Article Text

Abstract
Background: Tuberculosis (TB) remains an important infectious disease in New Zealand (NZ) and globally, but risk factors for transmission are still poorly understood. This research aimed to identify whether household crowding contributes to TB transmission in NZ.
Methods: This ecological study used TB surveillance and census data to calculate TB incidence rates by census area unit (CAU). Census data were used to determine CAU characteristics including proportion of household crowding (a bedroom deficit of one or more), proportion of population who are migrants born in high-TB-incidence countries, median household income, and deprivation level. A negative binomial regression model was used to estimate the association between TB incidence and household crowding.
Results: The analysis included 1898 notified TB cases for the 2000–4 period. Univariate analysis showed TB incidence at the CAU level was associated with household crowding, for the total population and for all ethnic and age groups. After adjusting for the covariates of household income, existing TB burden, and proportion of migrants from high-TB-incidence countries, multivariate analysis showed statistically significant associations between TB incidence and household crowding. The incidence rate ratio (IRR) was 1.05 (95% CI 1.02 to 1.08) in the total population and 1.08 (95% CI 1.04 to 1.12) for NZ-born people <40 years.
Conclusion: At the CAU level, TB incidence in NZ is associated with household crowding. An individual-based study (e.g. case–control) in recently infected cases (detected by molecular epidemiology techniques) is suggested to complement these findings. Reducing or eliminating household crowding could decrease TB incidence in NZ and globally.
Statistics from Altmetric.com
Tuberculosis (TB) is associated with poverty and deprivation.1–9 Household crowding is one manifestation of poverty and could be a mechanism that mediates the link between TB and deprivation. A small but significant proportion of the New Zealand (NZ) population live in conditions of relative poverty and in overcrowded houses.10 TB incidence rates have not declined in NZ for the past two decades and, although the main source of new cases is immigration from high-TB-incidence countries, local transmission continues to occur.11
A few studies in New Zealand 12 13 and several studies abroad 2 4 6–8 14–25 have explored the relationship between household crowding and TB incidence. However, the importance of this risk factor remains unresolved because of inconsistent findings, a reliance on ecological design, and the failure to control for potential confounders in many studies.
Previous NZ research found that the incidence of TB from 1999–2003 was higher in census area units (CAUs) with higher levels of crowding in all age and ethnic groups.13 That study used a univariate analysis so the association of higher TB incidence and household crowding was not adjusted for potential confounding factors, such as deprivation level or migration from high-TB-incidence countries. In the Wellington region, a retrospective ecological study found an association between TB notification and household overcrowding, but also did not control for immigration from high-TB-incidence countries.12
One characteristic of TB disease is a variable period of latency (sometimes decades) following infection. This feature makes it difficult to attribute observed disease rates to current environmental exposures and risk factors, particularly where populations include immigrants from high-TB-incidence countries. One way to sidestep this complication is to consider only younger cases, who are more likely to have developed TB from recent exposure. There is conflicting evidence in the literature on the association between childhood TB and household crowding. One ecological study found an association between crowding and TB disease in children,14 and one cross-sectional study of the household contacts of cases found that TB infection was significantly more common when the children came from crowded households.26 By contrast, another ecological study found that household crowding developed a protective effect after adjusting for significant risk factors such as low income, more ethnic minorities and more immigrants.8
Only a few case–control studies have investigated the risk of TB associated with household crowding.6 9 23 25 27–30 Of the six studies carried out in medium- to high-incidence countries (Gambia, West Africa, India, Thailand, Russia, Estonia), four found a significantly elevated risk of TB associated with measures of household crowding and household size,9 23 29 30 one found a marginally increased risk,6 and one found no risk.25 One of the few case–control studies from a relatively low incidence region (Liverpool) did not find an independent effect from household crowding.28 And one case–control study of latent TB infection in New York children aged 1–5 years found a non-significant elevated risk associated with household crowding in univariate analysis.27
Here, routinely collected TB surveillance and census data were analysed to determine whether household crowding contributes to the incidence of TB in NZ. This hypothesis was tested in the total population and in the subset of those aged <40 years, born locally. In this latter group, disease is more likely to represent new cases of infection (ie recently acquired progressive disease) compared with older populations and immigrant populations from high-TB-incidence countries where reactivation of pre-existing infection is relatively more important.
METHODS
Data description and definitions
TB surveillance data—The Institute of Environmental Science and Research Limited (ESR) is responsible for TB surveillance at the national level and provided TB notifications for 1995–4.11 TB notifications were analysed by CAU for 2000–4 using the number of TB cases in each CAU notified between 1995–9 as a measure of the pre-existing TB burden. The notification data were anonymised, so specific ethics committee approval for the project was not considered necessary.
Population data—Statistics NZ conducts a census of population and dwellings every five years. The 2001 census data provided population demographic information by age, ethnicity, migrations status and country of origin, socioeconomic deprivation, median household income and household crowding at the CAU level.
