Article Text

Abstract
Objectives Pulmonary arterial hypertension (PAH) is a devastating disease with limited survival and occurs as a frequent complication in patients with systemic sclerosis (SSc). A definite diagnosis of PAH is obtained by right heart catheterisation (RHC); however, the initial suspicion is raised by non-invasive methods. We assessed the diagnostic accuracy of key parameters derived from cardiopulmonary exercise testing (CPET) for detecting and ruling out SSc-associated PAH.
Methods In a multicentre setting, we prospectively evaluated 173 consecutive patients with SSc without known PAH, but with clinical suspicion of PAH. Each patient underwent CPET and RHC.
Results RHC identified PAH in 48 patients (27.8%), postcapillary pulmonary hypertension (PH) in 10 patients (5.8%) and ruled out PH in 115 patients (66.5%). CPET parameters correlated significantly with pulmonary haemodynamics. PeakVO2 and VE/VCO2 showed highest correlations with pulmonary arterial pressure, transpulmonary pressure gradient and pulmonary vascular resistance. Several parameters showed high sensitivity and specificity for PAH detection by receiver operating characteristic analysis. However, peakVO2 showed highest diagnostic accuracy (sensitivity 87.5%, specificity 74.8% at a threshold level of 13.8 mL/min/kg). A peakVO2 of >18.7 mL/kg/min was reached by 38/173 patients (22%) and excluded PAH in our cohort (negative predictive value 1.0). A nadir VE/VCO2 ratio of >45.5 showed a positive predictive value of 1.0. Diagnostic accuracy was highest in patients with low pulmonary arterial wedge pressure (<12 mm Hg). There were no study-related serious adverse events.
Conclusions CPET is a safe and valuable method in the non-invasive detection of SSc-associated PAH. It may be particularly beneficial for reducing unnecessary RHC procedures.
Statistics from Altmetric.com
Introduction
Pulmonary arterial hypertension (PAH) is a severe chronic disease, harbouring a poor prognosis and frequently resulting in right ventricular failure. Patients with systemic sclerosis (SSc) are at particular risk for developing PAH. The reported prevalence of SSc-associated PAH ranges from 5% to 12%.1–3 Even with all available therapeutic options, a recent meta-analysis revealed a 3-year survival rate of only 52%.4 The course of SSc-associated PAH is progressive, accounting for 30% of deaths among patients with SSc.5 Although early disease detection and therapeutic intervention is crucial,6–8 SSc-associated PAH is rarely diagnosed in WHO functional class I or II.8
The diagnosis of PAH is complicated by the fact that left ventricular (LV) diastolic dysfunction is frequently seen in elderly patients and patients with SSc. Diastolic LV dysfunction may alter pulmonary haemodynamics, leading to postcapillary pulmonary hypertension (PH).9 ,10 The distinction between PAH and postcapillary PH due to diastolic LV dysfunction may be challenging.11
The gold standard for the diagnosis of PAH is right heart catheterisation (RHC).10 ,12 However, non-invasive tools provide surrogates for the presence of pulmonary vascular disease, guiding the decision whether to perform RHC.10–13 While a definite diagnosis of PAH requires RHC, there is an obvious need for feasible non-invasive methods that are able to detect PAH in early stages. In addition, these tools should be able to exclude PAH with a high likelihood to reduce the number of unnecessary RHC procedures.
Echocardiography is recommended as a screening tool for PAH.10 ,12 ,14 However, the largest diagnostic trial on early detection of SSc-associated PAH showed only a moderate sensitivity (71%) and specificity (69%) of echocardiography and clinical symptoms.13 Pathophysiological considerations suggest that the haemodynamic/metabolic impairment in PAH may be observed during exercise before the disease becomes evident at rest.14 ,15 Stress echocardiography is able to detect increases in pulmonary arterial pressure (PAP) during exercise with a high sensitivity.16 However, due to left-sided heart involvement, these changes may be associated with a substantial increase in pulmonary arterial wedge pressure (PAWP) during exercise in the majority of patients with SSc.17
Gas exchange measurements during exercise show characteristic changes in patients with pulmonary vasculopathy and correlate with clinical severity.15 ,18 ,19 However, the diagnostic accuracy of gas exchange parameters for the detection or exclusion of SSc-associated PAH remains uncertain.
In this study, we systematically investigated the correlation of cardiopulmonary exercise testing (CPET) parameters with the diagnosis obtained by pulmonary haemodynamics at rest in a cohort of 173 patients with SSc with potential signs of PAH, thereby determining the diagnostic accuracy of CPET in these patients.
Methods
Study population
We prospectively evaluated 173 consecutive patients from six expert centres with a confirmed diagnosis of SSc. All patients did not have a prior diagnosis of PAH, but presented with potential clinical signs of PAH which were either symptoms or pathological findings obtained by prior non-invasive testing (ie, right heart enlargement or elevated PAP as assessed by echocardiography, reduced diffusing capacity for carbon monoxide (DLCO) as assessed by pulmonary function testing (PFT), elevated NT-proBNP serum levels). All patients underwent CPET and RHC.
Patients who denied or were unable to perform any of the required procedures and those with incomplete data sets or implausible CPET data were excluded (see online supplementary table S1). Patients receiving targeted PAH medication for other indications such as digital ulcerations, patients with known systolic left heart failure (LV ejection fraction <45%), patients on haemodialysis and one patient with severe coronary artery disease were also excluded from the analysis. A flow chart containing the enrolment algorithm and relevant study procedures is shown in figure 1.
