Article Text

Abstract
Objective A multicentre cohort follow-up study of a large number of patients with gastric mucosa-associated lymphoid tissue (MALT) lymphoma was conducted to elucidate the long-term outcome of the disease after Helicobacter pylori eradication.
Methods 420 patients with gastric low-grade MALT lymphoma who had undergone successful H pylori eradication and been followed up for at least 3 years were registered from 21 participating institutes. Responders to treatment were defined as patients whose post-treatment biopsies showed complete histological response (ChR) or probable minimal residual disease (pMRD). Treatment failure was defined as the status of progressive disease or lymphoma relapse after ChR/pMRD.
Results 323 patients (77%) responded to H pylori eradication. A logistic regression analysis showed that absence of H pylori, submucosal invasion determined by endoscopic ultrasonography and t(11;18)/API2-MALT1 were independent predictors of resistance to H pylori eradication. During the follow-up periods ranging from 3.0 to 14.6 years (mean 6.5 years, median 6.04 years), the disease relapsed in 10 of 323 responders (3.1%) while progressive disease was found in 27 of 97 non-responders (27%). Thus, 37 of 420 patients (8.8%) were regarded as treatment failures. Of these 37 patients, transformation into diffuse large B cell lymphoma occurred in nine patients. Among the non-responders and relapsed patients, 17 patients were subjected to a ‘watch and wait’ strategy while 90 patients underwent second-line treatments including radiotherapy (n=49), chemotherapy (n=26), surgical resection (n=6), chemoradiotherapy (n=5), antibiotic treatment (n=2), rituximab monotherapy (n=1) or endoscopic resection (n=1). Probabilities of freedom from treatment failure, overall survival and event-free survival after 10 years were 90%, 95% and 86%, respectively. Cox multivariate analysis revealed endoscopic non-superficial type to be an independent prognostic factor for adverse freedom from treatment failure, overall survival and event-free survival.
Conclusions The excellent long-term outcome of gastric MALT lymphoma after H pylori eradication was confirmed by this large-scale follow-up study.
- Gastric lymphoma
- MALT
- Helicobacter pylori
- endoscopic ultrasonography
- gastric cancer
- IBD
- gastric and duodenal ulcers
- Helicobacter pylori - treatment
- lymphoma
- liver
- Helicobacter pylori - pathogenesis
- colorectal neoplasm
- colonic polyps
- colonoscopy
- colorectal carcinoma
- endoscopic polypectomy
- autoimmune hepatitis
- autoimmunity
- liver immunology
- gastrointestinal immune response
- immunology in hepatology
Statistics from Altmetric.com
- Gastric lymphoma
- MALT
- Helicobacter pylori
- endoscopic ultrasonography
- gastric cancer
- IBD
- gastric and duodenal ulcers
- Helicobacter pylori - treatment
- lymphoma
- liver
- Helicobacter pylori - pathogenesis
- colorectal neoplasm
- colonic polyps
- colonoscopy
- colorectal carcinoma
- endoscopic polypectomy
- autoimmune hepatitis
- autoimmunity
- liver immunology
- gastrointestinal immune response
- immunology in hepatology
Significance of this study
What is already known about this subject?
Helicobacter pylori plays a causative role in the development of gastric mucosa-associated lymphoid tissue (MALT) lymphoma.
The eradication of H pylori leads to a complete remission (CR) of the disease in 50–90% of cases of gastric MALT lymphoma.
What are the new findings?
The excellent long-term clinical outcome of gastric MALT lymphoma after H pylori eradication was confirmed by the follow-up study ranging from 3.0 to 14.6 years (mean 6.5 years, median 6.04 years); the probabilities of freedom from treatment failure, overall survival and event-free survival after 10 years were 90%, 95% and 86%, respectively.
How might it impact on clinical practice in the foreseeable future?
Patients with localised gastric MALT lymphoma who achieved CR after H pylori eradication can be managed only by follow-up endoscopy with multiple biopsies every 1 or 2 years.
Even in non-responders to H pylori eradication, a ‘watch and wait’ strategy may be recommended for more than 2 years unless progression or relapse of lymphoma can be demonstrated in patients with localised gastric MALT lymphoma.
