Article Text

Abstract
Background and aim: Gastro-oesophageal reflux disease (GORD) has been linked to a number of extra-esophageal symptoms and disorders, primarily in the respiratory tract. This systematic review aimed to provide an estimate of the strength and direction of the association between GORD and asthma.
Methods: Studies that assessed the prevalence or incidence of GORD in individuals with asthma, or of asthma in individuals with GORD, were identified in Medline and EMBASE via a systematic search strategy.
Results: Twenty-eight studies met the selection criteria. The sample size weighted average prevalence of GORD symptoms in asthma patients was 59.2%, whereas in controls it was 38.1%. In patients with asthma, the average prevalence of abnormal oesophageal pH, oesophagitis and hiatal hernia was 50.9%, 37.3% and 51.2%, respectively. The average prevalence of asthma in individuals with GORD was 4.6%, whereas in controls it was 3.9%. Pooling the odds ratios gave an overall ratio of 5.5 (95% CI 1.9–15.8) for studies reporting the prevalence of GORD symptoms in individuals with asthma, and 2.3 (95% CI 1.8–2.8) for those studies measuring the prevalence of asthma in GORD. One longitudinal study showed a significant association between a diagnosis of asthma and a subsequent diagnosis of GORD (relative risk 1.5; 95% CI 1.2–1.8), whereas the two studies that assessed whether GORD precedes asthma gave inconsistent results. The severity–response relationship was examined in only nine studies, with inconsistent findings.
Conclusions: This systematic review indicates that there is a significant association between GORD and asthma, but a paucity of data on the direction of causality.
Statistics from Altmetric.com
Gastro-oesophageal reflux disease (GORD) develops when the reflux of stomach contents into the oesophagus causes chronic troublesome symptoms or complications.1 The most recognisable symptoms of GORD are heartburn and acid regurgitation, but the reflux of noxious material may have wider-reaching effects. In addition to the well-established oesophageal complications associated with the disease,2 GORD is believed to lead to extra-oesophageal symptoms and complications, primarily in the respiratory tract.3 An association between GORD and asthma has been accepted for many years, and has been the focus of numerous studies and reviews.4,5 Asthma could arise as a result of acid reflux via two possible mechanisms: damage to the pulmonary tree after direct exposure to acid refluxate (reflux theory); or through bronchial constriction as a result of the stimulation of vagal nerve endings in the oesophagus (reflex theory).6 In addition, cough and increased respiratory effort may exacerbate GORD by bringing about an increased pressure gradient across the lower oesophageal sphincter.7 This could have particular relevance in patients with hiatus hernia, as gastro-oesophageal junction competence is compromised by hiatus hernia during intra-abdominal pressure increases.8
The aim of this systematic review is to provide a realistic estimate of the strength and direction of the association between GORD and asthma in adults. Despite the large number of publications examining the clinical and epidemiological nature of this association, ambiguity remains. For example, estimates of the prevalence of GORD in individuals with asthma vary from 30% to 90%.9 A particular challenge is that the prevalence of GORD has been measured in a number of different ways in the literature. First, symptom frequency and/or severity have been used as a measure of disease. This is a patient-focused method that can be used in large population-based surveys, but a definitive symptom cutoff point for disease has not yet been established. At least weekly heartburn and/or acid regurgitation is known to impair quality of life,10 and this definition has been used in a recent systematic review,11 which reported that 10–20% of the population in the western world have GORD. Oesophageal pH monitoring is a more objective way of measuring abnormal acid reflux, but its diagnostic accuracy is modest.12,13 Endoscopy is an objective way of examining for the presence of oesophagitis, but it cannot distinguish microscopic changes in the oesophageal mucosa that may underlie symptoms in some individuals. Erosive oesophagitis is present in approximately 20–40% of individuals with GORD.14–16
We have therefore chosen to review all of these different methodologies to gain a realistic picture of the association between the two diseases. We examined studies that assess the prevalence or incidence of GORD in individuals with asthma, and the prevalence or incidence of asthma in individuals with GORD. We have employed an epidemiological framework for causality that assesses the strength of association, the consistency of association, the temporal association between GORD and asthma, and finally, the severity–response association between the two diseases.
