Article Text

Abstract
Objective Pharmaceutical treatment of latent tuberculosis infection (LTBI) reduces the risk of progression to active tuberculosis (TB); however, poor adherence tempers the protective effect. We aimed to estimate the health burden of non-adherence, the maximum allowable cost of hypothetical new adherence interventions to be cost-effective and the potential value of existing adherence interventions for patients with low-risk LTBI in Canada.
Design A microsimulation model of LTBI progression over 25 years.
Setting General practice in Canada.
Participants Individuals with LTBI who are initiating drug therapy.
Interventions A hypothetical intervention with a range of effectiveness was evaluated. Existing drug adherence interventions including peer support, two-way text messaging support, enhanced adherence counselling and adherence incentives were also evaluated.
Primary and secondary outcome measures Simulation outcomes included healthcare costs, TB incidence, TB deaths and quality-adjusted life years (QALYs). Base case results were interpreted against a willingness-to-pay threshold of $C50 000/QALY.
Results Compared with current adherence levels, full adherence to LTBI drug therapy could reduce new TB cases from 90.3 cases per 100 000 person-years to 35.9 cases per 100 000 person-years and reduce TB-related deaths from 7.9 deaths per 100 000 person-years to 3.1 deaths per 100 000 person-years. An intervention that increases relative adherence by 40% would bring the population near full adherence to drug therapy and could have a maximum allowable annual cost of approximately $C450 per person to be cost-effective. Based on estimates of effect sizes and costs of existing adherence interventions, we found that they yielded between 900 and 2400 additional QALYs per million people, reduced TB deaths by 5%–25% and were likely to be cost-effective over 25 years.
Conclusion Full adherence could reduce the number of future TB cases by nearly 60%, offsetting TB-related costs and health burden. Several existing interventions are could be cost-effective to help achieve this goal.
- burden of disease
- health economics
- tuberculosis
- public health
- cost-effectiveness
- adherence interventions
This is an Open Access article distributed in accordance with the Creative Commons Attribution Non Commercial (CC BY-NC 4.0) license, which permits others to distribute, remix, adapt, build upon this work non-commercially, and license their derivative works on different terms, provided the original work is properly cited and the use is non-commercial. See: http://creativecommons.org/licenses/by-nc/4.0/
Statistics from Altmetric.com
Strengths and limitations of this study
We developed a mathematical model to estimate the burden of non-adherence to latent tuberculosis infection therapy in Canada.
We conducted probabilistic analyses along with microsimulation to consider the parameter uncertainty when estimating individual-level health outcomes.
We suggest a relationship between intervention costs and effects for future adherence interventions that could aid planning of future studies.
There was lack of high-quality direct cost and effectiveness data for current adherence interventions for latent tuberculosis infection therapy; thus, the estimates were extracted from reviews that included other conditions or settings.
Secondary transmission was considered, but dynamic transmission was not included in this analysis.
Introduction
The World Health Organization (WHO) recently published the post-2015 tuberculosis (TB) elimination plan, which aims to reach TB elimination by 2050.1 This strategy demands rapid improvements in TB prevention and treatment outcomes worldwide, in part through optimisation of tools currently in use. Latent TB infection (LTBI) drug treatment has been identified as a priority for TB prevention and elimination in low-incidence regions, but LTBI treatment can only be impactful if high proportions complete an adequate course of drug therapy.2
Unfortunately, adherence is low in most TB programmes with some multicentre studies observing less than 40% completion.3–7 Public health agencies have set higher LTBI treatment completion goals to reach current TB elimination targets, but cost-effective adherence interventions will be required to achieve this goal.8 9 The burden of non-adherence and the potential value of new adherence interventions are not well understood in Canada, a low-TB-incidence region with an approximate annual TB incidence of 5 per 100 000 person-years.10
The health and economic benefits of improved LTBI drug adherence could be high, as improved adherence could have a significant impact on TB epidemiology. Non-adherence leads to a higher lifetime risk of active TB, resulting in higher health system costs and transmissions.11 The long duration and adverse drug reactions related to LTBI therapy are among some of the complex barriers to optimal adherence.12–17
Several interventions have been considered to improve LTBI therapy adherence.18 19 Planning of future trials or implementation strategies can be enhanced with an understanding of their potential cost-effectiveness. Thus, the aims of this study were to estimate the burden of non-adherence and to estimate the maximum allowable cost of hypothetical new interventions to be cost-effective. We also evaluated the health impact and cost sensitivity of four existing adherence interventions, which could potentially improve LTBI drug treatment adherence in Canada.