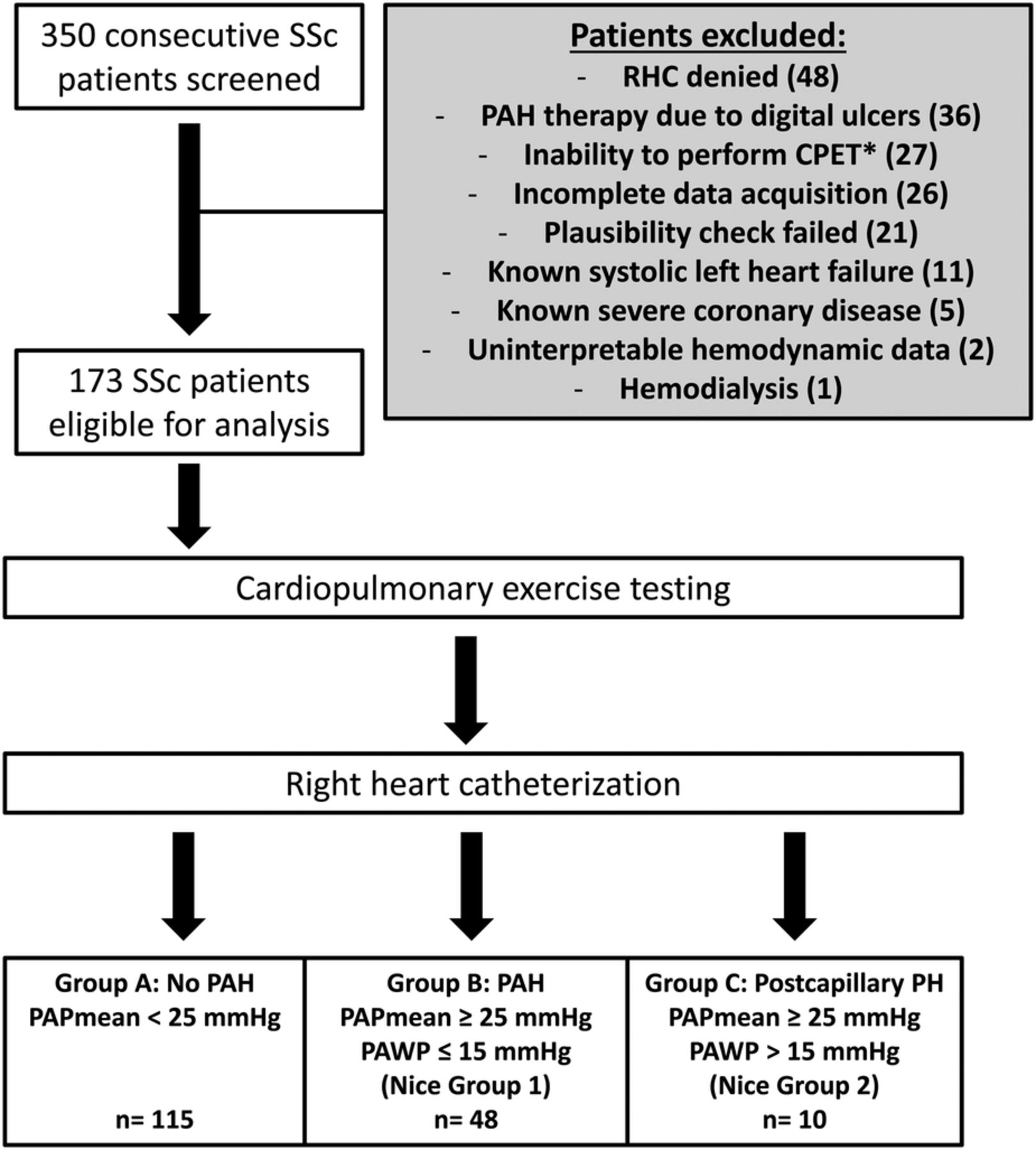
Flow chart of patient inclusion and study procedures in 350 patients with SSc. *Patients denying to perform CPET as well as patients with potential CPET contraindications were summarised in this category. These contraindications included neuromuscular involvement, joint involvement, uncontrolled hypertension, instable arrhythmia and permanent use of supplemental oxygen. CPET, cardiopulmonary exercise testing; PAH, pulmonary arterial hypertension; PAWP, pulmonary arterial wedge pressure; PH, pulmonary hypertension; RHC, right heart catheterization; SSc, systemic sclerosis.
supplementary data
This study was conducted in accordance with Good Clinical Practices and the current version of the revised Declaration of Helsinki. The respective local Research Institutional Review Board approved the analysis.
Diagnostic procedures
Pulmonary function testing
Total lung capacity (TLC), forced vital capacity, forced expired volume in 1 s and DLCO were all measured before CPET by a standardised procedure.20
Cardiopulmonary exercise testing
CPET was performed on a stationary, semirecumbent cycle ergometer. A detailed description of the used methodology can be found in the online supplementary material section. The visual determination of the anaerobic threshold, nadir VE/VCO2 and peak Petco2 is shown in online supplementary figure S1.