Introduction
Extranodal marginal zone lymphoma of mucosa-associated lymphoid tissue (MALT lymphoma) is a distinct clinicopathological entity in the recent classification of malignant lymphomas.1 2 Gastric MALT lymphoma accounts for 40–50% of primary gastric lymphomas, 20–40% of extranodal lymphomas, 4–9% of all malignant lymphomas and 1–6% of all gastric malignancies.1–3 H pylori plays a causative role in the development of gastric MALT lymphoma, and the eradication of H pylori leads to a complete remission (CR) of lymphoma in 50–90% of cases.4–32 A systematic review of the data from 32 publications revealed that CR was achieved in 78% of 1408 patients with low-grade gastric MALT lymphoma in stage I/II1 treated by H pylori eradication.33 Thus, H pylori eradication is now regarded as the first-line treatment for gastric MALT lymphoma.33 34 However, large-scale long-term follow-up outcome after the eradication therapy is still limited, particularly with regard to relapse or progression and survival.
We therefore conducted a multicentre cohort follow-up study of a larger number of patients with gastric MALT lymphoma in order to elucidate the long-term clinical outcome of H pylori eradication therapy including predictive factors for resistance to the therapy, probabilities of freedom from treatment failure (FFTF) and survival, as well as the prognostic factors for the disease.
Methods
Study design
This was a Japanese multicentre cohort follow-up study. Invitations to join the study were sent to all members of the JAPAN GAST Study Group (JGSG) and 21 institutes across Japan participated. The method used was a questionnaire-based inquiry on clinical and pathological data in each institute. Data for all consecutive patients with primary gastric MALT lymphoma diagnosed and treated by H pylori eradication between March 1994 and March 2007 were collected. The inclusion criteria were: (1) presence of gastric extranodal marginal zone lymphoma of MALT (MALT lymphoma) according to the WHO classification2 and compatible with Wotherspoon's histological score of 4 or 5 in the pretreatment gastric biopsy specimens4; (2) having undergone H pylori eradication therapy using a proton pump inhibitor (omeprazole, lansoprazole or rabeprazole) plus a combination of two antibiotics (amoxicillin, clarithromycin or metronidazole) as the first-line treatment for MALT lymphoma; and (3) follow-up period of at least 3 years after successful eradication therapy. Exclusion criteria were: (1) primary MALT lymphoma arising in the extragastric organs; (2) presence of diffuse large B cell lymphoma (DLBCL) prior to the H pylori eradication; and (3) positive H pylori infection after the final eradication therapy. Study protocols were approved by the institutional review board at each institute and complied with provisions of the Declaration of Helsinki.
Subjects
A total of 420 patients with gastric MALT lymphoma were registered from the following 21 institutes: Kyushu University (n=87), Tohoku University (n=71), Hokkaido University (n=41), Aichi Cancer Center Hospital (n=39), Hiroshima Red Cross Hospital and Atomic-Bomb Survivors Hospital (n=33), Hiroshima University (n=30), Kawasaki Medical School (n=26), Shinshu University (n=25), Hitachi General Hospital (n=12), Kyoto University (n=10), Iwate Medical School (n=9), Nihon University (n=7), Fukuoka University (n=5), Hyogo College of Medicine (n=5), Social Insurance Shiga Hospital (n=4), Hamamatsu University (n=4), Oita University (n=4), Toyama University (n=3), National Hospital Organisation Kyoto Medical Center (n=3), Tsukuba Memorial Hospital (n=1), and Hirosaki University (n=1). A certain proportion of the study population had been included in previous studies.18 23 25 27 31 32
The H pylori status was determined by histology, culture, rapid urease test, 13C urea breath test and/or serology. H pylori infection was judged to be positive if one or more of the tests showed a positive result and to be negative when all tests were negative. The endoscopic type of lymphoma was classified as either superficial, ulcerative, polypoid or others, based on the classification reported previously.3 The clinical stage was determined on the basis of the Lugano staging system, a modification of the Ann-Arbor classification.35 Endoscopic ultrasonography (EUS) was also performed to evaluate the depth of tumour invasion and the degree of perigastric lymphadenopathy.36 37 t(11;18)(q21;q21)/API2-MALT1 was investigated by reverse-transcription PCR38 and/or interphase fluorescence in situ hybridisation.39
Assessment after H pylori eradication therapy
The biopsy specimens after H pylori eradication and other non-surgical treatments was assessed according to the Groupe d'Etude des Lymphomes de l'Adulte (GELA) histological grading system, being classified as either complete histological response (ChR), probable minimal residual disease (pMRD), responding residual disease (rRD) or no change (NC).34 40 Responders were defined as patients whose post-treatment biopsies showed ChR or pMRD. Those patients were regarded as showing clinical CR.34 The remaining patients (rRD or NC) were considered as non-responders. rRD was regarded as clinical partial remission (PR).34 Follow-up endoscopic examinations with biopsies were performed every 3–6 months until confirmation of ChR or pMRD, and repeated every 6–12 months after ChR/pMRD. Treatment failure was defined as the relapse after ChR/pMRD or progressive disease (PD), including transformation into DLBCL. All the biopsy specimens were reviewed by the senior pathologist in each institute.
