Article Text

Abstract
Background: Patients with pulmonary hypertension develop intimal plaques in large pulmonary arteries.
Objective: To test the hypothesis that the composition of such plaques differs depending on whether the aetiology of the disease is thromboembolic or hypertensive.
Design: Chronic thromboembolic and plexogenic pulmonary hypertension (primary and secondary (Eisenmenger syndrome)) were investigated. These are spontaneous human models and were used to examine the independent role of thrombus and hypertension in plaque composition.
Setting: A national tertiary referral centre for lung transplantation and pulmonary thromboendoarterectomy.
Patients: Thirty nine patients with chronic thromboembolic pulmonary hypertension who had undergone thromboendoarterectomy (n = 32) or lung transplantation (n = 7), 28 with plexogenic diseases (nine primary and 19 Eisenmenger), and three with Eisenmenger syndrome complicated by thromboembolic events.
Interventions: The lung and thromboendoarterectomy samples were sectioned, stained with Movat pentachrome, and immunostained with antibodies for fibrin, platelets, inflammatory cells, smooth muscle cells, and erythrocyte membrane glycophorin A.
Main outcome measure: Composition of the plaques affecting large pulmonary arteries.
Results: Two types of intimal lesion were distinguished in chronic thromboembolic pulmonary hypertension: fibrous plaques with angioneogenesis; and core-rich atherosclerotic plaques with pultaceous cores largely consisting of glycophorin immunoreactive material, with cholesterol clefts (61.5%), CD68 positive macrophages (84.6%), T lymphocytes (87%), and calcification (46.1%). The samples from the patients with Eisenmenger syndrome and thromboembolic complications had similar characteristics, whereas those from patients with uncomplicated primary pulmonary hypertension had core-free fibrous plaques, spotted with macrophages and T lymphocytes.
Conclusions: Chronic thromboembolic pulmonary hypertension is associated with atherosclerotic plaques with glycophorin-rich pultaceous cores, and plexogenic pulmonary hypertension with fibrous plaques. Thromboembolic material thus plays a critical role in the formation of pultaceous cores, of which erythrocyte membrane derived glycophorin is a major component.
- pulmonary hypertension
- thrombosis
- glycophorin
- pultaceous core
Statistics from Altmetric.com
Both primary and secondary plexogenic pulmonary hypertension (Eisenmenger syndrome) are spontaneous in vivo models that are useful for investigating the role of hypertension in plaque formation and composition; chronic thromboembolic pulmonary hypertension is a unique model for investigating the corresponding role of thrombi.1–5 Both conditions generate proximal pulmonary artery plaques, the composition of which has not been specifically investigated. In plexogenic pulmonary hypertension plaques are mostly constituted of fibrous tissue, while in chronic thromboembolic pulmonary hypertension plaques may contain pultaceous cores, layers of organising/reabsorbing thrombolic material, and fibrous tissue.
Chronic thromboembolic pulmonary hypertension is usually characterised by a first thromboembolic event followed by the so called “honeymoon” asymptomatic phase, with possible further silent emboli, and finally the development of chronic hypertensive disease. At the time of the first thromboembolic episode, the pulmonary arteries are innocent bystanders.5 The current treatment for chronic thromboembolic pulmonary hypertension is pulmonary thromboendarterectomy, which removes recent and old thrombotic endoluminal material, neointima, and a few elastic lamellae from the inner layers of the tunica media of pulmonary arteries.6
We hypothesised that comparative studies of lung arteries from patients with plexogenic and chronic thromboembolic pulmonary hypertension would provide useful data for investigating the independent role of thrombi and hypertension in plaque formation, and that plaque composition is influenced by the different pathogeneses.
METHODS
We analysed the histopathological and immunohistochemical characteristics of the endoluminal material removed at pulmonary thromboendarterectomy from the pulmonary arteries of patients with chronic thromboembolic pulmonary hypertension, and from lungs excised at transplantation from patients with plexogenic or thromboembolic hypertensive pulmonary disease. All the patients underwent electrocardiography and echocardiography, invasive right and left ventricular haemodynamic examinations, coronary and pulmonary angiography, and routine biochemical analyses; any risk factors for atherosclerosis were investigated and recorded. None of the patients had associated ischaemic or other heart disease, and none of those who underwent pulmonary thromboendarterectomy needed any additional surgery.