Classification of patients
Based on haemodynamic measurements, patients were classified into three groups: group A—patients without PH (mean PAP <25 mm Hg); group B—PAH (Nice group 1) defined by a mean PAP ≥25 mm Hg and a PAWP ≤15 mm Hg;10 ,12 group C—postcapillary PH (Nice group 2) defined by a mean PAP ≥25 mm Hg and a PAWP >15 mm Hg. Group A was further divided into two subgroups to separate patients with normal pulmonary haemodynamics (mean PAP <21 mm Hg) from those with a slightly elevated mean PAP (21–24 mm Hg) not fulfilling the definition of manifest PH (in the case of SSc, termed ‘borderline’ PH).12
To analyse potential differences in diagnostic accuracy depending on disease severity, patients with PAH (group B) were divided into those with moderate mean PAP elevation (B1) and those with severe disease (B2), according to the median value of the mean PAP in the whole PAH cohort (37 mm Hg) (see online supplementary table S2).
Statistical analysis
All calculations were performed with SPSS, V.21 (IBM, Armonk, New York, USA). Contingent on distributional characteristics (ie, normality as assessed by the Shapiro-Wilk test) either parametric (ie, analysis of variance (ANOVA), t-test) or non-parametric (ie, Kruskal-Wallis test, Mann-Whitney U test) methods were used to compare groups. Receiver operating characteristic (ROC) analysis was either performed on all included patients or on all patients except the subgroup with advanced PAH. Diagnostic accuracy of CPET parameters was determined by ROC analysis. To discriminate patients with PAH from those without PAH, ROC analysis compared patients with PAH with those either without PAH (group A) or with postcapillary PH (group C). Linear and reciprocal (y=(b0+(b1/x))) regression models (Spearman's rank correlation) were used for determining correlations between haemodynamics and gas exchange parameters. Continuous data are summarised by mean±SD or SE. To guard against type I error inflation (ie, over 5%), pairwise comparisons were evaluated by Tukey's method (ANOVA) or, otherwise, using the sequentially rejective Bonferroni-Holm procedure.
Results
One hundred and seventy-three patients were included into the final analysis (figure 1). Demographical data, haemodynamic characteristics, pulmonary function and echocardiography of all groups are shown in table 1. Most patients were female (86%), and patients with PAH were older than those without PAH (67±9 vs 55±13 years, p<0.001). Otherwise, no significant differences in demographical data were found between groups. As expected, diffusion capacity was reduced in all groups, with lowest values in patients diagnosed with PAH. However, PFT revealed no signs of significant restrictive lung disease among all groups, as indicated by a normal TLC. Disease duration of SSc tended to be longer in patients with postcapillary PH, but this difference did not reach statistical significance. There were no serious adverse events related to any of the study procedures.
Demographic data and patient characteristics
Haemodynamic characterisation
Based on the haemodynamic classification by RHC, we found 115 patients (66.5%) without PH, 48 patients (27.8%) with PAH and 10 patients (5.8%) with postcapillary PH (table 1). Among the 115 patients without PH, 17 patients showed a slightly elevated mean PAP between 21 and 24 mm Hg with normal PAWP (borderline PH). In the 10 patients with postcapillary PH, the mean PAP was 29±4.1 mm Hg, and none of these patients had an increased transpulmonary pressure gradient (TPG) >12 mm Hg, diastolic pressure gradient >7 mm Hg or pulmonary vascular resistance (PVR) >3 Wood units, indicating isolated postcapillary PH (table 1).
Relationship between haemodynamics and gas exchange
We found significant differences between patients without PAH and those with PAH in most of the analysed gas exchange parameters (table 2). The differences in peakVO2, AT, nadir VE/VCO2 and peak PETCO2 remained significant when comparing patients without PAH and normal mean PAP (group A1) with those with PAH and moderately increased mean PAP (group B1) (figure 2). None of the analysed parameters showed significant differences between group B1 and group C (postcapillary PH). Only peakVO2 and nadir VE/VCO2 showed significant differences between group B and group C, as well as between group A1 and group C (figure 2).
Differences in key gas exchange parameters between patients without PAH (group A), patients with PAH (group B) and patients with postcapillary PAH (group C)

Differences in key gas exchange parameters among the various subgroups of patients with systemic sclerosis. Values are shown as group means±SEM. PETCO2: determination of significant differences by analysis of variance with Tukey's correction. Peak VO2, AT, nadir VE/VCO2: determination of significant differences by Mann-Whitney U tests with Bonferroni-Holm correction. *: p<0.05 vs group A1, †: p<0.05 vs group A2, ‡: p<0.05 vs group B1, §: p<0.05 vs group B2, ||: p<0.05 vs group C. PAH, pulmonary arterial hypertension; PH, pulmonary hypertension.
In patients with borderline PAP elevation (group A2) and patients with PAH (group B), there was a constant decrease in peakVO2, AT and peak PETCO2, as well as a constant increase in VE/VCO2 as the mean PAP increases. Patients with postcapillary PH (group C) also showed a reduction in peakVO2, AT, peak PETCO2 and an elevated nadir VE/VCO2 (figure 2). All analysed parameters were more impaired than group A2 (borderline PH).