Second-line treatments for non-responders
Patients with treatment failure or persistence of lymphoma following H pylori eradication were subjected to either a ‘watch and wait’ strategy (no treatment) or various antineoplastic treatments including radiotherapy, chemotherapy with or without rituximab, chemoradiotherapy, rituximab alone, surgical resection or others.
Prognostic factors and statistical analysis
A logistic regression analysis was performed to identify the predictive factors for response to H pylori eradication. FFTF was measured from the date of start of the final H pylori eradication to the treatment failure, which was censored at the date when patients underwent additional therapy without PD or when patients died of causes unrelated to lymphoma. Overall survival (OS) was measured from the date of the eradication to death from any cause, and event-free survival (EFS) was measured from the date of the eradication to treatment failure or death from any cause. Probabilities of FFTF, OS and EFS were calculated by the Kaplan–Meier method and the values were compared using the log-rank test and generalised Wilcoxon test. All variables with p<0.1 by either of the tests were included in multivariate analyses using the Cox proportional hazards model. Other statistical differences were evaluated by the Fisher exact probability test, the χ2 test or the Mann–Whitney U test. p Values <0.05 were regarded as statistically significant. For multiple comparisons, however, p values were interpreted after the Bonferroni correction.
Results
Patient characteristics at baseline
The baseline characteristics of 420 patients are summarised in table A in the online supplement. The median age was 61 years (range 16–87) and 56% of the patients were women. H pylori infection was negative in 10%. The most frequently involved site was the middle third of the stomach (45%), followed by the proximal third (22%). Endoscopically, 67% of tumours were classified as superficial type, 16% as ulcerative type, 12% as polypoid type and 4% as others; 90% of patients had clinical stage I disease. Among 341 patients who underwent EUS, the depth of lymphoma infiltration in the gastric wall was: mucosa in 52%, submucosa in 38% and muscularis propria or beyond in 10% of cases. t(11;18)/API2-MALT1 was positive in 30 of 206 patients (15%) examined.
Response to H pylori eradication
The clinical course after the successful eradication of H pylori is summarised in figure 1. After H pylori eradication, ChR was achieved in 284 patients (68%) and pMRD in 39 (9%). Thus, 323 patients (77%) were responders. There were 97 non-responders (23%), including rRD in 13 (3%) and NC in 84 (20%). The median time from H pylori eradication to ChR or pMRD was 4 months (range 1–94). As shown in table 1, non-responders were significantly associated with male sex, absence of H pylori, proximal or multiple locations, endoscopically non-superficial type, advanced stage (≥II1), deep submucosal invasion and t(11;18)/API2-MALT1. Multivariate logistic regression analysis indicated that male sex, absence of H pylori, the location in the proximal or multiple areas, non-superficial type and advanced stage were independent predictors of resistance to H pylori eradication therapy (table 2). In 175 patients who underwent both EUS and investigation for t(11;18), absence of H pylori, submucosal invasion under EUS and t(11;18)/API2-MALT1 were independent predictors of resistance to H pylori eradication.