Chronic thromboembolic pulmonary hypertension
There were 39 patients with chronic thromboembolic pulmonary hypertension (22 men, aged (mean (SD)) 43.2 (13.8) years, and 17 women, aged 54.7 (11.8) years). Of these, 32 underwent pulmonary thromboendarterectomy and seven underwent lung transplantation (performed before the introduction of the pulmonary thromboendarterectomy technique in our hospital). The time between the onset of the symptoms diagnosed as being caused by pulmonary hypertension and performance of surgery was 26 (42.6) months (range 6–264 months).
Plexogenic primary and secondary pulmonary hypertension
There were 31 patients with plexogenic primary and secondary pulmonary hypertension: nine with primary pulmonary hypertension (two men aged 19 years and seven women aged 43.6 (5.08) years); 19 with Eisenmenger syndrome (six men aged 27.8 (4.8) years and 13 women aged 36.6 (12.3)); and three with Eisenmenger syndrome complicated by thromboembolic events (two men aged 54.0 (4.2) years and one women aged 51 years).
The coronary artery trees of the 13 patients with Eisenmenger syndrome who underwent heart–lung transplantation (one of whom had thromboembolic complications) contained no atherosclerotic plaques on pathological examination.
None of the hearts from the patients with primary pulmonary hypertension was available for study because they were used in domino procedures.
Histopathological and immunohistochemical study
All the pulmonary thromboendarterectomy material and multiple arterial samples from transplanted lungs were fixed in 10% buffered formalin and embedded in paraffin. Multiple 5 μ thick sections were cut and stained with haematoxylineosin and Movat pentachrome stain.7 Further sections were used to investigate the immunohistochemical characteristics of the thrombus components using antibodies to platelets (anti-IIb/IIIa glycoprotein complex), fibrin and erythrocyte membrane derived material (antiglycophorin A), and plaque cells (inflammatory and non-inflammatory smooth muscle and endothelial cells) (table 1). The sections were immunostained by previously described methods using the avidin–biotin peroxidase complex and diaminobenzidine tetrahydrochloride as chromogen.7,8 The positive controls were sections of coronary artery samples with recent thrombotic occlusion (glycoprotein IIb/IIIa and fibrin), normal spleen (macrophages, lymphocytes, glycophorin A, endothelial cells), and large bowel (smooth muscle cells); the lung samples provided further internal positive controls. The negative controls were obtained by substituting primary antibody with normal swine serum or an unrelated primary antibody.
Antibodies and antisera used in the immunohistochemical study
The features that we specifically investigated were:
pultaceous material (lipid-rich, necrotic material)
cholesterol clefts
fibrous tissue and “neointimal hyperplasia” consisting of smooth muscle cells and loose matrix-rich extracellular collagen
organised/reabsorbed thrombotic material, defined by residual fibrin stands embedded in the neointimal fibrous tissue
“recent” non-organised thrombotic material
vascular neogenesis
inflammatory cells (macrophages, lymphocytes, foam and non-foam cells)
calcification.
Statistical analysis
Univariate and multivariate logistic models were used to compare atherogenic risk factors (age, blood cholesterol, triglyceride, and glucose concentrations, systolic and diastolic systemic blood pressure, and smoking) between the patients with plexogenic and chronic thromboembolic pulmonary hypertension, and between the patients with purely plexogenic pulmonary hypertension and those with chronic thromboembolic pulmonary hypertension or Eisenmenger syndrome with thromboembolic complications.
A paired t test was used to compare the risk factors for patients aged more or less than 60 years with atherosclerotic lesions in chronic thromboembolic pulmonary hypertension.
Further univariate and multivariate logistic models were used to assess the predictive value of factors that might contribute to the development of the recorded histopathological features: the clinical and pathological diagnosis of chronic thromboembolic pulmonary hypertension, age, systolic, diastolic, and mean pulmonary artery pressure, pulmonary vascular resistance, and time between the onset of severe symptoms (New York Heart Association functional class III/IV) and surgery. A probability (p) value of 0.05 was considered significant.