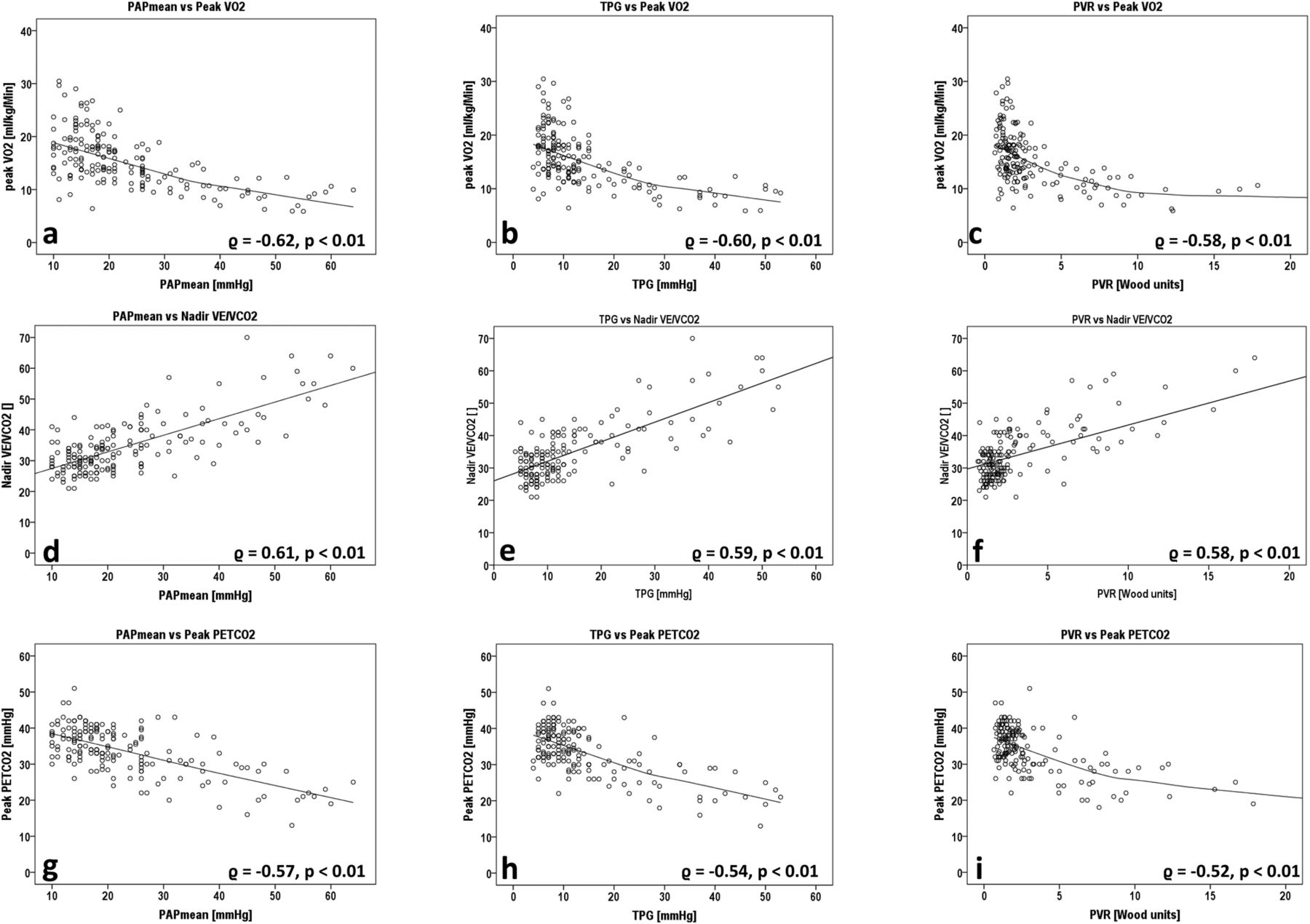
The analysed gas exchange parameters show significant correlations to resting pulmonary haemodynamics. A regression analysis was performed, based on the whole patient cohort (figure 3). Surprisingly, peakVO2 showed a strong reciprocal relationship to mean PAP (r=−0.62, p<0.01), TPG (r=−0.60, p<0.01) and PVR (r=−0.58, p<0.01). Peak PETCO2 also showed a strong reciprocal relationship to mean PAP (r=−0.57, p<0.01) and TPG (r=−0.54, p<0.01); however, the correlation to PVR was weaker (r=−0.52, p<0.01). Nadir VE/VCO2 showed strong linear correlations to mean PAP (r=0.61, p<0.01) and TPG (r=0.59, p<0.01), and a slightly weaker correlation to PVR (r=0.58, p<0.01) (figure 3).