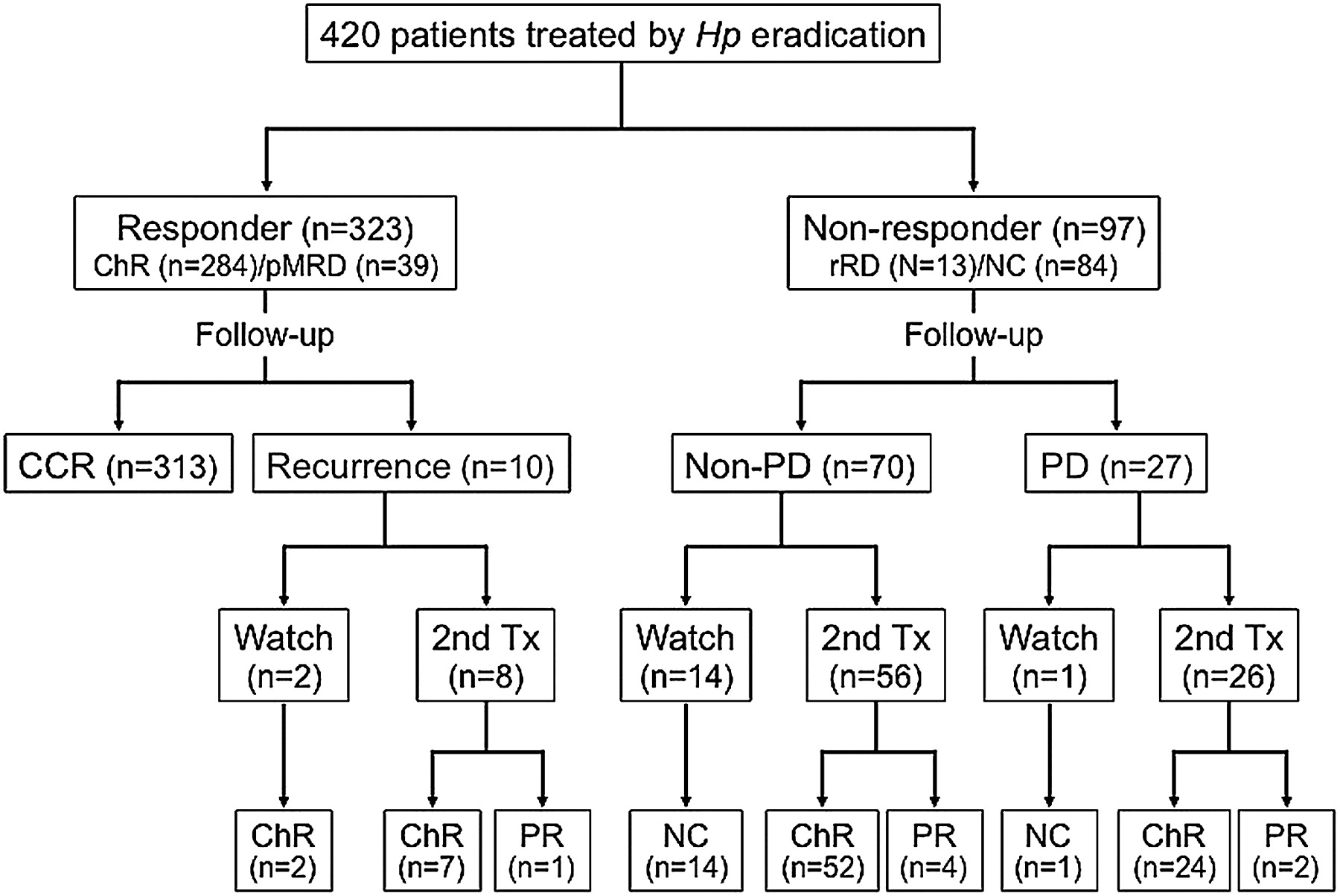
Clinical course of the 420 study patients. Hp, Helicobacter pylori; ChR, complete histological response; pMRD, probable minimal residual disease; rRD, responding residual disease; NC, no change; CCR, continuous complete remission; PD, progressive disease; Tx, treatment; PR, partial remission.
Association between clinicopathological factors and response to the Helicobacter pylori eradication
Predictive factors for resistance to Helicobacter pylori eradication therapy as determined by logistic regression analysis
Relapse in responders
The median follow-up period of 323 responders after ChR/pMRD was 5.48 years (range 1.0–14.3). During the period, lymphoma relapse was observed in 10 patients (3.1%). The time duration from ChR/pMRD was 1–131 months (median 21.5). Only one patient showed transformation into DLBCL, which was treated by surgical resection. Six patients were treated by either chemotherapy (n=4) or radiotherapy (n=2). CR was achieved in those seven patients. Other one patient developed macroscopic local relapse of MALT lymphoma 10.9 years after ChR which was associated with reinfection of H pylori. Re-eradication of H pylori resulted in rRD (PR) in this case. The remaining two patients who showed histological relapse 12 and 13 months after the initial response spontaneously achieved ChR again without any additional treatment.