RESULTS
Intimal plaques were found in the proximal pulmonary arteries of all the patients with severe pulmonary hypertension. In the patients with chronic thromboembolic pulmonary hypertension and plexogenic hypertension complicated by thromboembolism, part of the plaques contained pultaceous cores consisting largely of glycophorin immunoreactive material, indicating the major contribution of red cell membranes to their formation. In the patients with plexogenic pulmonary hypertension, the plaques were fibrous and spotted with CD68 positive macrophages and CD45RO positive T lymphocytes. There was an inverse topographical relation between the pultaceous cores and angioneogenesis in the patients with chronic thromboembolic pulmonary hypertension.
Histopathological study
The results of the histopathological study are summarised in table 2.
Prevalence of histopathological features found in endoluminal pulmonary thromboendarterectomy material from patients with chronic thromboembolic pulmonary hypertension (n=32), and in the pulmonary arteries of lungs excised at transplantation from patients with thromboembolic (n=7) and plexogenic pulmonary hypertension (n=31)
Plaque composition
Two different types of intimal plaque were found in the patients with chronic thromboembolic pulmonary hypertension: fibrous lesions characterised by large numbers of HHF35 immunoreactive smooth muscle cells and angioneogenesis; and the typical “atherosclerotic” plaques with pultaceous cores and cholesterol clefts (24 cases of chronic thromboembolic pulmonary hypertension, with samples from six excised lungs and 18 pulmonary thromboendoarterectomies) (fig 1). The findings were similar in the three lungs from patients with Eisenmenger syndrome and thromboembolic complications, while the intimal plaques in the large pulmonary arteries from patients with uncomplicated plexogenic pulmonary hypertension consisted of HFF35 positive cell-rich fibrous tissue spotted with inflammatory cells. Two small clusters of cholesterol clefts were found in the lung of one patient with primary pulmonary hypertension and one with Eisenmenger syndrome without any signs of thromboembolic complications. The main difference between the cases with chronic thromboembolic and plexogenic pulmonary hypertension was that only the former had plaques containing abundant pultaceous material.

(A) Recent thrombotic material (red) layered on reabsorbing/organising thrombotic material and fibrous tissue from one patient with transplanted chronic thromboembolic pulmonary hypertension; the arrowheads indicate a deep core, and the large arrow shows ongoing core formation in the thrombotic material. (B) Pulmonary thrombo-endarterectomy sample showing residual fibrin layers in the newly formed fibrous tissue (arrowheads); note the vascular neogenesis typical of thrombus organisation and the absence of a pultaceous core. (C) Deep pultaceous core surrounded by HHF-35 actin positive smooth muscle cells (brown) in a proximal vessel from a lung with chronic thromboembolic pulmonary hypertension excised at transplantation. (D) Typical “atherosclerotic” plaque from a pulmonary thromboendarterectomy sample: note the residual layers of the elastic media of the pulmonary artery (arrowheads). (E) Cluster of foam macrophages with lymphocytes in reabsorbing thrombotic material. (F) Anti-CD45RO immunostaining for T lymphocytes. A, B, D, E: Movat pentachrome stain; C, F: avidin–biotin complex; C: anti-HHF-35; F: anti-CD45RO.
Thrombotic material
Recent thrombotic material was found in 33 of the cases of chronic thromboembolic pulmonary hypertension (six lungs excised at transplantation and 27 pulmonary thromboendarterectomy samples) and the three cases of Eisenmenger syndrome complicated by thromboembolic events (all three lungs excised at transplantation). The thrombi were layered on organising/organised thrombotic material and fibrous tissue (fig 1A). Organised/reabsorbing thrombi were characterised by the presence of residual fibrin layers embedded in the fibrous tissue (fig 1B), which were seen in 34 cases of chronic thromboembolic pulmonary hypertension (27 pulmonary thromboendarterectomies and seven explanted lungs) and in the three cases of Eisenmenger syndrome complicated by thromboembolic events.
Angioneogenesis
Angioneogenesis was observed in 37 of the 39 cases of chronic thromboembolic pulmonary hypertension (all seven lungs excised at transplantation and 30 pulmonary thromboendarterectomy samples) and in two of the three cases of Eisenmenger syndrome with thromboembolic complications (fig 1B). The type of neogenesis varied from capillary (CD 34 positive endothelial cells) to arteriolar-like structures with media-like walls consisting of HHF 35 positive smooth muscle cells lined with CD34 positive endothelial cells (fig 2).