Methods
Model
An individual-level (microsimulation) model was developed, representing hypothetical individuals with confirmed LTBI who were initiating drug therapy in Canada (figure 1). Ethics approval was not required for this simulation-based study. Individuals entered the simulation in a decision tree that represents the first year of LTBI drug therapy. Based on the individual’s adherence to drug therapy and the drug regimen completed, simulated individuals entered a Markov model with a differential lifetime reactivation risk for TB. TB reactivation could occur any time in an individual lifetime, and individuals were assumed to receive TB drug treatment. On successful completion of active TB therapy, individuals were at heightened risk of TB relapse within the first 2 years but had no risk of active TB after that. The simulation ran over a time horizon of 25 years with annual cycle length. Individuals could enter the absorbing death state at any cycle through natural or TB-related death. The two sources of death were tracked separately so that the impact of adherence on TB-related deaths could be evaluated. The simulation tracked TB-related events (incidence and deaths), healthcare costs and quality-adjusted life years (QALYs). One level of secondary transmission was modelled deterministically by applying the average number of secondary transmissions to each case of active TB, as has been done in previous studies.20 21 The model was developed using TreeAge Pro 2016 software (Williamstown, Massachusetts, USA).

Two-stage latent tuberculosis infection (LTBI) treatment outcome decision analytic model. The decision tree represents LTBI therapy outcomes based on isonicotinylhydrazide (INH) as first choice therapy followed by rifampin in cases of intolerance. The second stage was a Markov model that simulated the remaining time horizon where patients experienced a differential risk of tuberculosis (TB) reactivation based on their adherence to drug therapy.
LTBI drug therapy
In Canada, standard first-line LTBI therapy is 9 months of daily isoniazid (isonicotinylhydrazide (INH)) so it was used as the first treatment regimen in the simulation.10 Individuals were categorised into four groups of adherence to INH: completed ≥80% of doses (fully adherent), completed ≥6 months of therapy but <80% of doses, completed 3–6 months of therapy and completed <3 months of therapy. If an individual was intolerant to INH therapy, they switched to a 4-month regimen of daily rifampin (RIF). Individuals were categorised into ‘completed’ or ‘did not complete therapy’ for RIF, given the lower duration of treatment compared with INH therapy. Irrespective of the regimen used, adherence interventions were simulated to improve the proportion of simulated patients who were fully adherent to their respective drug therapy. Pooled adherence rates from large multicentre studies in low-incidence TB settings characterised the completion rates to INH (61% completion) and RIF (75% completion) therapies (table 1).
LTBI adherence model inputs
Disease inputs
Model parameters and their probability distributions, representing uncertainty about their true values, came from published literature or other secondary sources (table 1). If constructing probability distributions from the available data was not feasible, we specified plausible distributions based on expert opinion. Individual-specific adherence rates were modelled based on published studies and represented the ‘standard care’ scenario.3–5 19 Partial protective effects were given for less than full adherence for INH for 3–6 months or 6–9 months of treatment completion. There is a lack of evidence that partial RIF completion offers a protective effect, so we assumed no partial protective effect for less than full adherence.22 The lifetime risk of TB reactivation and the risk reduction of lifetime TB reactivation with INH therapy was simulated based on observations from the WHO International Union Against Tuberculosis trial.11 Risk reduction of lifetime TB reactivation with RIF was simulated based on best estimates of effectiveness from a previous study.22 We assumed that individual lifetime TB reactivation risk was constant over time.23
Economic inputs
A health system perspective was used to estimate costs. TB diagnosis and care costs were based on a Canadian national report.24 Costs of LTBI drug therapy and monitoring were provided by the British Columbia Centre for Disease Control, a centralised provincial public health agency responsible for the majority of diagnoses and treatments of active and latent TB infections in the province. Costs measured in previous years were adjusted to 2016 Canadian dollars using the Organisation for Economic Co-operation and Development consumer price indices data.25 Health state utility values for TB and LTBI states were obtained from a recent study using the SF-36 survey.26 The costs and QALYs were discounted at a rate of 3%. Willingness-to-pay (WTP) threshold of $C50 000 was used to interpret all results in the base case.27
Analytical approach
In the primary analysis, the health and economic outcomes of a ‘full adherence’ scenario were compared with the ‘current adherence’ scenario to evaluate the impact on TB cases, TB deaths and costs. As the purpose of this approach was to estimate the burden (lost opportunities) attributable to low adherence, no costs were assigned for any adherence-improving intervention. Subsequently, a hypothetical adherence intervention was simulated and compared with the current adherence scenario. In probabilistic analyses, the effectiveness of the hypothetical intervention was varied over the uncertainty distributions reported in previous studies. The relationship between a hypothetical intervention’s efficacy and maximum allowable costs of that intervention was estimated such that it remained cost-effective at the specified WTP threshold.
