Article Text

Abstract
Pulmonary lymphangioleiomyomatosis (LAM) is a rare disease that affects women in the reproductive years. It is occasionally associated with tuberous sclerosis, especially in the incomplete form. As it is likely that oestrogen plays a central role in disease progression, exogenous oestrogen will cause a deterioration in LAM. However, the early stage of this disease is easy to miss unless the physician is a specialist. Although there have been some reports in menopausal women given exogenous oestrogen for osteoporosis, this is the first report of pulmonary LAM caused by exogenous oestrogen used for the treatment of infertility.
- lymphangioleiomyomatosis (LAM)
- tuberous sclerosis complex
- exogenous oestrogen
Statistics from Altmetric.com
CASE REPORT
A 27 year old woman with progressive dyspnoea was referred to our hospital in December 2000 by a local doctor for further examination of an abnormal shadow seen on chest imaging. Hypomelanotic maculae on the abdominal skin, ungual fibroma of the bilateral digit pedis, and facial angiofibroma were observed. Although the details were not known, she had bilateral cystic kidneys 70 days after birth and was diagnosed as having tubular sclerosis. She had married in 1996 and, as she had not conceived after 2 years of marriage, treatment with an oral infertility drug (ethinylestradiol norgestrel; Duoluton) was started in August 1998.
Pulmonary symptoms appeared in 1999, 12 months after beginning the infertility treatment. She first noticed the dyspnoea when ascending the stairs or on a slope, and dyspnoea with bloody sputum progressed from July 2000.
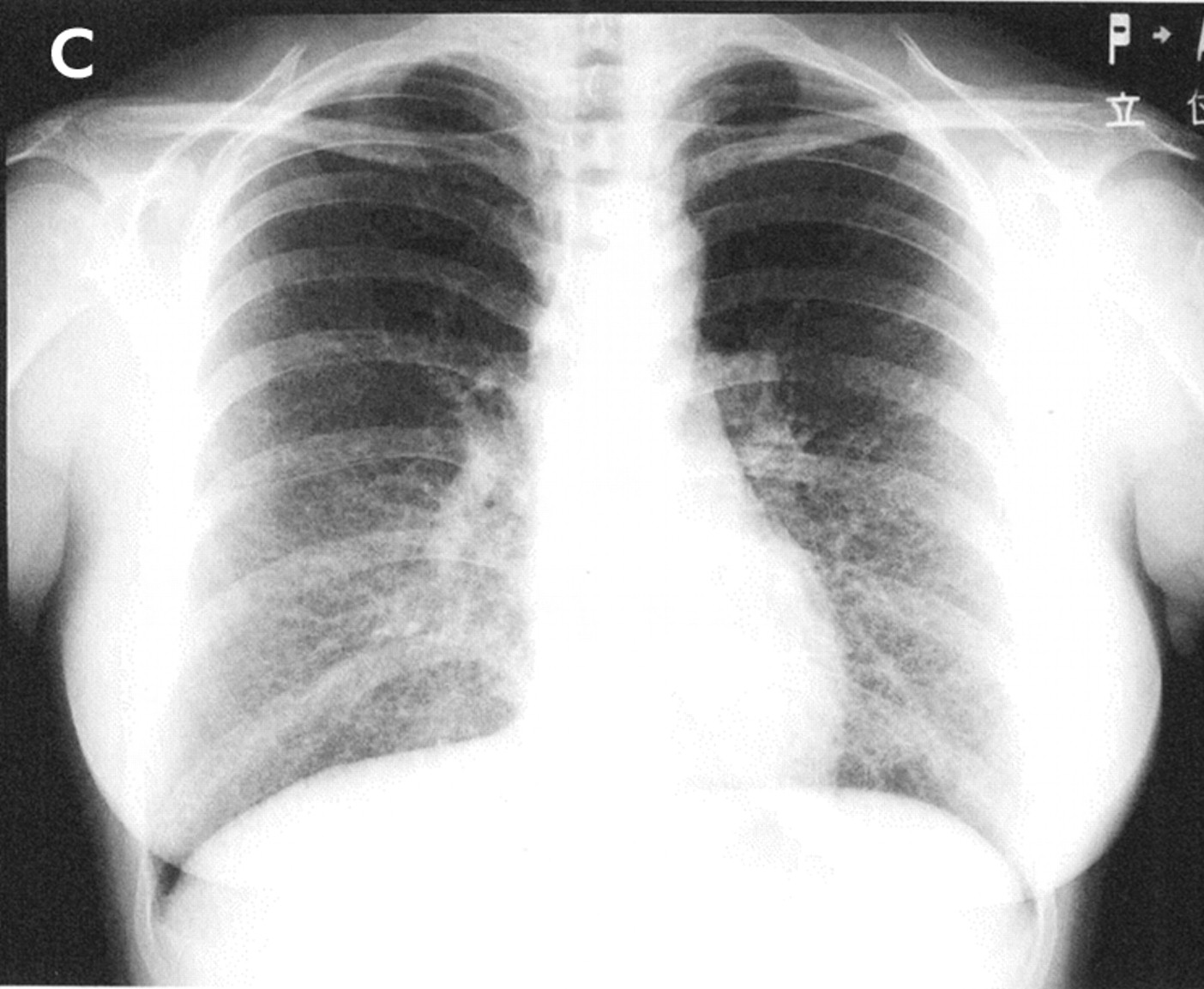
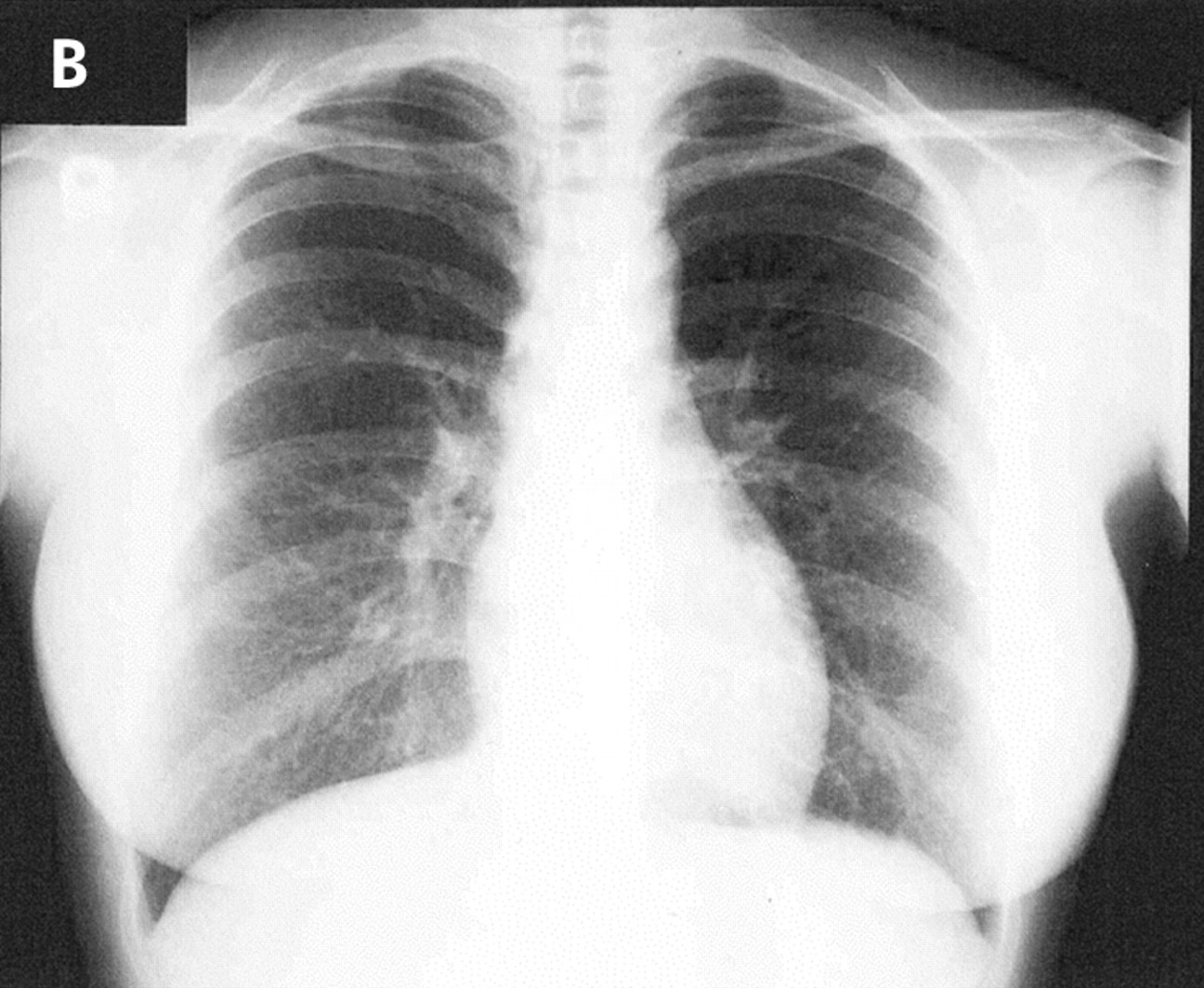
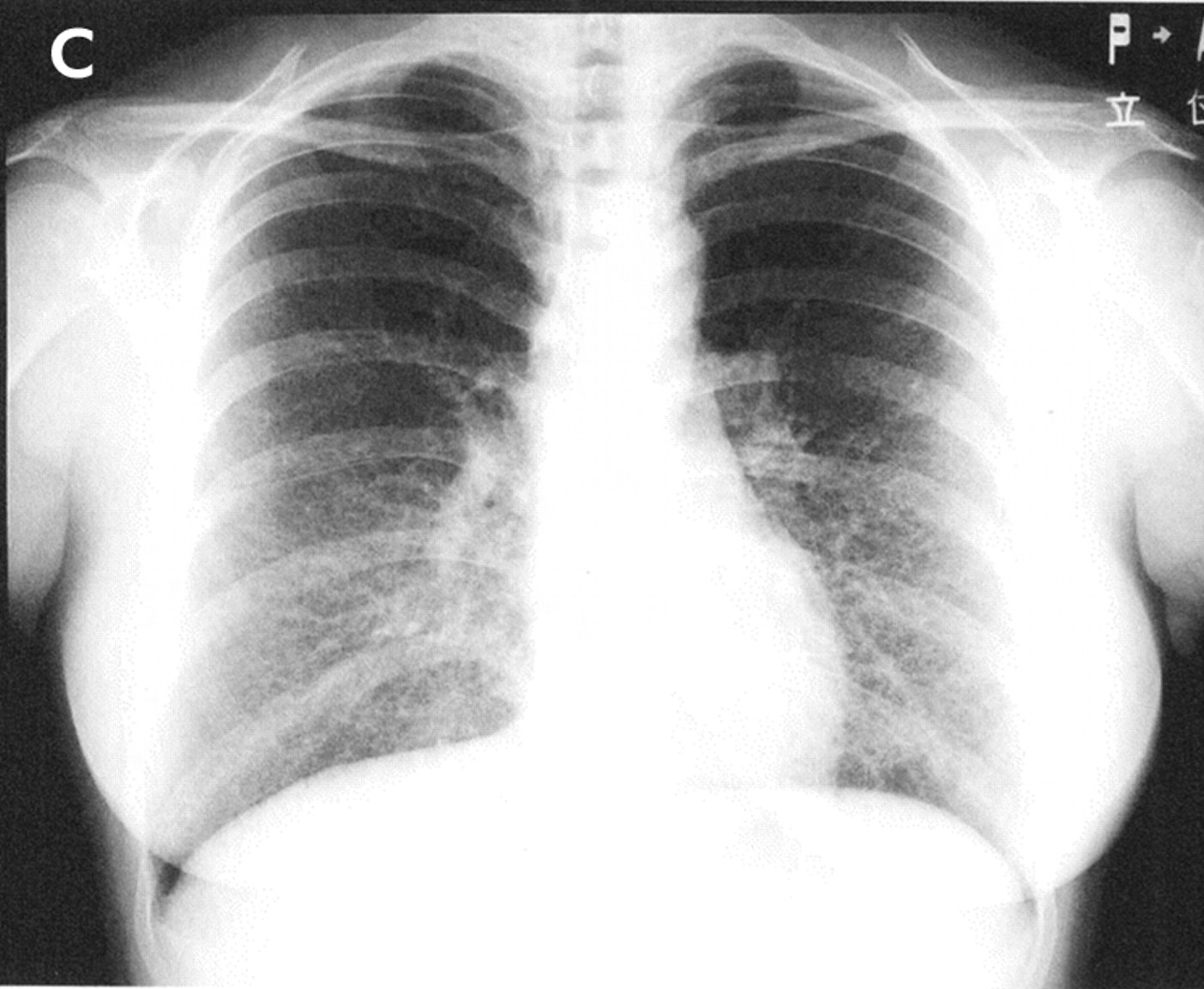
On admission the white blood cell count was raised to 11 100/mm3. Serum levels of angiotensin converting enzyme (ACE) were also raised (25.1 IU/l). Arterial blood gas analysis gave Pao2 10.9 kPa (81.6 mm Hg), Paco2 4.7 kPa (35.4 mm Hg), pH 7.40. The alveolar–arterial oxygen difference was 3.1 kPa (23.5 mm Hg). Routine bacteriological, fungal, and mycobacterial cultures of sputum were negative. A plain chest radiograph revealed diffuse fine reticulonodular shadowing (fig 1C) which showed a progression from that of 2 years earlier (fig 1A) and from the previous year (fig 1B). A CT scan of the chest showed diffuse multiple thin-walled cystic air spaces, CT scan of the bilateral kidneys showed multiple cysts, and a CT scan of the brain showed subependymal nodules. Spirometric tests gave forced expiratory volume in 1 second (FEV1) of 2.02 l (74.8% predicted), forced vital capacity (FVC) of 2.30 l (81.3% predicted), and FEV1/FVC ratio of 87.8%. A transbronchial biopsy specimen from right B4 showed hyperplasia of the smooth muscle at the alveolar wall and bronchiole, and deposition of haemosiderin and emphysema.