METHODS
Search strategy
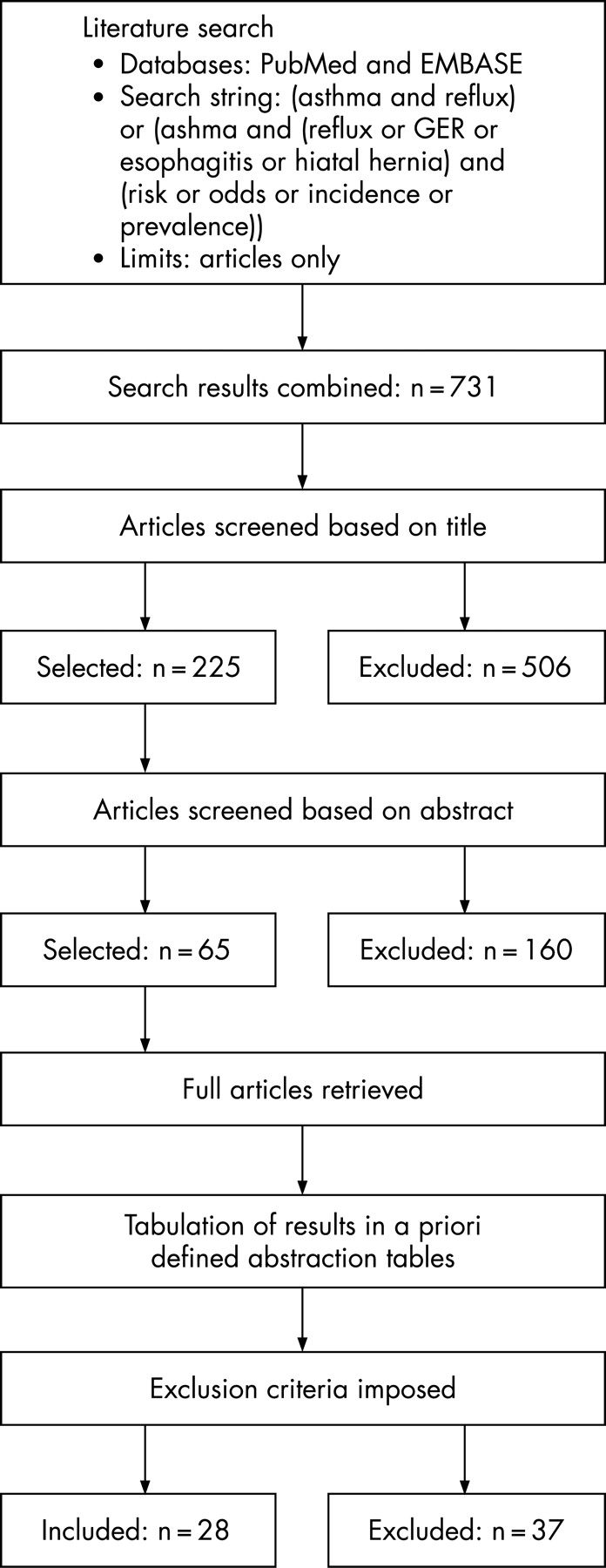
Studies published between 1966 and October 2006 were identified in Medline and EMBASE using the following combinations of search terms: ‘asthma and reflux’ and ‘asthma and (reflux or GER or oesophagitis or hiatal hernia) and (risk or odds or incidence or prevalence)’. There was no language restriction imposed on the search. Articles that potentially assessed the prevalence or incidence of reflux symptoms, abnormal oesophageal acid exposure, oesophagitis, hiatal hernia or Barrett’s oesophagus in adults with asthma, or the prevalence of asthma among adults with reflux symptoms or abnormal acid exposure were selected first based on the title, and then based on the abstract. Translations of relevant non-English language studies were obtained. Two independent investigators conducted the search and data abstraction.
Study selection
We sought to ensure as far as possible that the true prevalence of asthma was recorded. Studies conducted in a primary or secondary care setting were required to define asthma in accordance with American Thoracic Society (ATS) guidelines.17 Patients were therefore required to have the following: a previous diagnosis of asthma with a history of discrete attacks of wheezing, coughing or dyspnoea, and either an increase in the forced expiratory volume in one second (FEV1) of 20% from baseline after bronchodilator administration, or a decrease in FEV1 of 20% after methacholine bronchoprovocation.17 For population-based surveys or studies that included large administrative datasets, the definition of asthma did not need to meet the ATS guidelines. Studies describing the prevalence of reflux symptoms were required to give a description of the symptoms, including their severity and/or frequency. Studies that monitored oesophageal pH were excluded if the monitoring was performed for less than 24 hours. Studies were also excluded if the study cohorts were composed entirely of asthmatic patients referred for suspected GORD, or if the population source was not defined. Studies were excluded if they had a sample size of less than 50.