Evaluation of existing adherence interventions
In a secondary analysis, four existing or emerging adherence interventions identified through literature review were evaluated against standard care. A literature review was conducted to identify potential adherence interventions that could improve LTBI drug therapy adherence. Three systematic reviews summarised randomised controlled trials of medication adherence interventions for TB/LTBI or for other health conditions related or similar to TB (eg, HIV, chronic/semichronic diseases).28–30 The WHO LTBI management guidelines for low-incidence countries also reported potential interventions.31 These reviews summarised evidence largely from randomised controlled trials from multiple settings and were the most relevant sources for intervention effectiveness. Other interventions were considered but excluded because they were significantly more expensive (eg, directly observed therapy).
Four existing adherence intervention types were considered in this evaluation. The first intervention came from a review that summarised evidence of economic incentives to promote adherence to long-course LTBI or TB drug therapy.28 The incentives could include monetary rewards or other types of rewards (eg, food) for adherence. The pooled estimate for adherence incentives compared with standard care was used in the current analysis (RR=1.04, 95% CI 0.97 to 1.13). During the probabilistic simulations, the effectiveness estimates of all interventions were drawn from log-normal distributions matching the pooled point estimates and uncertainty intervals. The next adherence interventions came from a review that summarised evidence for two-way weekly text message (short message service (SMS)) adherence support.30 The SMS intervention evidence came from trials in long-term conditions such as HIV or hypertension and reported outcomes over 1 year. Based on similarities in the length of treatment observation and asymptomatic nature of the conditions in the review, we assumed SMS interventions would have a similar efficacy for the LTBI population. For the purpose of this study, the pooled effect size of two-way SMS interventions was used (RR=1.23, 95% CI 1.13 to 1.35). The third review summarised evidence for a set of adherence interventions and found enhanced adherence counselling to be effective.29 Enhanced adherence counselling involved more intensive patient education, monitoring and counselling related to the importance of drug therapy adherence. Basic adherence counselling is typically provided at prescription pick-up in British Columbia; however, this review summarised evidence of trials studying an enhancement or supplement to standard adherence counselling.29 The specific enhancements varied between the included studies but included up to three additional counselling sessions focused on the importance of adherence.29 Adherence counselling could also be enhanced through regular patient education sessions, monitoring of adherence using diaries and motivational interviewing.32–34 Once again, the pooled effect size was used to specify the input distribution used in the simulation (RR=1.09, 95% CI 1.01 to 1.15).
The WHO guidelines highlighted three studies of peer support interventions.31 In this type of intervention, an individual who has previously completed LTBI treatment would support an individual who is initiating treatment. Peers supporters could also be a friend or family member of the individual initiating drug therapy. In either case, the peer supporter receives some training on how to support the patient and provide ongoing adherence support throughout their drug therapy. The effect sizes reported in these three studies were pooled to derive the effectiveness estimate used in this analysis (RR=1.10, 95% CI 1.00 to 1.29).
Cost data were unavailable for some interventions, so empirical probability distributions could not be specified. An alternative approach was used to estimate the value of these interventions by assigning deterministic costs to each intervention and assessing the cost-effectiveness acceptability at different levels of costs. The results describe the relationship between intervention cost and the likelihood of being cost-effective (the sensitivity of each intervention to cost). The interventions were evaluated individually compared with standard care to estimate the relationship between intervention cost and cost-effectiveness acceptability (ie, probability of being cost-effective over standard care).
Sensitivity analysis
In addition to the probabilistic analysis, key assumptions were varied in the model in a series of deterministic analyses. The time horizon and WTP threshold were varied to examine their impact on the final results. The primary analysis was re-evaluated using 5-year and 10-year horizons. Based on proposed alternative WTP thresholds, the primary and secondary analyses were re-evaluated using $C20 000/QALY and $C100 000/QALY.27
Results
We found that, with current levels of adherence among a Canadian LTBI population initiating drug therapy, TB cases would occur at a rate of 90.3 cases per 100 000 person-years and TB-related deaths would occur at a rate of 7.9 deaths per 100 000 person-years. An intervention that brings the population to perfect adherence would reduce TB cases to 35.9 cases per 100 000 person-years and reduce TB deaths to 3.1 deaths per 100 000 person-years (table 2). This represents a 60% reduction in new TB cases and deaths. When non-adherence was eliminated, QALYs were increased by 12 000 in a simulated population of a million LTBI individuals.