{kind=link}
{kind=link}
{kind=link}
(A) Chest radiograph in 1999 before infertility treatment. (B) Chest radiograph in 2000 one year after infertility treatment. (C) Chest radiograph at admission showing diffuse small nodular opacity.
Paraffin embedded transbronchial tissue sections were stained for oestrogen and progesterone receptors in accordance with the method of Logginidou et al.1 Immunoreactivity for both oestrogen and progesterone receptors and HMB45 were negative. The patient was discharged and followed at our outpatient clinic. The alveolar–arterial oxygen difference, respiratory function tests, and serum ACE levels had not improved 7 months after stopping Duoluton treatment.
DISCUSSION
We have reported a case showing exacerbation of pulmonary LAM resulting from administration of exogenous oestrogen for infertility. To our knowledge, this is the first case involving exogenous oestrogen administration for infertility, although there are several previous reports of pulmonary LAM in menopausal women being treated with exogenous oestrogen for osteoporosis.2–5
LAM is a rare disease that affects women, primarily during the reproductive years. It is characterised by non-neoplastic proliferation of atypical smooth muscle cells within the lung parenchyma and elsewhere, leading to progressive loss of lung function and, ultimately, death.6 Fewer than 1% of tuberous sclerosis cases are associated with pulmonary manifestations, and these are indistinguishable from those of LAM.7 Some have referred to LAM as a forme fruste of tuberous sclerosis.8,9 Mental retardation, seizures, and facial angiofibroma form a classic triad. Because the term “tuberous sclerosis” only refers to cerebral tubers, the term “tuberous sclerosis complex (TSC)” is preferred to stress multiorgan involvement.10 Antemortem diagnosis of TSC can be established by clinical or imaging features. The complete triad of tuberous sclerosis is not commonly present in those who develop pulmonary involvement.9 Although this patient had neither mental retardation nor seizures, she had hypomelanotic maculae on the abdominal skin, ungual fibroma of the bilateral digit pedis, and facial angiofibroma. Furthermore, CT scanning showed LAM in the chest, bilateral cystic kidneys, and subependymal nodules in the brain. We therefore diagnosed this case as TSC.
TSC has recently been shown to result from mutations in the tumour suppression genes TSC1 encoding hamartin on chromosome 9q34,11 and TSC2 encoding tuberin on chromosome 16p13.3.12
Franz et al13 showed in a prospective study that cystic and nodular pulmonary changes consistent with LAM are common in women with TSC. The absence of immunoreactivity for an oestrogen receptor suggests that the oestrogen receptor might be downregulated by exogenous oestrogen. Based on these observations, we conclude that LAM in tuberous sclerosis might differ in origin from sporadic LAM. Worsening of the reticulonodular shadow on the chest radiographs appeared after initiating treatment with Duoluton and gradually progressed thereafter. We could not determine whether this progression was due to the treatment or to tuberous sclerosis associated LAM itself. Seven months after stopping medication the alveolar–arterial oxygen difference and chest radiograph had not improved; we speculate that Duoluton directly promoted the pulmonary lesions. TSC is a hereditary disease and the presence of LAM should be considered before starting infertility treatment. In our patient tests for both oestrogen and progesterone receptors were negative. The patient was followed for 7 months without drugs.
We conclude that before giving exogenous oestrogen, especially for infertility treatment, the physician should confirm that the patient does not have a previous history of LAM in tuberous sclerosis.