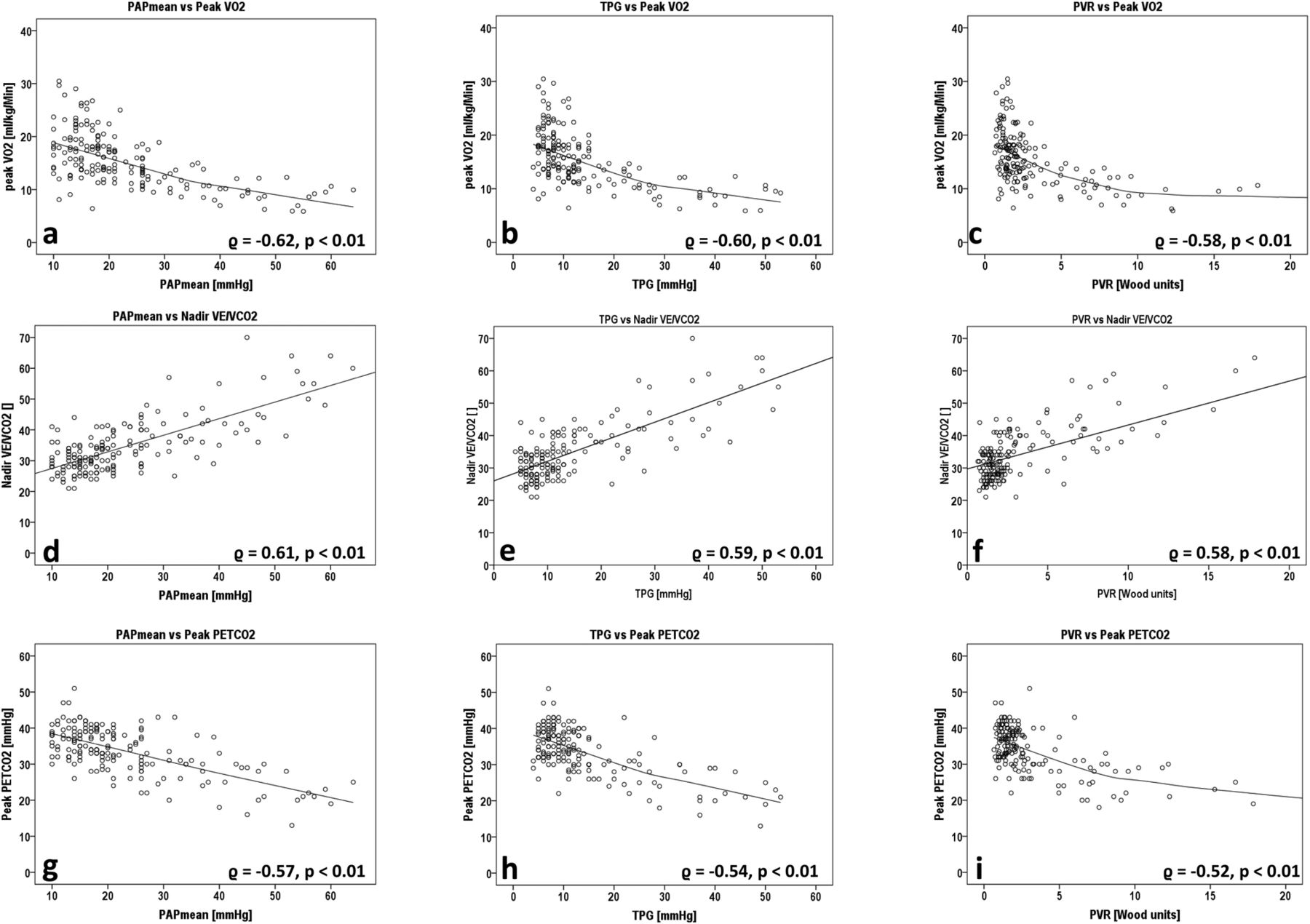
Correlation of gas exchange parameters (peak VO2, nadir VE/VCO2, peak PETCO2) with resting pulmonary haemodynamics (mean PAP, TPG and PVR). Display of the whole patient cohort (n=173). ϱ: Spearman's rank correlation coefficient. Fitting curves were calculated by linear models or by the loess procedure for inverse relationships. PAP, pulmonary arterial pressure; PVR, pulmonary vascular resistance; TPG, transpulmonary pressure gradient.
From all analysed parameters, mean PAP and TPG were almost equally well reflected by peak VO2 (mean PAP: ϱ=−0.62, p<0.01/TPG: ϱ=−0.60, p<0.001) and nadir VE/VCO2, (mean PAP: ϱ=0.61, p<0.01/TPG: ϱ=0.59, p<0.01) followed by PETCO2 (mean PAP: ϱ=−0.57, p<0.01/TPG: ϱ=−0.54, p<0.01). PVR was best reflected by peak VO2 (ϱ=−0.58, p<0.01) and nadir VE/VCO2 (ϱ=0.58, p<0.01). The correlations of cardiac output/cardiac index with gas exchange parameters were considerably lower. This may be explained by the fact that cardiac output was only measured at rest and not during exercise. Cardiac index showed a better correlation with peak VO2 (ϱ=0.35, p<0.01) and nadir VE/VCO2 (ϱ=−0.25, p<0.01) than cardiac output.
Ability to detect early pulmonary vascular disease by exercise gas exchange parameters
We performed ROC analyses to determine the most relevant parameters for detection or exclusion of PAH in our cohort. For ROC analysis, patients with PAH (group B) were compared with all patients without precapillary PH (groups A/C). Among all analysed parameters, peakVO2 expressed in mL/min/kg showed the highest area under the curve (AUC) of 0.891, closely followed by peak PETCO2 (AUC 0.851), nadir VE/VCO2 (AUC 0.850) and the AT expressed in mL Vo2/min/kg (AUC 0.842) (figure 4A).