Outcomes associated with current and full adherence scenarios over 25 years
A hypothetical intervention that increased relative adherence by 10% could cost up to $C220 per patient and its incremental cost-effectiveness ratio (ICER) would approach a WTP of $C50 000/QALY. An intervention that increased relative adherence by 40% would nearly bring the population to full adherence and could have a maximum allowable cost of $C450 per patient to remain cost-effective (figure 2). In the Canadian province of British Columbia, 807 individuals initiated LTBI treatment in 2013.35 As an example of health spending impact, an intervention at $C450 would have increased LTBI treatment spending by $C363 150 in this province in that year.

The relationship between an interventions’ effectiveness at improving adherence and maximum allowable cost at a WTP threshold of $C50 000/QALY. Our primary analysis focused on the maximum allowable spending based on the efficacy of an intervention(s) that could improve adherence. QALY, quality-adjusted life year; WTP, willingness to pay.
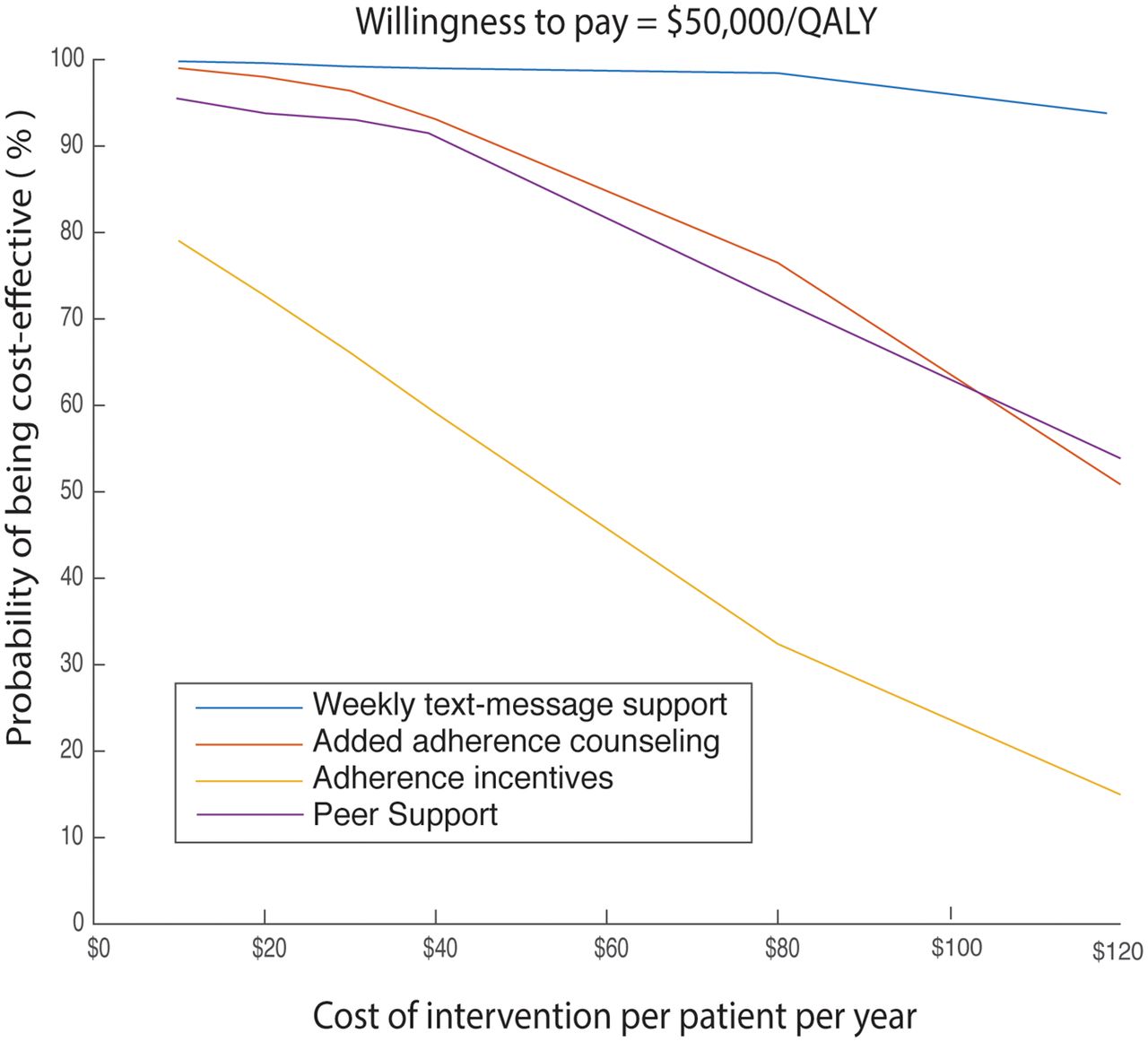
In a simulated population of one million individuals undergoing LTBI therapy, the four adherence interventions added between 900 and 5060 QALYs reduced new TB cases by 9.5%–25% and reduced TB deaths by 5.0%–25% over a 25-year time horizon. Two-way weekly SMS-based adherence interventions appeared to have the greatest health impact and were the least sensitive to cost when compared with standard care (figure 3). Adherence incentives had a steep drop in likelihood of being cost-effective when compared with standard care as their cost increased (figure 3). Online supplementary appendix, tables S1 and S2 report the health impacts for the four existing interventions in the base case evaluation and sensitivity analysis.
Supplementary file 1

{kind=link}
{kind=link}
{kind=link}
The likelihood that each intervention would be cost-effective (when interventions were individually compared with standard care) plotted as a function of intervention cost. Weekly SMS was the least sensitive to cost and would offer the highest probability of being cost-effective at most costs.
In sensitivity analysis, 5-year and 10-year time horizons had little impact on the reduction of TB incidence and deaths (~60%), but the number of TB cases was reduced (online supplementary appendix, table S3). At a 5-year time horizon, full adherence would have an ICER of $C110 066/QALY because of increased drug costs that are not offset by future savings in TB care costs. A hypothetical intervention that brought the population to full adherence could cost between $C150 and $C875 per person depending on the WTP (online supplementary appendix, figure S1). Shorter time horizons reduced the impact of the interventions proportionately. The likelihood of cost-effectiveness of all interventions dropped sharply as cost rose at a WTP threshold of $C20 000 (online supplementary appendix, figure S2). At a WTP threshold of $C100 000, the likelihood of being cost-effective was high for most interventions, except adherence incentives (online supplementary appendix, figure S2).