Census Area Units—CAUs are non-administrative geographical areas. In main or secondary urban areas they generally coincide with suburbs, and normally contain a population of 3000–5000. In rural areas they cover larger geographic areas, but may have smaller populations.
Household Crowding—Relates to situations where the number of people residing in a household exceeds the ability of the dwelling to provide adequate shelter and services to its members.10 There is no internationally agreed standard definition of crowding. This report defines a crowded household as one, where depending on the age, sex and relationship of the household members, one or more additional bedrooms are required. This measure has been developed by the Canada Mortgage and Housing Corporation and is called the Canadian National Occupancy Standard (CNOS). Statistics New Zealand used this standard in its recent report on household crowding.10
Household Income—Jensen Equivalised Annual Household Income for households in private occupied dwellings is a measure of total household income adjusted for household composition.10
Deprivation—The New Zealand Deprivation Index (NZDEP) is an area-based summary measure of deprivation constructed from census data using nine variables based on the proportions of a population in the following categories: 18–59-year-olds on a means-tested benefit; with income below a particular equivalised threshold; 18–59-year-olds unemployed; with no access to a telephone and no access to a car; aged <60 and living in a single parent family; 18–59-year-olds without any qualifications; living in households above equivalised bedroom occupancy threshold; and not owning a home.31 For comparison purposes, CAUs were grouped into quintiles of NZDEP scores (constructed from 2001 census data).
High-TB-incidence countries—The New Zealand Ministry of Health has defined high-TB-incidence countries as all countries except Australia, Austria, Belgium, Canada, Czech Republic, Denmark, Finland, France, Germany, Greece, Holland, Iceland, Ireland, Israel, Italy, Luxembourg, Malta, Monaco, NZ, Norway, Slovakia, Sweden, Switzerland, the UK and USA.32 This definition was used to identify migrants born in high-TB-incidence countries.
Using the TB surveillance data and Census 2001 data, the explanatory and outcome variables were computed at the CAU level, as shown in table 1.
Theoretical framework
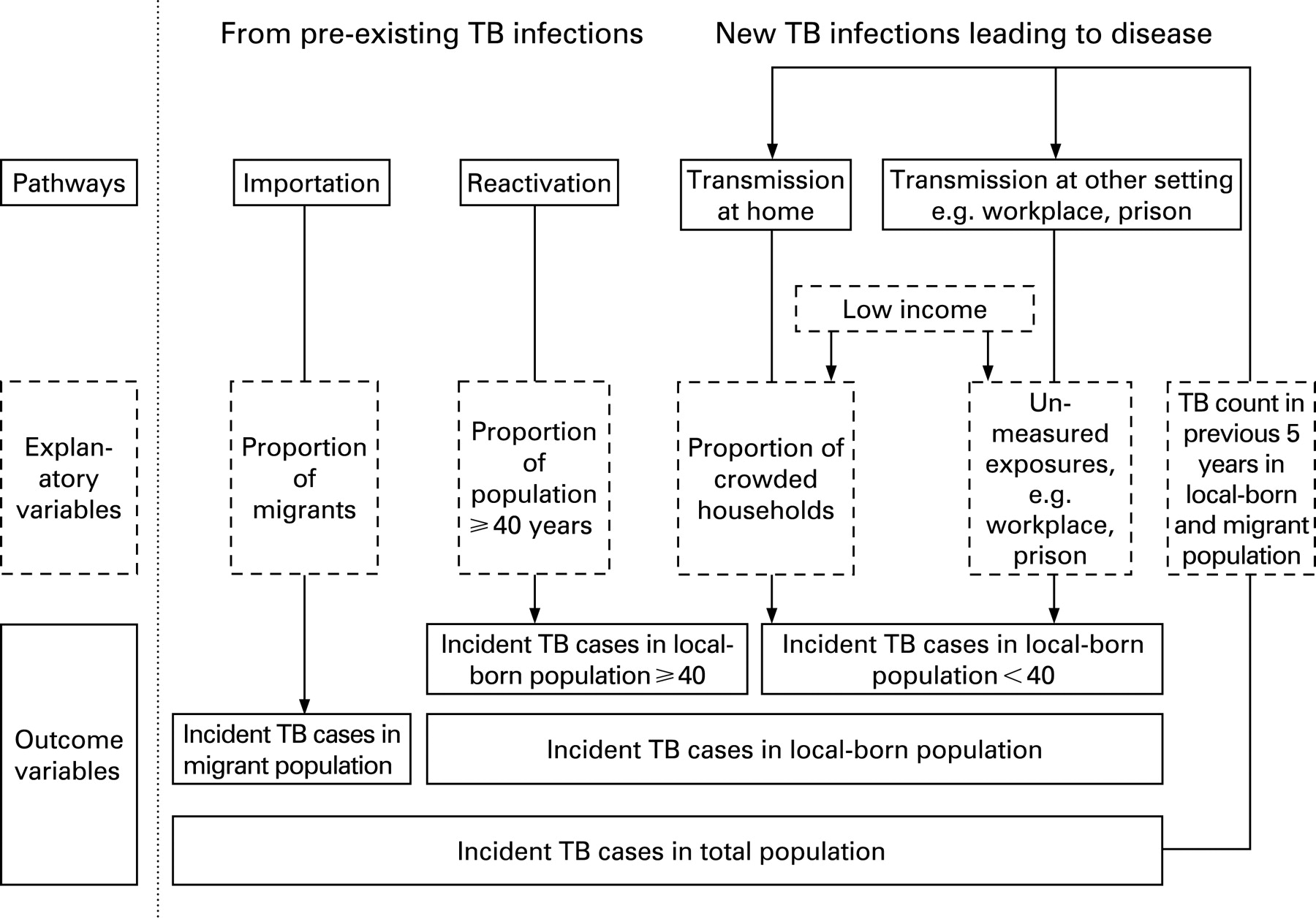
Guided by the local epidemiology of TB,11 33 a theoretical framework was conceptualised for development of TB in NZ through two broad pathways (figure 1). One pathway was from pre-existing infections, possibly acquired many years ago. Most migrants born in high-TB-incidence countries and elderly people who develop TB are likely to do so through this pathway. The other pathway was through local and relatively recent transmission of infection and subsequent development of the disease. Young NZ-born TB patients are more likely to have developed TB through this second pathway. These pathways and the main explanatory and outcome variables used in the multivariate analysis are shown in figure 1.

