteroids may be effective in obese individuals with asthma in whom systemic inflammation and glucocorticoid insensitivity are shown to be important factors.
OBESITY AND SYMPTOMS, HEALTH CARE AND DRUG UTILISATION
Obese individuals are not only at increased risk of asthma but also more symptomatic, require more asthma drugs and have an increased risk of emergency visits than do lean individuals once they develop asthma. For instance, Sin et al13 showed that a BMI of >31 kg/m2 increased the risk of asthma by 50%, the use of bronchodilators by 94% and dyspnoea by 2.7-fold compared with a normal BMI of 22–25 kg/m2. Interestingly, in this study the risk of airflow obstruction was no different between the two BMI categories, suggesting that obesity increases asthma symptoms and drug use but has little impact on airways obstruction. These data are consistent with those of Thomson et al63 who showed in a group of subjects with asthma treated in an emergency room that, while obese patients were more likely to be on anti-asthma drugs and had longer stays in the emergency room, they had better peak flows at the time of assessment than did normal weight subjects with asthma. In one of the largest studies to date, Rodrigo and Plaza64 showed that patients with increased BMI (mean 29 kg/m2) who presented to emergency rooms with acute exacerbations had higher FEV1 (% predicted) and peak flows but paradoxically were more symptomatic, taking more corticosteroids and oral theophyllines, and were more likely to be hospitalised than those with a normal BMI. Similar findings have been noted in other studies65 and also among children with asthma.66
SUMMARY AND CONCLUSIONS
Robust epidemiological data link obesity with an increased risk of asthma in the community. However, the exact mechanisms responsible for this relationship remain unknown. While animal studies have implicated inflammatory mechanisms as a potential culprit, human studies have not fully endorsed this concept. There is little doubt that obesity adversely impacts lung function, which improves with weight reduction through mechanical unloading, although more information is needed to improve our understanding of how and if obesity modifies phenotype in prevalent asthma. Obesity also increases symptoms and use of medications and health services including emergency rooms and hospitals. Reduction in weight (regardless of method) improves clinical outcomes and enhances lung function, but this is difficult to achieve and even more difficult to sustain.
As we wait for additional studies to further elucidate the relationship between obesity and asthma, the question remains about how best to integrate the current state of knowledge, particularly as it pertains to obese patients in whom the diagnosis of asthma is being considered. It seems reasonable to have heightened clinical suspicion for asthma in obese patients with respiratory symptoms. However, clinical history should be supplemented by careful physical examination and physiological characterisation with complete pulmonary function (not just spirometry) and bronchoprovocation testing to determine if characteristic asthma features such as bronchodilator-responsive expiratory airflow limitation and AHR are present. In addition, common co-morbid illnesses such as heart failure and obesity hypoventilation syndrome should be carefully ruled out. A potentially variable response to asthma treatments (particularly glucocorticoids) related to obesity must also be considered, recognising that a suboptimal response to treatment could also suggest an improper diagnosis. Studies suggest that weight loss reduces symptoms, although the resultant effects on physiological variables such as lung function and biomarkers of airway inflammation and AHR may vary by patient. Notwithstanding these recommendations, there is a pressing need to improve our understanding of the mechanisms underlying the relationship between obesity and asthma and to develop treatment strategies to improve health outcomes of obese patients with asthma.
REFERENCES
Footnotes
Funding: Grant support: Canada Research Chair (DDS); NIH HL090982 (ERS).
Competing interests: None.