Discussion
This study is the first to evaluate the burden of non-adherence to LTBI drug therapy in Canada and to estimate the potential value of hypothetical emerging and existing medication adherence interventions. A previous transmission model established that LTBI drug treatment is critical to the global TB elimination strategy but did not explore the impact of adherence interventions in their analysis.36 The financial and health benefits of eliminating non-adherence were apparent in our analysis. We found that, compared with the currently observed level of adherence, full adherence to LTBI therapy could prevent about 60% of future TB cases and deaths among individuals initiating drug treatment for LTBI. This reduction could potentially impact TB incidence at the population level but would require intensive interventions to achieve.
Our findings suggest a maximum allowable cost of $C450 per person treated for an intervention that brings all individuals to full adherence to remain cost-effective. Given the difficulties in achieving large-scale health behaviour change, a more modest relative increase in adherence of 10% was also estimated and would still be cost-effective at a maximal allowable cost of $C220. While the intervention would represent reasonable value for money, the healthcare spending at a population level could be a barrier to implementation in some jurisdictions. Thus, low-cost interventions may be needed to address non-adherence in low-risk populations, reserving high-cost interventions for higher-risk individuals.
Important differences were found among the interventions included in this analysis in the probability of being cost-effective and their sensitivity to intervention costs. The two-way weekly SMS intervention had a high likelihood of being cost-effective relative to standard care and was least sensitive to intervention cost if effective in the same range as demonstrated in previous studies. Peer support and additional adherence counselling sessions were also likely to be cost-effective, but their uncertainty increased as their cost rose. There could be potential for these interventions to be synergistic, but data were unavailable to model that relationship. Adherence incentives were highly sensitive to cost, and the probability of being cost-effective quickly dropped as its cost increases. These findings suggest that some existing approaches could improve the efficiency of LTBI treatment programs, but additional research is needed to confirm their effectiveness in practice.