Tabulation of results
The full papers from the studies selected based on the content of their abstracts were analysed. A standardised abstraction form, constructed a priori, was used. The following data were collected: sampling frame, study design, sample size, control groups (if any), definition of asthma, definition of reflux symptoms, parameters for interpreting 24 hour pH study results, endoscopic findings, number of patients on medications for asthma and/or GORD, severity of asthma or GORD, and temporal relationships between the development of these conditions.
Analysis
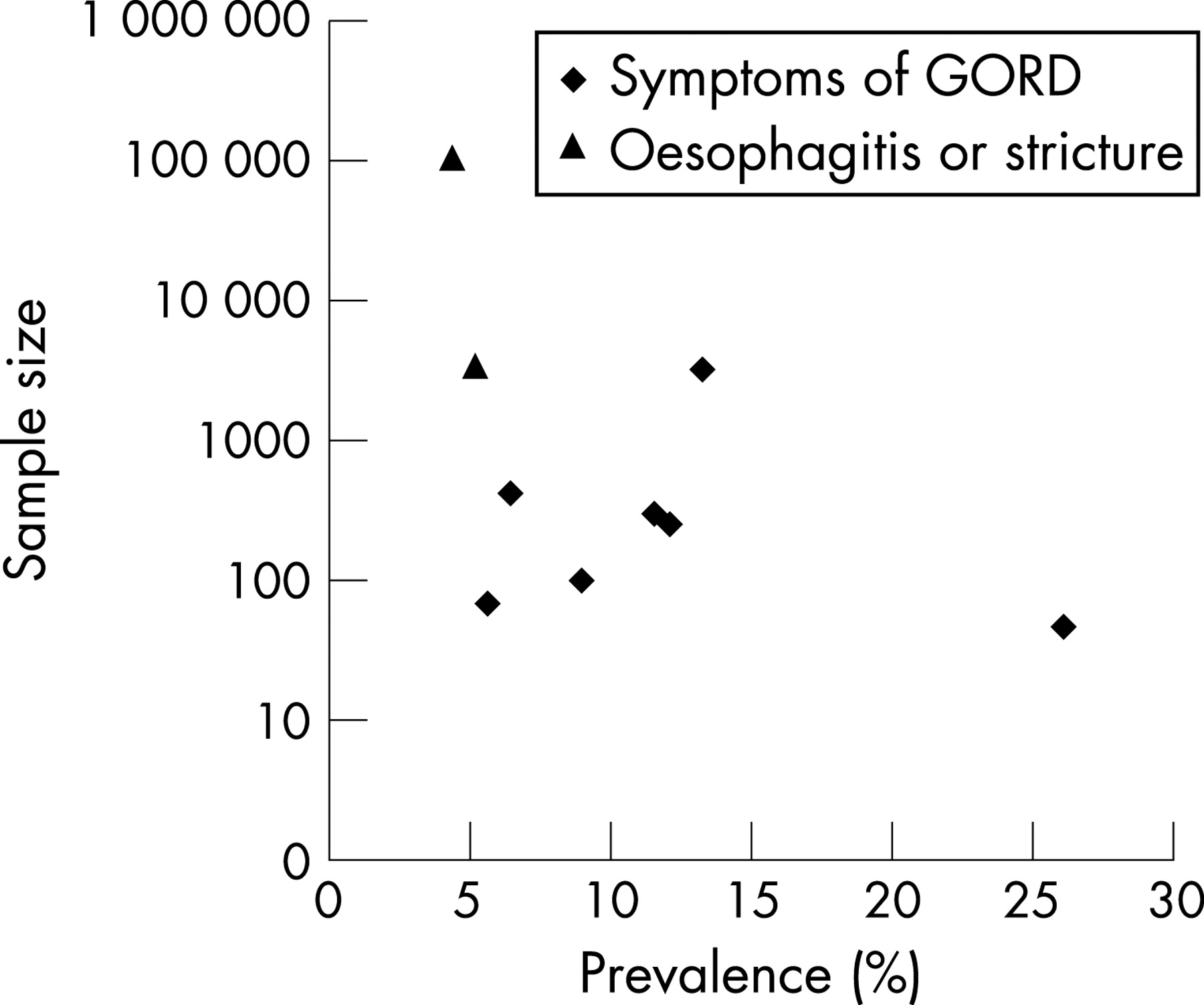
We determined overall prevalence estimates by pooling values from studies meeting the selection criteria and calculating average values weighted by sample size. For the studies reporting reflux symptoms, the average prevalence was calculated both with and without the studies reporting less frequent than weekly heartburn and/or acid regurgitation. Unadjusted odds ratios were pooled from studies that had included a comparison group to give overall estimates of the association between GORD and asthma. Heterogeneity was calculated using the I2 test. I2 is the percentage of total variation across studies caused by heterogeneity.18 Severity–response and temporal relationships were also identified and presented. Publication bias was examined by constructing funnel plots of the prevalence values from the included studies, which were tested for asymmetry using Macaskill’s test and the test proposed by Peters et al.19
RESULTS
In total, 65 relevant studies were identified, and 28 of these met our inclusion and exclusion criteria. The progression of studies through the search and selection process is illustrated in fig 1, and the number of studies in each subject area is shown in fig 2. Funnel plots indicate the absence of publication bias or a small study effect among the studies reporting the prevalence of GORD in asthma (Macaskill’s p _ 0.2461, modified Macaskill’s p _ 0.80; fig 3) and the presence of a possible small study effect among the studies of asthma in GORD (Macaskill’s p _ 0.002, Peters’ p _ 0.28; fig 4). One study reported both the incidence of GORD in patients with asthma, and the incidence of asthma in patients with GORD. Several studies reported prevalence estimates for reflux symptoms, abnormal oesophageal pH and endoscopic findings, making the total number of prevalence estimates higher than the total number of studies. Only studies in adults were selected, but a minority of the studies also included some children,20,21 and in some studies a lower age limit was not reported.22–27 In most of the included studies, the ratio of men to women was reasonably even (32–62% men). In one study, only 12% of the study population was male,28 and in several studies over 90% of the population was male.29–33



Symptoms of GORD in patients with asthma