Vascular neogenesis in pulmonary thromboendarterectomy samples. (A) Newly formed vessels lined with CD34 positive endothelial cells. (B) HHF-35 positive smooth muscle cells reproduce “arteriolar” walls surrounding endothelial cells. Avidin–biotin complex: (A) anti-CD34; (B) anti-HHF-35.
Inflammatory cells
Multiple clusters of foam cells were identified in 33 of the cases of chronic thromboembolic pulmonary hypertension (the seven explanted lungs and 26 pulmonary thromboendarterectomy samples). Lymphocytes were associated with the foam cells in 31 cases, and observed alone in a further three cases. Sparse foam cells and lymphocytes were found in all the cases of primary pulmonary hypertension, in 18 cases of Eisenmenger syndrome, and in the three cases of Eisenmenger syndrome complicated by thromboembolic events (fig 1E, F).
Dystrophic calcification
Dystrophic calcifications were found in 18 of the 39 cases of chronic thromboembolic pulmonary hypertension (four lungs and 14 pulmonary thromboendarterectomy samples), and in one of the cases of Eisenmenger syndrome with thromboembolic complications. The calcium deposits were in both the fibrous tissue and the thrombotic material.
Pulmonary artery remodelling
The pulmonary artery wall underlying the intimal plaques showed the typical remodelling of atherosclerotic systemic arteries (fig 1A, D), characterised by expansion of the arterial wall, with loss of integrity and thinning of the tunica media, and parallel plaque extension toward the arterial wall. This finding was independent of the plaque composition.