Treatments for non-responders
As shown in figure 1, PD was observed in 27 of 97 non-responders. Eight patients showed transformation into DLBCL. One PD patient, who was positive for t(11;18) and had been subjected to a ‘watch and wait’ strategy, developed lung metastasis of MALT lymphoma 12 years later.25 The other 26 patients were treated by radiotherapy (n=11), chemotherapy (n=10), chemoradiotherapy (n=3) or surgical resection (n=2). Twenty-four patients achieved CR and two patients treated with radiotherapy or chemotherapy showed PR.
Fourteen of 70 non-responders without PD were subjected to a ‘watch and wait’ strategy while 56 patients underwent second-line treatments. One patient showing rRD (clinically PR) at 20 months was treated with ‘third-line’ antibiotic therapy with gatifloxacin, amoxicillin and rabeprazole which resulted in ChR 15 months later. The remaining 55 patients underwent radiotherapy (n=36), chemotherapy (n=12), surgery (n=3), chemoradiotherapy (n=2), rituximab monotherapy (n=1) or endoscopic resection (n=1). Fifty-two of these 55 patients achieved CR while three patients treated with radiotherapy, chemotherapy or endoscopic resection showed PR.
Figure 1 summarises the clinical course after second-line treatments applied to 97 non-responders and 10 responders with relapse. The second-line treatments resulted in CR in 85 patients, PR in seven patients and NC in 15 patients. The rate of the CR induction by each treatment was 94% by radiotherapy, 88% by chemotherapy, 100% by surgical resection, 100% by chemoradiotherapy, 50% by antibiotics, 100% by rituximab monotherapy and 0% by endoscopic resection.
Treatment failure, long-term outcome and prognostic factors
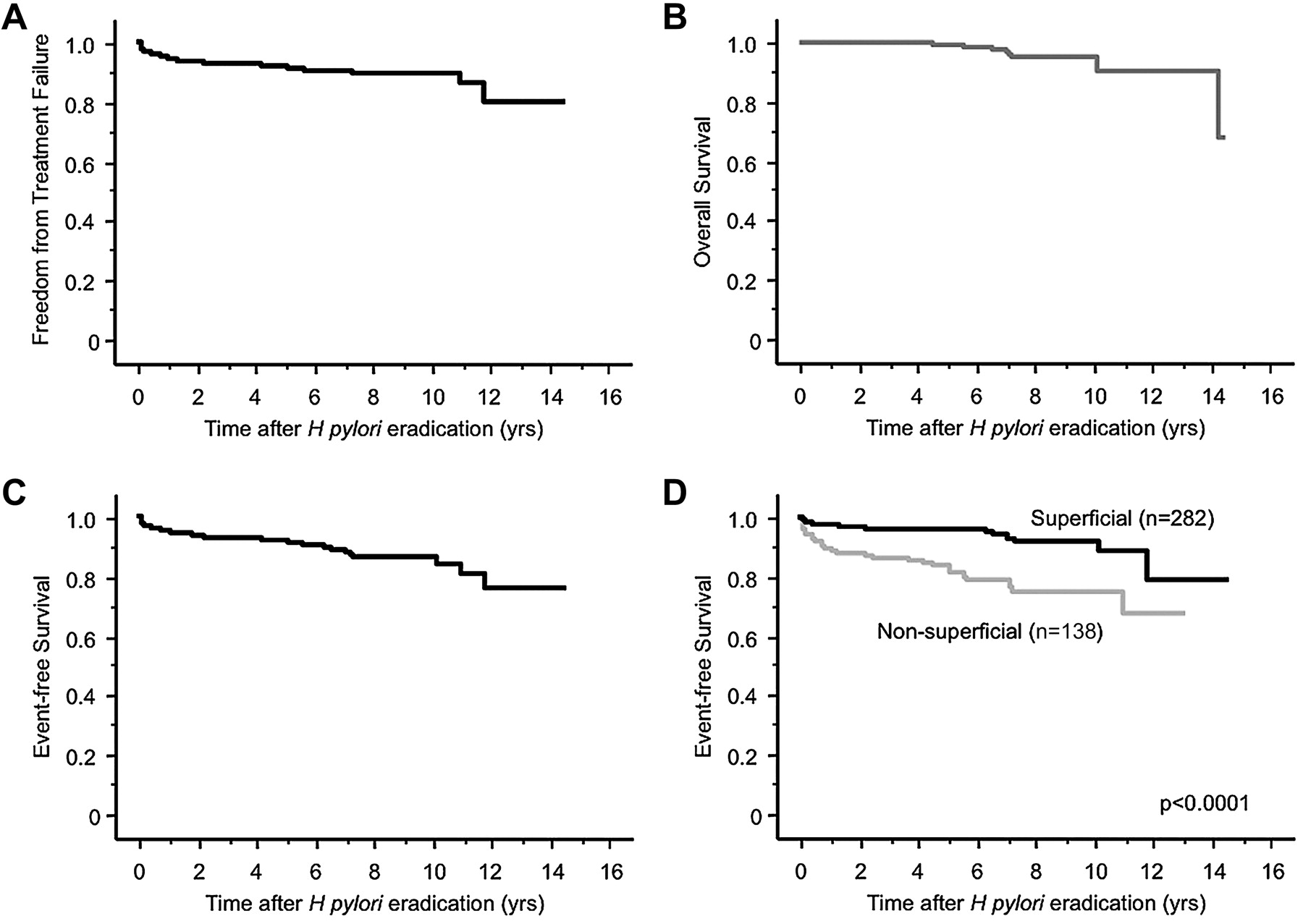
Overall follow-up periods of 420 patients after H pylori eradication ranged from 3.0 to 14.6 years (mean 6.5, median 6.04). PD and disease relapse occurred in 27 patients and 10 patients, respectively. Thus, 37 of 420 patients (8.8%) showed treatment failure. Probabilities of FFTF after 5, 10 and 12 years were 92%, 90% and 80%, respectively (figure 2A). Univariate and multivariate analyses for FFTF are summarised in table B in the online supplement. Univariate analysis showed absence of H pylori, non-superficial type, advanced stage and submucosal invasion under EUS to be significantly associated with an adverse prognosis. Cox multivariate analysis excluding EUS assessment showed non-superficial type to be the single independent predictor for adverse FFTF.