We identified a total of 22 studies that reported the presence of symptoms of GORD in patients with asthma. Eight studies satisfied our criteria, and are detailed in table 1.20–22,28,29,34–36 Fourteen studies were excluded from the analysis, as described in table 2.23,24,37–48 Among the included studies, one was based on a large primary care administrative database and seven were performed in secondary care settings (table 1). Most of the studies were cross-sectional (n _ 7), whereas the database study was a longitudinal cohort study with nested case–control analysis. The pooled sample-size weighted average prevalence of GORD in asthma from the seven cross-sectional studies was 59.2%. The Montreal definition of GORD recommends that moderate heartburn and/or regurgitation at least weekly should be used as a cutoff point for disease in epidemiological studies,1 and this has been employed in a recent systematic review.11 When we only included those studies that reported the prevalence of at least weekly heartburn and/or acid regurgitation (n _ 5), the average prevalence of GORD was 58.4%. Three studies reported the prevalence of GORD in controls, with an average prevalence of 38.1%. Pooling the odds ratios from these studies gave an overall odds ratio of 5.45 (95% CI 1.89–15.76). At least 90% of patients with asthma used bronchodilators in the three studies in which this was reported.22,29,35 In the cohort study based on a large UK primary care database, the current use of oral or inhaled steroids was associated with a non-significant increased risk of GORD.20
Two studies of symptoms of GORD in patients with asthma warrant particular attention. By far the largest study was the cohort study by Ruigomez and colleagues,20 which measured the occurrence of a new diagnosis of GORD in UK primary care patients. The authors found a significantly higher incidence rate for GORD (eight cases per 1000 person-years; 95% CI 7.0–9.1) in those with a previous diagnosis of asthma than in controls (4.4 cases per 1000 person-years; 95% CI 3.9–5.0), indicating that patients with asthma were 1.8 times more likely to develop GORD than those without asthma.20 The second study of particular interest aimed to avoid bias by using a strictly consecutive recruitment protocol, excluding any patients who were referred to the study by other clinicians because of gastrointestinal symptoms.29 That study found a significantly higher prevalence of symptoms of GORD in patients with asthma compared with controls without asthma (OR 2.4; 95% CI 1.6–3.6).29 Asthma severity was directly related to the age of onset of reflux symptoms.29
Studies that monitored oesophageal pH in patients with asthma
We identified 32 studies in which oesophageal pH monitoring was performed in patients with asthma. Nine studies were included in the analysis (table 3),23–26,28,30,34,35,49 all of which were cross-sectional and had a secondary care setting. The pooled sample-size weighted average prevalence of abnormal oesophageal acid exposure in asthma patients was 50.9%. Only one study included a control group, but that study did not report the prevalence of abnormal acid exposure among the controls.30 Without any measure of the prevalence of abnormal acid exposure among controls, such as patients seen in a clinic other than an asthma clinic, it is not clear from the studies whether the rate of abnormal oesophageal acid exposure is higher than expected among patients with asthma or not. In total, 23 studies were excluded (table 4).37,39,41,43,50–68 All but one28 of the nine included studies reported medication use, and bronchodilators were widely used.