Receiver operating characteristic analyses of pulmonary arterial hypertension (PAH) detection by exercise gas exchange parameters (peak VO2, peak PETCO2, nadir VE/VCO2, AT). Upper panel (A): analysis of the whole patient cohort—comparison of groups A+C (no PAH) versus group B (PAH). Lower panel (B): comparison of groups A+C (no PAH) versus group B1 (PAH, mean PAP 25–36 mm Hg) only. AUC, area under the curve; PAP, pulmonary arterial pressure.
In a second ROC analysis, all patients without precapillary PH (groups A/C) were compared with the subgroup of patients with PAH and a moderate increase of the mean PAP (group B1). Again, peakVO2 showed the highest AUC value (0.811) followed by nadir VE/VCO2 (AUC 0.756) peak PETCO2 (AUC 0.748) and AT (AUC 0.718) (figure 4B). The difference in PETCO2 between AT and start of exercise and the difference in VE/VCO2 between AT and start of exercise showed lower AUC values.
Highest AUC values were determined when expressing peak VO2 as an absolute value, corrected for body weight. Regarding PETCO2 and VE/VCO2, best correlations with the invasively determined diagnosis of PAH were achieved by selecting the highest PETCO2 value and the lowest VE/VCO2 value during exercise, instead of selecting the AT values. A detailed analysis is shown in the online supplementary figure S2.
The combination of several parameters showed the highest ability of PAH detection for peakVO2 (mL/min/kg) combined with nadir VE/VCO2 and peak PETCO2. A ROC analysis showed an AUC of 0.908 for this combination (not shown). In a multivariable analysis, peakVO2 and nadir VE/VCO2 were the only parameters showing statistical significance.
Diagnostic accuracy and threshold values
Based on the ROC analyses, threshold values for peakVO2, AT, nadir VE/VCO2 and PETCO2 were determined for different conditions:
Maximising cumulative sensitivity and specificity for each parameter, as calculated by the Youden index.
Minimising the number of false negative results for each parameter by looking at sensitivity values >95%.
Verifying the usefulness of threshold values for nadir VE/VCO2 and PETCO2 known from existing literature.23
Regarding optimised cumulative sensitivity/specificity, peakVO2 reached highest values of all analysed gas exchange parameters (sensitivity 87.5%, specificity 74.8% at a threshold of 13.8 mL/min/kg) (table 3). Peak PETCO2 showed a lower sensitivity (81.3%) and a slightly higher specificity (84.6%) at a threshold of 31.3 mm Hg. In a subgroup analysis, only including patients with PAH with a moderate PAP elevation between 25 and 36 mm Hg (group B1), peakVO2 still showed highest sensitivity (73.9%) and peak PETCO2 highest specificity (84.6%) (see online supplementary table S3).
Threshold values for peak VO2, AT, peak PETCO2 and nadir VE/VCO2 in different diagnostic settings
A peakVO2 threshold level of >18.7 mL/min/kg was reached in 38/173 patients (22%) and excluded the presence of PAH in our cohort (sensitivity 100%, specificity 30.9%, negative predictive value 1.0). In addition, the nadir VE/VCO2 was most predictive of PAH, as all patients with a nadir VE/VCO2 >45.5 (n=15/173, 9%) had PAH (positive predictive value 1.0). This parameter had the lowest rate of false positive results compared with all other analysed variables (specificity 31.3%).
Diagnostic accuracy in relation to PAWP
Patients with PAH with a false negative test result showed a significantly higher PAWP than those with PAH with a positive test result. Therefore, a subgroup analysis was performed, dividing the whole cohort into patients with a PAWP <12 mm Hg (n=127) and those with a PAWP ≥12 mm Hg (n=44), independent of PAH status. For each of the two groups, a separate ROC analysis was performed for all relevant gas exchange parameters. The AUC showed higher values in the group with a PAWP <12 mm Hg compared with the group with a PAWP ≥12 mm Hg for peakVO2 (AUC 0.934 vs 0.775), peak PETCO2 (AUC 0.896 vs 0.750), nadir VE/VCO2 (AUC 0.890 vs 0.739) and AT (AUC 0.882 vs 0.769) (see online supplementary figure S3).