{kind=link}
{kind=link}
Kaplan–Meier curves of 420 patients with gastric MALT lymphoma after Helicobacter pylori eradication. (A) Freedom from treatment failure. (B) Overall survival. (C) Event-free survival. (D) Event-free survival as stratified by endoscopic types (p<0.0001).
During the follow-up period two patients died from transformed DLBCL and 11 from causes unrelated to lymphoma. Probabilities of OS after 5, 10 and 12 years were 99%, 95% and 91%, respectively (figure 2B). Univariate analysis for OS showed that older age, endoscopic non-superficial type, advanced stage and submucosal invasion determined by EUS were significant factors (see table C in online supplement). Cox multivariate analysis showed that older age and non-superficial type were independent predictors for poor OS.
Probabilities of EFS after 5, 10 and 12 years were 92%, 86% and 76%, respectively (figure 2C). As shown in table D in the online supplement, univariate analysis for EFS revealed location in the proximal/multiple areas, non-superficial type, advanced stage and submucosal invasion under EUS to be significantly associated with poor EFS. Cox multivariate analyses excluding or including EUS assessment showed that either non-superficial type or submucosal invasion was the single independent predictor for worse EFS (figure 2D).
Other malignant neoplasms
Other malignancies were found in 35 patients (8.3%), 17 of whom (4.0%) had metachronous gastric cancer. Among these 17 patients, five (29%) had undergone either radiotherapy (n=3) or chemotherapy (n=2). The other malignancies included colorectal cancer (n=3), hepatocellular carcinoma, head and neck cancer, prostatic cancer, uterine cancer (n=2 in each), NK/T cell lymphoma of nasal type, chronic myelomonocytic leukaemia, oesophageal cancer, lung cancer, breast cancer, pancreatic cancer, cholangiocarcinoma, renal cell carcinoma and metastatic bone marrow carcinoma of unknown primary site (each in one patient). Two patients with metachronous gastric cancer also had oesophageal cancer or hepatocellular carcinoma.