The US study by Sontag and co-workers30 found the highest prevalence of abnormal pH over 24 hours, at 81.8%, despite excluding patients who had a referral for GORD. That study considered more criteria in their analysis than other studies, examining the frequency of reflux episodes, acid contact times, and oesophageal acid clearance times measured using three different methods. Controls had significantly fewer reflux episodes (p _ 0.0001), shorter total acid contact time (p<0.0001) and shorter oesophageal clearance times (p _ 0.0001) than patients with asthma. When reported, there were no significant differences in medication use between patients with asthma who had normal and abnormal oesophageal pH.26,30,34,49
Five studies also reported, as sub-analyses, the prevalence of abnormal oesophageal pH particularly in asthma patients without the typical symptoms of GORD of heartburn and/or acid regurgitation, giving an overall prevalence of 10–50%.23,24,26,35,49 In one study,23 significant predictors of abnormal pH were nocturnal asthma symptoms (OR 7.7; 95% CI 1.8–32.7) and hoarseness (OR 6.6; 95% CI 1.8–24.1). The frequency of symptoms was not, however, described by the authors. Another study specifically reported the frequency of night-time asthma symptoms, but found no significant difference between patients with normal and abnormal oesophageal pH.49
Studies reporting the results of endoscopy in patients with asthma
We identified 18 studies in which endoscopy was performed in patients with asthma. Six studies satisfied our inclusion criteria (table 5),28,31,32,36,40,69 and 12 studies were excluded from the analysis (table 6).37,38,42,46,61–63,66,68,70–72 All of the included studies were cross-sectional and based in secondary care. The prevalence of erosive oesophagitis ranged from 27.8% to 47.4%, giving a pooled sample-size weighted average prevalence of 37.3%. The reported prevalence of hiatal hernia among patients with asthma ranged from 37.1% to 61.7%, giving a pooled sample-size weighted average prevalence of 51.2%. Only two studies included a control group, and in both studies there was a significant positive association between asthma and erosive oesophagitis or hiatal hernia (table 5).28,36
The level of bronchodilator use was not given in three of the studies.28,36,40 In the study by Sontag et al.,32 75% of patients used bronchodilators, and there was no significant difference between the prevalence of oesophagitis in those taking and not taking this medication. Bronchodilator use was similarly high (72%) in the study performed by Avidan and colleagues.31 In another study,69 although the level of bronchodilator use was not reported directly, the authors did state that drug consumption did not differ between those patients with oesophageal dysfunction (including hiatal hernia, oesophagitis, dysmotility or low lower oesophageal sphincter pressure) and those without. That study also found that frequent wheezing and cough was significantly more common among patients with oesophageal dysfunction than those without, but there were no significant differences in spirometric measurements between the two groups.