Immunohistochemistry
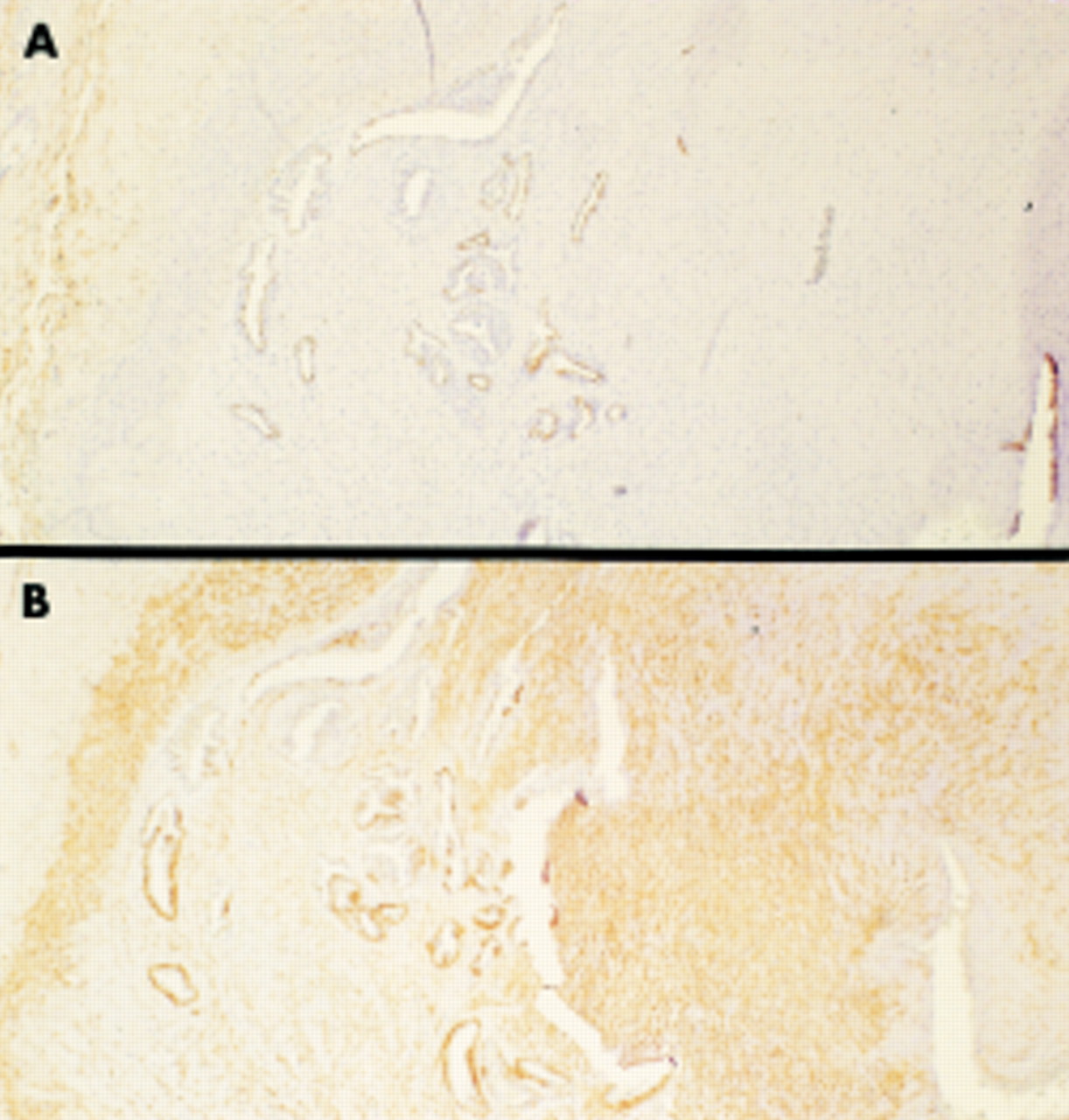
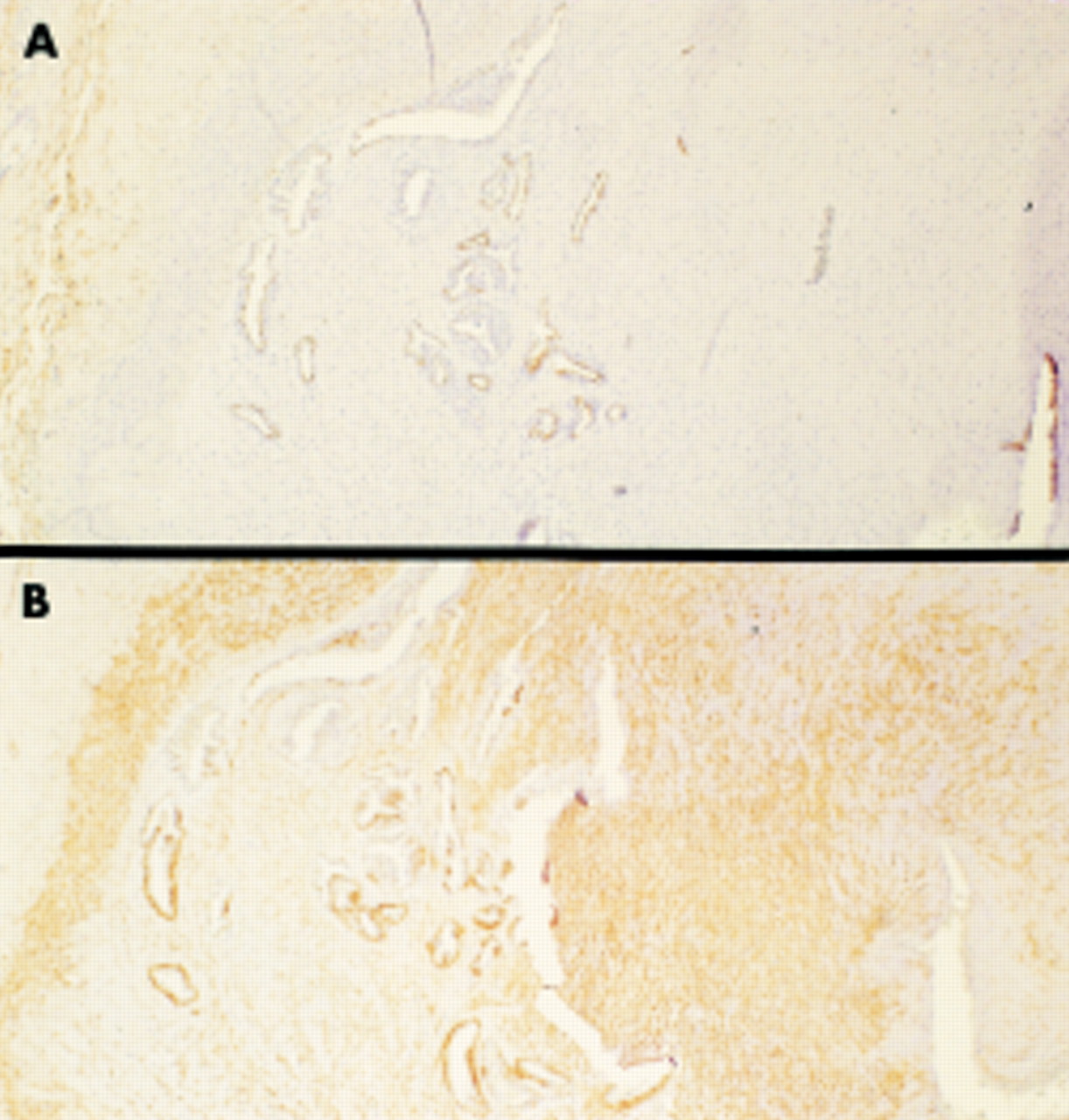
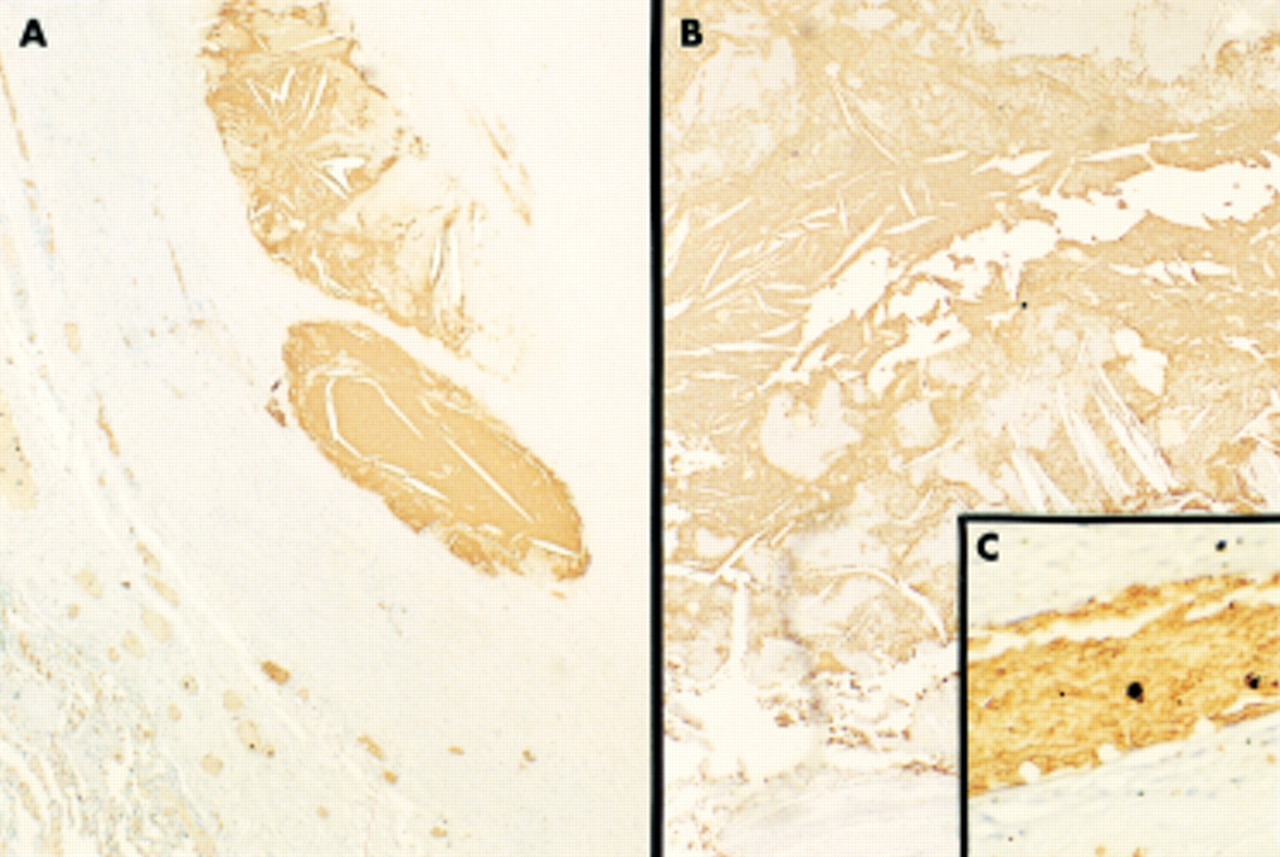
Immunostaining with anti-fibrin, anti-IIb/IIIa, and anti-glycophorin A antibodies confirmed the presence of the thrombus components revealed by the Movat pentachrome stain in the plaques from the patients with chronic thromboembolic pulmonary hypertension. Immunostaining with anti-glycophorin A antibodies clearly showed the prevalence of erythrocyte membrane derived material in the pultaceous cores (fig 3A) and the organising thrombotic material (fig 3B). The intra-sample positive control was provided by red cells (fig 3C).