Discussion
While many publications have evaluated the efficacy of H pylori eradication for gastric MALT lymphoma, the number of patients in each study is small and the follow-up periods are relatively short. Table E in the online supplement summarises 28 studies that included more than 20 patients treated by successful H pylori eradication.5–32 The number of patients ranged from 21 to 199 and CR was achieved in 1361 of 1877 patients (73%). During the follow-up period (median 0.8–6.3 years), PD was observed in 17 of 1576 patients (1.1%), relapse was recorded in 60 of 1203 patients (4.9%) with CR and treatment failure (PD or relapse) was observed in 118 of all 1877 patients (6.3%). Only five studies had a median follow-up period exceeding 5 years.19 20 29 30 32 Compared with these studies, our investigation is large and the median follow-up period of 6.04 years is the third longest. Based on the cancer incidence data reported from the National Cancer Center, Japan (http://ganjoho.jp/professional/statistics/statistics.html), our study population is presumed to comprise approximately 7% of all patients with gastric MALT lymphoma diagnosed during the period 1994–2006 in Japan. As a result, the rates of ChR/pMRD (77%), relapse (3.1%) and treatment failure (8.8%) in our study were similar to those in the previous studies. However, our PD rate (27 of 420 patients, 6.4%) was higher than previous data (1.1%, table E in online supplement).
Various predictive factors for resistance to H pylori eradiation in gastric MALT lymphoma have been reported, such as absence of H pylori infection,7 13 16 23 31 advanced stage,13 31 DLBCL component,18 19 25 37 proximal location,7 18 24 33 endoscopic non-superficial type,16 18 deep invasion of lymphoma in the gastric wall13 18 19 31 36 37 and t(11;18)/API2-MALT1 translocation.15 31 33 38 39 In our subjects, absence of H pylori was an independent predictor both in a whole analysis (n=420) and in a stratified analysis of 175 patients who underwent EUS and t(11;18) investigation (table 2). In the latter analysis, deep submucosal invasion by EUS and t(11;18) were also determined to be independent predictors. We therefore consider that, in addition to evaluation for H pylori status, the depth of tumour invasion and t(11;18) should also be considered prior to the eradication therapy.34 37It has also become clear in this investigation that non-antral (middle and proximal thirds) involvement of MALT lymphoma in Japanese subjects, which is presumably associated with the high prevalence of pangastritis in the population, should be taken into consideration before eradication therapy.
To date, prognostic factors for FFTF have not been reported in gastric MALT lymphoma. We found that non-superficial type was the most significant factor for adverse FFTF (see table B in online supplement). Among patients with treatment failure, the number of PD (n=27) was greater than that of relapse (n=10). It has been reported that relapse of MALT lymphoma is occasionally associated with reinfection with H pylori.15 19 21 22 29 In our study, however, only one of 10 patients with relapse had reinfection. Interestingly, the patient developed macroscopic local relapse 10.9 years after the initial ChR. These observations suggest that the clonal memory B cells may exist for a long time even after ChR was achieved by removing stimuli from H pylori-specific T cells.1 41
The probability of 5-year OS after H pylori eradication has been reported to be 82–96%.5 18 20 22 29 30 The probabilities of OS after 5 and 10 years in the present investigation were 99% and 95%, respectively (figure 2B), which was much better than those reported previously. By contrast, the prognostic factors for OS in gastric MALT lymphoma have rarely been analysed. In a report by Stathis et al,30 age, previous hepatitis C virus infection and performance status according to the Eastern Cooperative Oncology Group scale were associated with OS in the univariate analysis, and only age remained statistically significant in multivariate analysis. In our study, age and also non-superficial type were found to be independent prognostic factors for adverse OS by Cox multivariate analysis (see table C in online supplement).
Similarly, EFS in patients with gastric MALT lymphoma treated by H pylori eradication has been described in only a few publications,5 18 32 and a probability of 5-year EFS ranging from 67% to 85% has been reported. In our patients the probability of 5-year EFS was 92%, which was higher than that in previous reports. Pinotti et al reported that performance status and secondary malignancy were significantly associated with EFS.5 Another study reported that DLBCL component, deep submucosal invasion and age showed a significant association with EFS in univariate analysis, and that only deep submucosal invasion by EUS was significantly associated with EFS in multivariate analysis.18 In our current multivariate analysis, either non-superficial type or submucosal invasion was an independent prognostic factor for poor EFS (see table D in online supplement).