Asthma in individuals with GORD
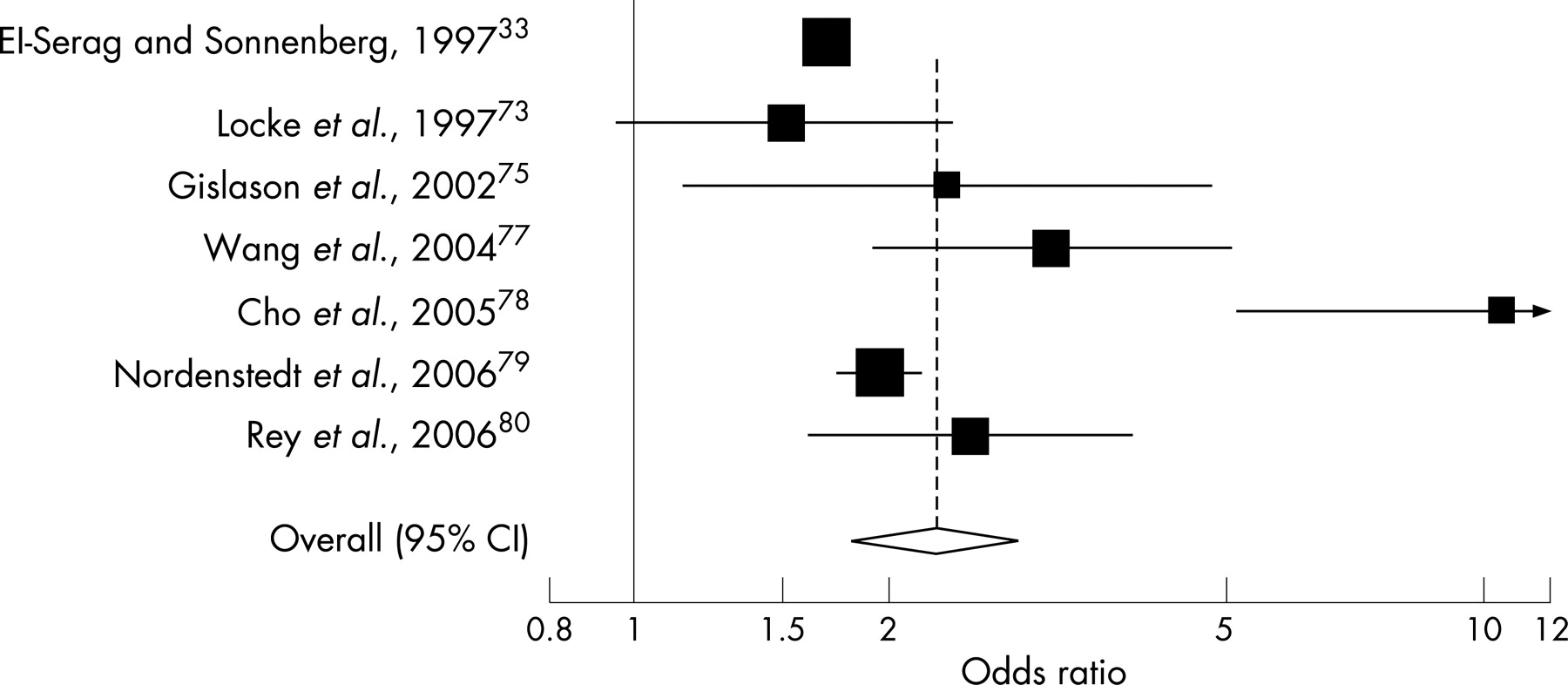
We identified a total of 15 studies that evaluated the presence of asthma in adults with GORD. Eleven studies met our inclusion criteria (table 7)20,27,33,73–80 and four studies were excluded (table 8).81–84 Of the included studies, nine were cross-sectional and two were cohort studies. Seven studies were general population surveys, three took their data from large administrative databases and one was based in secondary care. Nine studies reported the prevalence of asthma in individuals with GORD, giving an average prevalence of 4.6%. The average prevalence in controls was 3.9%, reported in seven of the studies. When only those studies that reported the prevalence of at least weekly heartburn and/or acid regurgitation were included (n _ 4), the average prevalence increased to 12.3%, largely because of the exclusion of a very large database study (n _ 101 366), which reported the lowest prevalence of asthma in GORD (4.3%).33 Overall, seven cross-sectional studies included a control group (table 7). Pooling the unadjusted odds ratios using a random effects model gave an overall odds ratio of 2.27 (95% CI 1.814–2.834; fig 5). The calculated I2 was 85%, however, indicating considerable heterogeneity. Six of those studies with controls were population based and were thus considered to be of high generalisability. When only those studies were included in the analysis, the pooled odds ratio was 2.68 (95% CI 1.82–3.96) and the I2 test gave a value of 81%. Only one study reported medication use, finding no association between the current use of gastrointestinal drugs and the occurrence of asthma.20

There were two cohort analyses that reported incidence estimates for asthma in individuals with GORD, or a complication associated with GORD. One of these, which was a follow-up study from the third US National Health and Nutrition Examination Survey (NHANES III), found that the incidence rate of hospitalisation as a result of asthma in patients who had had previous hospitalisation for hiatal hernia or oesophagitis was 2.6 cases per 1000 person-years, whereas in controls without hiatal hernia or oesophagitis it was 1.0 cases per 1000 person-years.74 The other study used a UK primary care administrative database, and found an incidence rate of a new diagnosis of asthma among patients with an existing diagnosis of GORD of 6.0 (95% CI 4.9–7.3) per 1000 person-years.20 In patients without a previous diagnosis of GORD, the incidence rate of asthma was significantly lower at 3.8 cases (95% CI 3.1–4.6) per 1000 person-years.