{kind=link}
{kind=link}
{kind=link}
(A) Pultaceous material with cholesterol clefts; the glycophorin A immunoreactive material of the core is surrounded by a fibrous capsule. (B) Ongoing core formation from thrombotic material. (C) Intra-sample control showing specific immunostaining of red cells for anti-glycophorin A antibodies. All panels: avidin–biotin complex, anti-glycophorin A.
Topographical observations
In the patients with chronic thromboembolic pulmonary hypertension, atheromatous cores (fig 1C, F) were localised deeply inside the lesion and close to the tunica media, or superficially, near to or within the thrombotic material. Angioneogenesis and the pultaceous material had an inverse topographical relation, with the areas rich in new vessels being characteristically free of pultaceous material (fig 1B).
Atherosclerosis risk factors in patients with thromboembolic and plexogenic pulmonary hypertension
The patients with chronic thromboembolic pulmonary hypertension were significantly older (p < 0.05) than those with plexogenic disease, probably because of the earlier development of pulmonary hypertension in primary pulmonary hypertension and Eisenmenger syndrome, and the exclusion of patients older than 65 years from our lung transplantation programme. There were no significant differences in serum cholesterol, triglyceride, and glucose concentrations, or in systolic and diastolic systemic blood pressure, between the thromboembolic and plexogenic groups (table 3), or between the patients with chronic thromboembolic pulmonary hypertension aged more or less than 60 years. However, smoking was significantly less likely in the patients with plexogenic pulmonary hypertension.
Classical risk factors for atherosclerosis in patients with chronic thromboembolic and plexogenic pulmonary hypertension
Predictive value of candidate factors for the histopathological findings
At multivariate analysis, only chronic thromboembolism significantly predicted the presence of pultaceous material in large pulmonary arteries, with the presence of organised and recent thrombi, calcifications, and cholesterol clefts.
DISCUSSION
Our results show that the composition of pulmonary artery plaques in patients with chronic thromboembolic pulmonary hypertension is very different from that in patients with pure plexogenic pulmonary hypertension, the former having large pultaceous cores that are absent in the latter. They also show that erythrocyte membrane derived glycophorin A is a major component of this pultaceous material; glycophorin immunoreacting material was observed in deep cores surrounded by fibrous capsules and separated by thrombotic stratifications, and within the thrombotic material. Thromboembolic material is therefore sufficient on its own to induce plaque formation and influence its composition. The plaques in the patients with plexogenic pulmonary hypertension consist of fibrous tissue without pultaceous cores.
The atherogenic process seems to be independent of metabolic risk factors; blood cholesterol, triglyceride, and glucose concentrations were similar in the patients with plexogenic or chronic thromboembolic hypertension. Only smoking was significantly more frequent in the latter, probably because patients with congenital heart disease or early onset primary pulmonary hypertension are unlikely to smoke. Furthermore, the angiographically documented absence of coronary atherosclerosis and the pathological confirmation of normal coronary arteries in the hearts of the patients with Eisenmenger syndrome indirectly confirm the non-atherogenic habitus of the entire population. The large pulmonary artery pathology in our patients can therefore be attributed entirely to their thromboembolic or plexogenic hypertension.