Previous analyses have assessed the cost-effectiveness of different regimens of LTBI therapy, but none evaluated the value of interventions that directly target drug adherence.14 37–41 Some studies compared the cost-effectiveness of INH to RIF and suggest that shorter-course RIF could be a more efficient first-line therapy. Current evidence on RIF’s non-inferiority to INH is lacking, so it remains second-line therapy in Canada.37 If RIF becomes first-line therapy, or combination INH–rifapentine therapy is approved for use in Canada, the value of these adherence interventions could change and adherence interventions should be re-evaluated under these new guidelines.
This study has several limitations. First, there was lack of high-quality direct effectiveness data for adherence interventions for LTBI therapy; thus, the estimates were therefore extracted from other conditions or settings. However, there is some reason to believe similar effects may occur in LTBI as there is some consistency for certain interventions, such as two-way text messaging, in other infectious and chronic disease conditions.30 As more detailed data are collected through current and future studies, this analysis can be extended to include the observed data.18 Second, there was a lack of reliable cost data for the interventions tested in this analysis. The value of the interventions was presented as a function of their cost to convey their cost-sensitivity. An additional limitation was that dynamic transmission was excluded due to the complexities and assumptions involved in its modelling. We instead applied a simplified assumption on the number of secondary cases due to transmission as has been done in previous studies.20 21 Consideration of higher-order dynamic transmission could increase the benefits of TB cases prevented, so the figures presented here may be underestimated. Finally, we limited our evaluation to a low-risk group of patients with LTBI. Risk factors such as HIV, transplant recipients, dialysis patients and patients on immunosuppressive therapy can increase the risk of TB reactivation and death. Addition of comorbidities could increase the value of eliminating non-adherence, so the results reported may be underestimated.
Further research is needed to understand the synergies between adherence interventions. An adherence intervention could be valuable to implement individually; however, none of the existing interventions is likely to fully address the burden of non-adherence. Also, currently about 50% of patients who would benefit from prophylactic therapy are lost before they initiate drugs.42 Therefore, other strategies such as retaining or increasing the number of patients on therapy would also likely be a valuable. Although important, this analysis investigated closing a single gap in the LTBI care cascade. While adherence improvements could yield a sizeable health benefit, dropouts at each step in the cascade of care mean that less than 50% of individuals testing positive with a LTBI diagnostic test actually would currently benefit from an adherence intervention.7 Likewise, increasing uptake of LTBI therapy would increase the value of improving adherence in larger numbers of patients, having a larger impact on TB control efforts.
This study describes the burden of non-adherence to LTBI drug therapy, the potential value of adherence interventions and suggests their maximum allowable cost to remain cost-effective. Clinicians and researchers of new adherence interventions can use these results to understand the maximum costs for their interventions given the evidence on their effectiveness. Such insight can be used to understand if the intervention is feasible based on the efficacy needed to support intervention costs. Based on the interventions we evaluated, the two-way weekly SMS intervention had the highest likelihood of being cost-effective, followed by peer support and then enhanced adherence counselling. The major costs would be staff training, labour/peer time, overhead and, in some cases, technology development costs. Adherence incentives appear to be the most uncertain strategy and should be kept as a last choice given the availability of more efficient alternatives. However, high-quality studies will be need to confirm effectiveness in practice prior to wide-scale use of these interventions.
References
Footnotes
Contributors AP conceived the study, participated in design of the study, conducted data analysis and drafted the final manuscript. JRC participated in design of the study, conducted data analysis and helped draft the final manuscript. MS participated in design of the study and helped to draft the final manuscript. FM participated in design of the study and helped to draft the final manuscript. JJ participated in design of the study and helped to draft the final manuscript. KS participated in data analysis and helped to draft the final manuscript. RTL conceived the study, secured funding for the study, participated in design of the study and helped to draft the final manuscript. All authors have read and approved the final manuscript.
Funding This study was supported by the British Columbia Lung Association (reference no F10906110) and the Canadian Institutes of Health Research Partnerships for Health System Improvement (reference no 267385). AP was supported in part by the National Institute of Mental Health of the National Institutes of Health under grant no R01MH097558901 and by the Canadian HIV Trials Network. JJ and RTL were supported in part by a Michael Smith Foundation award for Health Research Scholars.
Competing interests RTL is executive and scientific director of the WelTel International Health Society and WelTel, which develop and implement mobile health solutions. The remaining authors declare that they have no competing interests.
Provenance and peer review Not commissioned; externally peer reviewed.
Data sharing statement No additional data are available.