Severity–response relationship between GORD and asthma
Only three of the studies evaluating the presence of symptoms of GORD in individuals with asthma considered whether the severity of asthma had an impact on the presence, severity or frequency of GORD symptoms. One study from Italy found that a greater proportion of patients with severe asthma experienced at least twice weekly heartburn and/or acid regurgitation than those with mild or moderate symptoms (p<0.03).21 Reflux symptoms were present in 30% of patients with mild asthma, 46% of those with moderate asthma and 70% of those with severe asthma.21 In a cross-sectional study from Spain,34 a composite score for GORD was calculated based on the percentage of time that pH was less than four in upright and supine positions and in total, the number of reflux episodes in total, the number of reflux episodes longer than five minutes and the duration of the longest reflux episode. The value of this composite score was similar in patients with mild asthma (median 8.8; range 8.0–22.1), moderate asthma (median 9.5; range 7.9–144.5) and severe asthma (median 10.5; range 8.0–66.6).34
Vincent and colleagues26 found that in patients with GORD, there was a very strong association between the provocative dose of methacholine causing a 20% fall in FEV1 and the number of oesophageal reflux episodes (p<0.001). There were, however, no other correlations between lung function (FEV1 or mean expiratory flow) and GORD criteria (percentage of 24-hour period with oesophageal pH<4, number of reflux episodes or lower oesophageal sphincter pressure).
Only two endoscopy studies examined the association between the severity of asthma and the severity of endoscopic findings. Overall, they indicated that more severe asthma is associated with an increased risk of GORD. In one study from Japan,40 patients with intermittent, mildly persistent or moderately persistent asthma had a lower mean endoscopic grade of oesophagitis than patients with severe asthma (p<0.05). In the other study,36 also from Japan, patients with mild asthma were most frequently classified as having no apparent mucosal changes, those with moderate asthma most frequently had minimal changes, and those with severe asthma most frequently had oesophagitis of Los Angeles grade A (mucosal break ⩽5 mm).
In the studies that examined the presence of asthma in individuals with GORD, the severity of GORD defined by the frequency of reflux symptoms was associated with a higher prevalence of asthma in three studies (fig 6).73,78,80 Another study found that there was a higher prevalence of asthma among patients who had GORD and erosive oesophagitis (169/2114, 5.2%) than those who had GORD without erosive oesophagitis (127/2065, 4.3%).76

{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
Temporal sequence relationship between GORD and asthma
The temporal relationship between GORD and asthma was investigated in two studies.20,74 One of those studies,20 which used the UK General Practice Research Database, found a clear association between the presence of a new diagnosis of asthma and the subsequent development of GORD in a multivariate analysis adjusted for age, sex, smoking, previous morbidity and healthcare utilisation (RR 1.5; 95% CI 1.2–1.8). That study also assessed the likelihood of GORD preceding asthma, showing a non-significantly increased risk of a new diagnosis of asthma among patients with GORD compared with those in the control cohort without GORD (RR 1.2; 95% CI 0.9–1.6).20 The longitudinal US study that used the NHANES III data74 showed an increased likelihood of hospitalisation as a result of asthma in individuals who had previously been hospitalised with oesophagitis or hiatal hernia (RR 2.1; 95% CI 1.1–4.2).
DISCUSSION
The findings of our systematic review support a significant association between GORD and asthma. The pooled prevalence values indicate that the prevalence of symptoms of GORD among individuals with asthma is substantially higher (1.6-fold) than in controls. Similarly, although to a lesser degree, the average prevalence of asthma in individuals with GORD is also higher than in controls (1.2-fold). The average prevalence of reflux symptoms in adults with asthma was 59%, and the prevalence of erosive oesophagitis was 37%. The average prevalence of GORD diagnosed by pH monitoring was 51%. These values in individuals with asthma are substantially higher than those reported in the general population (10–20% for GORD symptoms, 7–16% for erosive oesophagitis11,14,15,85). None of the studies reporting the prevalence of GORD in asthma were population based, however, and some of this difference may be because the subjects came from selected primary and secondary care populations.