The development of synchronous or metachronous other malignant neoplasms has been observed in 1–20% of patients with gastric MALT lymphoma. Our analysis of pooled data from 32 studies found synchronous or metachronous cancers in 136 of 2300 patients (5.9%).5–32 42–45 Approximately 1–5% of patients with gastric MALT lymphoma developed metachronous gastric cancer after successful eradication of H pylori.18 20 23 25 30 32 We also confirmed an equivalent incidence of metachronous malignancies (8.3%) and gastric cancer (4.9%) in our study population. While the incidence of second malignancy in patients with gastric MALT lymphoma is not high compared with the general population,43 44 a study from Netherlands reported that the risk of gastric cancer in patients with gastric MALT lymphoma was significantly higher than in the general population.46 Longer endoscopic follow-up would be warranted even after CR by H pylori eradication to detect metachronous gastric cancer as well as relapse of lymphoma.
It is beyond doubt that patients with PD or clinically evident relapse should undergo oncological treatment. Radiotherapy and chemotherapy have a curative potential in localised gastric MALT lymphoma.34 We confirmed the high response rate of radiotherapy (94%) and chemotherapy (88%) as second-line treatments. On the other hand, the strategy for non-responders without PD or patients with histological relapse without DLBCL remains controversial. In our 10 responders it took more than 2 years from the eradication until confirmation of ChR/pMRD (data not shown). In addition, two other patients who showed histological relapse returned to ChR without any treatment. This presumably transient relapse or histological residual disease has also been reported in previous studies.8 15 18 20 27 A recent European consensus report recommends that patients with rRD or NC can be followed for up to 2 years by a ‘watch and wait’ strategy.34 We consider that ‘watch and wait’ follow-up can be prolonged for more than 2 years unless PD or relapsed endoscopic lesions can be demonstrated. The decision to continue a ‘watch and wait’ strategy or to start oncological treatment should be made based on multidisciplinary factors including H pylori status, clinical stage, presence of t(11;18) or DLBCL component.
There are some limitations in the present study. The retrospective nature seems to have been a source of selection biases. The OS and EFS in our patients might have been overestimated because patients who died within 3 years were excluded. The lack of the central review of all biopsy specimens might have induced some heterogeneity in the histological assessment. Patients in whom assessment of t(11;18) and EUS were not applied might have influenced the results of multivariate analyses for predictive factors. Nevertheless, these shortfalls did not hinder the main conclusions of the study.
In conclusion, this large-scale follow-up study shows that the long-term clinical outcome of gastric MALT lymphoma after H pylori eradication is excellent. An endoscopic appearance of non-superficial type is predictive of adverse FFTF, OS and EFS after H pylori eradication for patients with gastric MALT lymphoma. Based on these results, we propose that patients with stage I disease who achieved CR after H pylori eradication can be managed only by follow-up endoscopy with multiple biopsies every 1 or 2 years. Other staging procedures such as CT or PET are not required frequently. The metachronous development of gastric cancer should also be kept in mind, especially for patients who underwent radiotherapy or chemotherapy.
Acknowledgments
The authors thank the following members of the JAPAN GAST Study Group: Taiji Akamatsu (Matsumoto), Toshihiko Kudo (Toyama), Masahiko Nakamura (Tokyo), Tsuneya Nakamura (Nagoya), Shinji Tanaka (Hiroshima), Ken Haruma (Kurashiki), Tsutomu Chiba (Kyoto), Shigeaki Mizuno (Tokyo), Yuichi Akai (Tokyo), Koichi Eguchi (Fukuoka), Kunihiko Aoyagi (Fukuoka), Kazutoshi Hori (Nishinomiya), Shigemi Nakajima (Shiga), Masafumi Nishino (Hamamatsu), Mihoko Yamade (Hamamatsu), Mitsushige Sugimoto (Hamamatsu), Tadayoshi Okimoto (Oita), Takama Maekawa (Kyoto), Kazuto Ikezawa (Tsukuba), Tadashi Shimoyama (Hirosaki), Tosihiko Doi (Kashiwa) Motowo Mizuno (Hiroshima), and Hiroshi Inagaki (Nagoya).
References
Supplementary materials
Supplementary Data
This web only file has been produced by the BMJ Publishing Group from an electronic file supplied by the author(s) and has not been edited for content.
Files in this Data Supplement:
- Download Supplementary Data (PDF) - Manuscript file of format pdf
Footnotes
Funding This study was supported by Grants-in-aid from the Ministry of Education, Culture, Sports, Sciences, and Technology of Japan No. 20590744 (SN, TM).
Competing interests None.
Patient consent Obtained.
Ethics approval The ethics committee at Kyushu University Hospital.
Provenance and peer review Not commissioned; externally peer reviewed.