The likelihood of finding pultaceous cores in patients with plexogenic pulmonary hypertension is extremely low. The pathological changes characterising plexogenic pulmonary hypertension are typically those seen in small arteries and capillary vessels (medial hyperplasia, intimal thickening, and plexiform lesions), whereas large proximal pulmonary arteries usually develop fibrous intimal thickening.1–4,9 Angioneogenesis is characteristically absent except in the presence of a thromboembolic complication. In chronic thromboembolic pulmonary hypertension, the distal vessels are typically spared or show distal embolisation with recent thromboembolic material or a multichannel pattern1; the large pulmonary arteries in our patients showed a combination of recent and organising thromboembolic material, smooth muscle cell-rich fibrous plaques with angioneogenesis, and atherosclerotic plaques with pultaceous material.
Bilayered cell membranes are lipid-rich structures and probably a major source for cholesterol clefts, as indicated by their presence in recently deposited thrombotic material. The lipid content of plasma membranes is very different from that of endoplasmic reticular membranes (highest) or mitochondrial membranes (lowest, and different in the inner and outer membrane).10 All the thrombus cells (white cells, red cells, and platelets) are membrane bound, and platelets and white cells contain other membrane bound structures (granules, lysosomes, reticular structures, mitochondria, and so on). The large number of red cells in thrombi and their abundant glycophorin-A content contribute to the formation of pultaceous material, which was immunostained by specific glycophorin-A antibodies. As glycophorins are exclusively erythrocyte membrane components,11 the presence of glycophorin immunoreactive material in pultaceous cores indicates that at least some of it comes from erythrocyte membranes.
The pultaceous material seems to localise remote from the angioneogenesis that usually occurs during thrombus reabsorption/organisation. Angioneogenesis was typically surrounded by newly deposited fibrous tissue and was never seen in the pultaceous material. These findings suggest an inverse relation between angioneogenesis and the accumulation of pultaceous material, and deserve further investigation of the mechanisms that govern thrombus organisation.
Inflammation and the immunophenotype of inflammatory cells (T lymphocytes and macrophages) were common to plexogenic and thromboembolic pulmonary hypertension; however, inflammatory infiltrates were sparse within the fibrous tissue in the former and often clustered in groups in the latter. This distribution probably reflects the inflammatory trigger: the endothelial insult is caused by high pressure levels in plexogenic pulmonary hypertension but by thrombotic material in chronic thromboembolic pulmonary hypertension. The effects of hypertension in both plexogenic and thromboembolic pulmonary hypertension also reflect on arterial wall remodelling: like systemic arteries affected by atherosclerosis, pulmonary arteries undergo vessel wall remodelling regardless of plaque composition. Inflammation and remodelling are therefore further elements that make the plaques observed in our study similar to those affecting systemic arteries.
The spontaneous human models of chronic thromboembolic and plexogenic pulmonary hypertension suggest that systemic arterial atherosclerotic plaques may be a partial result of thrombotic or haemorrhagic events,12 at least in some patients or in some lesions. The potential origin of plaque cores from thrombotic material may explain why pultaceous core-rich plaques can be found in the systemic arteries of patients without any of the classical risk factors for atherosclerosis. Both thrombosis and haemorrhages imply the presence of blood cells in a given lesion, thus extending the number of episodes that may contribute to core/plaque formation during life. These observation do not undermine the proven role of metabolic and mechanical contributors to the pathogenesis of multifactorial atherosclerosis, but may help to refocus attention on the role of thrombus in atherogenesis.13–17
Conclusions
The human model of thromboembolic pulmonary hypertension shows that thrombotic material can provide the basic elements for the pultaceous material characteristically present in the core of atherosclerotic plaques, whereas hypertensive non-thromboembolic arterial conditions induce fibrous neointimal plaque formation in which foam cells and lymphocytes are common, but the pultaceous-rich cores commonly seen in atherosclerotic plaques are exceptional. Although these data do not undermine our consolidated knowledge of atherosclerotic plaque composition or pathogenetic theories, or exclude other mechanisms underlying the formation of pultaceous material, they may help future studies of the clinical and pathological correlates of systemic atherosclerosis.
Acknowledgments
Study supported by grants: “Ricerche Finalizzate e Correnti” IRCCS Policlinico S Matteo, Pavia, Italy