Although there appears to be a strong association between GORD and asthma, most of the studies included in our analysis were cross-sectional or case–control in design, and therefore could not give a clear indication of the temporal sequence of these conditions, an important criterion for causal associations. The temporal sequence between GORD and asthma was explored in only two studies. The single study that assessed whether primary care patients with asthma were at an increased risk of subsequently developing GORD found a significantly increased incidence of GORD among those patients compared with controls. That and another study reported the likelihood of GORD preceding asthma, with inconsistent findings. Similarly, the severity–response relationship, another criterion for a causal association, was reported in a minority of studies. Results were again inconsistent, but tended towards a positive correlation when the increasing severity of GORD (based on either increasing symptom frequency or the increasing severity of oesophagitis) was associated with an increase in the prevalence of asthma. In several studies, increasingly severe asthma was associated with an increased prevalence of symptoms of GORD or severity of GORD. As a result, the available evidence does not yet clearly indicate whether GORD precedes asthma, or asthma triggers GORD. The recently published Montreal definition of GORD concludes that GORD can be an “aggravating cofactor” in asthma.1
In addition to statistical association and temporal and severity–response relationships, the controlled introduction or removal of stimuli related to one condition (such as GORD) and the corresponding response (such as the effect on asthma symptoms or pulmonary function) have been used to examine the potential for a causal relationship between the two conditions. This has been investigated using oesophageal acid perfusion testing, but no consistent effect has been found.86 GORD treatment in patients with asthma has also had mixed results. A recent systematic review showed minimal improvement of asthma symptoms with GORD therapy, but no improvement in objective pulmonary function indices.87 Antireflux therapy does, however, allow a reduction in asthma medication use.4 This difference in effect may be related to the fact that pharmacological treatments for GORD change the composition of refluxate without preventing reflux itself, whereas antireflux surgery reduces the number of reflux events. It may be that only some patients are sensitive to acid reflux, or that GORD may affect asthma symptoms but not the pulmonary function measures used in those studies.4,9 For example, increased respiratory effort could be a result of the pain of heartburn causing increased minute ventilation rather than triggering bronchospasm. Even if asthma is GORD related, in some cases there may be resistance to GORD treatment through chronic or irreversible changes.
Our systematic review has both strengths and limitations. We present the most comprehensive systematic review of the epidemiological and clinical literature in this area. In particular, consistent definitions of GORD and asthma provide as true a representation of the prevalence of these diseases as possible. The results of our statistical funnel plot testing argue against the presence of publication bias. We have attempted to minimise selection bias by excluding studies in which investigated asthma patients were referred on the basis of a suspicion of underlying GORD. Most of the studies included in our review were, however, based in secondary and tertiary referral centres and thus have limited generalisability because they are subject to selection bias. In particular, the results from endoscopic and oesophageal pH monitoring studies may have limited generalisability because a large proportion of eligible patients will not give consent for these invasive and sometimes uncomfortable procedures, especially if the procedure is for the purpose of research only. Most studies had no internal controls and this aspect may have led to an overestimation of the association between GORD and asthma, as patients with difficult-to-control disease or suspicion of another causative factor may be overrepresented in these populations. Although we did not employ formal scoring of the studies in this review based on quality, we did perform a secondary analysis of studies with greater generalisability including only those that were population based and included internal controls. Six studies measuring the prevalence of asthma in individuals with GORD met these generalisability criteria, and the pooled odds ratios from those studies were indicative of a significant positive association between GORD symptoms and asthma.
Although there are a great many studies reporting the prevalence of GORD in individuals with asthma, and vice versa, we found very few population-based studies, and very few studies that considered the temporal sequence relationship between the two diseases. This type of epidemiological research would add to our understanding of the link between GORD and asthma. Prospective studies of individuals with GORD that include long-term follow-up and systematic testing for the incidence of asthma, and vice versa, would be the most valuable strategy. Further studies should also evaluate the severity–response relationship between the two diseases. Ideally, studies should include internal controls and adequate numbers of patients to avoid type 2 errors. They should also document, using validated and reproducible measures, the severity of asthma, GORD and oesophagitis. Age is an important factor in relation to the onset of asthma. Most asthma diagnoses are made in childhood, whereas most ‘difficult to control’ asthma is thought to originate in adult life.88 It would be interesting to investigate whether age plays a role in GORD-related asthma.
In conclusion, this systematic review quantifies the prevalence of GORD in individuals with asthma, and asthma in GORD, and so contributes to our understanding of the association between these two diseases. It also highlights that, despite the enormous volume of literature that exists on the subject, there is a shortage of high-quality data. We have identified a clear paucity of data on the direction of the temporal sequence association. Addressing this should be a focus for future epidemiological research in this area.
Competing interests: Declared (the declaration can be viewed on the Gut website at http://www.gutjnl.com/supplemental).
REFERENCES
Supplementary materials
Competing interests: Dr C. Henderson is an employee of Oxford PharmaGenesis Ltd, which has received funding from AstraZeneca R&D M�lndal, Sweden.
Footnotes
Funding: This study was funded by a research grant from AstraZeneca R&D Mölndal, Sweden.
- Abbreviations:
- ATS
- American Thoracic Society
- GORD
- gastro-oesophageal reflux disease
Linked Articles
- Digest