Discussion
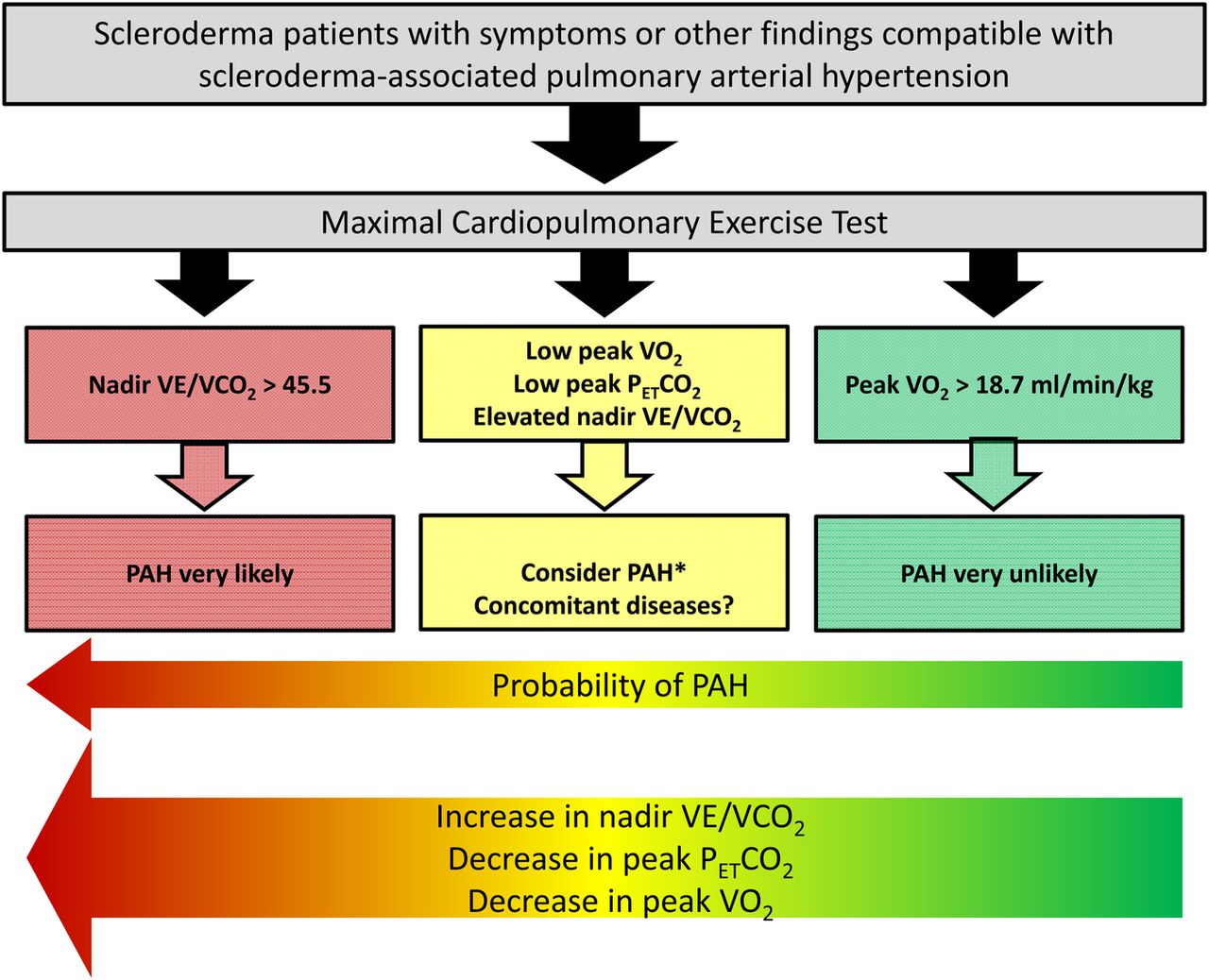
Our data—obtained in a large cohort of patients with SSc with a full haemodynamic profile—demonstrate that several exercise gas exchange parameters show a high diagnostic accuracy in detecting different stages of PAH (figure 5). All parameters correlated well with mean PAP and pressure gradients across the pulmonary circulation. Unexpectedly, among all parameters, peakVO2 was best able to discriminate between patients with and without PAH. A value >18.7 mL/min/kg excluded PAH in all patients. Compared with single parameter analyses, combining multiple gas exchange parameters did not improve the diagnostic yield of CPET in the detection of PAH.

{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
Probability of pulmonary arterial hypertension (PAH) in patients with scleroderma, stratified by cardiopulmonary exercise testing. *Results from other non-invasive diagnostic methods may also be considered for PAH probability assessment.
Since the development of PAH carries a high risk in patients with SSc and is an important predictor of outcome, the timely detection and treatment of this complication is of particular relevance. Echocardiography, which is recommended for screening purposes in SSc, was repeatedly shown to be suboptimal for early detection of PAH in these patients, at least when considered as a single test.13 It is reasonable to assume that pulmonary vascular limitation may be detectable during exercise before it becomes evident at rest. Indeed, we have previously shown that developing pulmonary vasculopathy in SSc may be recognised with non-invasive exercise testing such as CPET.15 However, the ability of CPET to detect such limitations and to specifically attribute them to pulmonary vasculopathy may be potentially biased by several factors.24 Our results may help to specify the role of CPET in describing pathophysiological interactions, and thus help characterising the diagnostic relevance of CPET for PAH detection in two ways:
PeakVO2 is the best discriminator between patients with and without PAH: It may appear surprising that peakVO2, a general marker of maximal exercise capacity, showed highest values of sensitivity and specificity for PAH in the ROC analyses and closely correlated with pulmonary haemodynamics. However, these results are consistent with previous findings from Tolle et al25 and Kovacs et al.26 In both studies, patients with impaired haemodynamics showed a relevant reduction in peakVO2—even in patients without overt resting PAH. This may be explained by the fact that peakVO2 is closely related to cardiac output during exercise, according to the Fick principle. PeakVO2 may be influenced by multiple factors that are not linked to a lack of cardiac or ventilatory reserve, such as pain or joint stiffness. In addition, peakVO2 decreases with age. Therefore, a low peakVO2 cannot be attributed to pulmonary vasculopathy alone. However, a high peakVO2 reflects a good haemodynamic adaptation to exercise and is therefore able to exclude PAH with high accuracy.
Ventilatory efficiency (VE/VCO2, PETCO2) is inferior to peakVO2 in detecting SSc-associated PAH: in our analysis, parameters of ventilatory efficiency showed a high sensitivity and specificity of detecting PAH as calculated by the Youden index. However, levels of PETCO2 and VE/VCO2 during exercise showed a substantial decrease in specificity for sensitivity levels ≥95%. Only a VE/VCO2 ratio >45.5 was able to confirm PAH with high accuracy (positive predictive value 1.0). This may reflect the multifactorial character of SSc, where different mechanisms contribute to cardiac and/or pulmonary involvement, thus affecting the efficiency of CO2 elimination during exercise. An elevation of PAWP seems to be particularly important in this context, as nearly all false negative CPET tests were found in patients with a slight elevation of the mean PAP and a PAWP between 12 and 15 mm Hg. Unfortunately, the uncertainty and the need for a distinct diagnosis of PAH is highest in this group, as pulmonary vascular limitation in these patients is difficult to identify. In particular, PAWP values of ≤15 mm Hg do not rule out left-sided heart involvement.11 Therefore, diagnostic accuracy of CPET was markedly improved when patients with a PAWP of 12–15 mm Hg were excluded (see online supplementary figure S3).
Special attention is required for patients with borderline mean PAP elevation, currently not considered as PAH (21–24 mm Hg), who showed a high number of false positive results which may reflect early pulmonary vasculopathy. However, overlap with postcapillary PH due to left-sided heart involvement cannot be excluded.17 For this group, serial measurements may be able to identify a potential future transition into manifest PAH.
Study limitations
It is important to note that the cohort studied herein was not a screening cohort, as—based on the inclusion and exclusion criteria—we focused on patients who had either dyspnoea or other signs suggestive of PAH, explaining the higher prevalence of PAH in our cohort as compared with epidemiological or screening studies.1–3 ,13 However, this approach enabled us to include a relevant number of patients diagnosed with SSc-associated PAH by RHC. Since a major part of our cohort was symptomatic, our data are not necessarily transferable to asymptomatic patients, and to screening purposes.
A further potential concern may be that we did not consider an impaired lung function as an exclusion criterion. However, the participating expert centres did not include patients with severely compromised cardiopulmonary status and/or being on permanent oxygen supply into this study. This becomes evident, for example, by the mean TLC of 94.5±21.2% of predicted, without significant differences among any subgroups. While all of our patients received lung function testing and CPET, chest CT scans were not part of the study evaluation. We believe that these limitations have no significant impact on the validity of our conclusions.
Conclusions and clinical relevance
In summary, we demonstrate that in patients with SSc, CPET parameters are strongly associated with the presence or absence of PAH as diagnosed by RHC. Thus, CPET is a safe and feasible method in the non-invasive assessment of SSc-associated PAH. While a nadir VE/VCO2 >45.4 is strongly predictive of PAH, a peakVO2 >18.7 mL/min/kg reliably excluded PAH and may thus be helpful for reducing unnecessary RHC procedures. Therefore, CPET appears feasible in symptomatic patients with SSc with a positive screening result. Given the high diagnostic accuracy, the use of CPET—complimentary to other diagnostic tools including echocardiography—may also be feasible for screening approaches. However, this has to be evaluated in future studies.
Key messages
What is already known on this subject?
Patients with scleroderma (SSc) are at high risk of developing pulmonary arterial hypertension (PAH). Cardiopulmonary exercise testing (CPET) shows characteristic gas exchange patterns in patients with PAH. However, the diagnostic accuracy and clinical impact of gas exchange measurements during exercise for the detection or exclusion of PAH in patients with SSc remain uncertain.
What might this study add?
In a large group of patients with SSc and a multicentre approach, we systematically analysed the diagnostic value of key CPET parameters for evaluating SSc-associated PAH, as compared with right heart catheterisation (RHC). We demonstrate that CPET is a reliable tool to detect or rule out PAH and may particularly be able to reduce the number of unnecessary RHC procedures in patients with SSc.
How might this impact on clinical practice?
In patients with SSc who present for evaluation because of clinical signs of PAH, CPET is a non-invasive procedure that is feasible and safe. CPET may be able to exclude PAH with a high probability.
Acknowledgments
The authors thank Linda Nikel and Sibel Gün (Cologne University Hospital) for technical assistance.
References
Footnotes
DD and CN contributed equally to this study.
Contributors All coauthors participated in aspects of the study that qualifies them as authors: DD contributed to the study conception, study design, patient data, analysis/interpretation of the data, statistical analysis and writing the final version of the article. CN contributed to the study conception, study design, patient data, analysis/interpretation of the data, statistical analysis and writing the final version of the article. GK, TB, MH (Dresden), JW, EG and HO contributed to the study conception, patient data, analysis of the data and critical review of article. MH (Cologne) contributed to the study conception, study design, statistical analysis and critical review of the article. RE contributed to the study conception, study design, patient data, analysis/interpretation of the data and critical review of article. SR contributed to the study conception, study design, patient data, analysis/interpretation of the data, statistical analysis and writing the final version of the article. DD and CN (the first two authors) contributed equally to this manuscript, so that a shared first authorship is considered appropriate.
Funding This work was supported in part by a research grant from Actelion Pharmaceuticals (DD, SR).
Competing interests None.
Ethics approval Local institutional review board.
Provenance and peer review Not commissioned; externally peer reviewed.