Development of TB in the first pathway (from pre-existing infection) is unlikely to be due to current living and crowding conditions. Current household crowding is more likely to contribute to TB in the second pathway (recent infection). Consequently, in addition to analysing the entire NZ population, the relationship between crowding and TB incidence was also considered in the subset of cases in NZ-born people <40 years (TBNZ<40), which included 321 (16.9%) of the total notified cases during 2000–4. The analysis also compared TB rates in migrants and NZ-born patients ⩾40 years. For the sub-model involving only NZ-born people aged <40 years, some of the explanatory variables were recalculated or modified. For example, CAU level income (INCOMENZ<40) and household crowding (PCROWDNZ<40) variables used in the sub-model were derived from census data, but limited to households with at least one NZ-born person aged <40 years (table 1).
Whatever the level of household crowding, TB transmission can only occur if there is a source case of infectious TB. The total number of incident TB cases in the previous five years (TB5YR) is an indicator of the magnitude of this source in each CAU and was included in this model.
Statistical analysis
Both univariate and multivariate methods of analysis were used, as described below. All analyses were done for the total population (full model) and then repeated for the subset of NZ-born people aged <40 years (sub-model). Data were analysed using the STATA 9.0 software program.34
Univariate analysis
Spearman’s correlations between TB rates and the explanatory variables were examined in the total population. Correlation coefficients of >0.6 were considered important for potentially confounding parameter estimates in the regression model.
TB rates were calculated and plotted by CAU quintiles of crowding, migrants born in high-TB-incidence countries, income, and deprivation to identify patterns of association. This analysis was done for the total population, NZ-born people aged <40 years (sub-model), NZ-born people aged ⩾40 years, and migrants from high-TB-incidence countries.
Multivariate analysis
As TB notifications are counts and rare events, a negative binomial model (NBM) was used. In the full model, the counts of incident TB cases were entered for the five-year period (2000–4) as the dependent variable (TBTOT). To control for over-dispersion, the expected count of the TB cases in each CAU as a weighting factor was also introduced. The log of the total population in each CAU was used as the offset variable. The intention was primarily to explore the relation between TB incidence and crowding (PCROWD), controlled for proportion of population who are migrants born in high-TB-incidence countries (PMIG) and socioeconomic status (INCOME). To avoid multicollinearity, other explanatory variables with a high correlation with any of these variables (the ethnic composition variables of PEUR, PMAO, PPAC, POTH) were not included in the model. The following explanatory variables were retained in the full model: PCROWD, PMIG, INCOME, P<40 and TB5YR (see table 1 for a description of variables). For the sub-model (NZ-born people aged <40 years), the dependent variable was TB count in NZ-born people <40 years of age (TBNZ<40) and the explanatory variables were PCROWDNZ<40, PMIG, INCOMENZ<40, P<40, TBMIG5YR and TBNZ5YR.
RESULTS
The 2001 Census included 1860 CAUs. Of these, 719 CAUs had at least one TB case in the 2000–4 period. The total usually resident population in NZ in the 2001 Census was 3 737 277. The total TB cases notified in the 2000–4 period were 1898. About 60% of these cases occurred in migrants born in high-incidence countries.
Univariate analysis
Crude TB rates were calculated and plotted according to the quintiles of explanatory variables of interest (PCROWD, PMIG and INCOME). These results are shown for the total population, NZ-born people aged <40 years (sub-model), NZ-born people aged ⩾40 years and migrants from high-TB-incidence countries.
Crude TB rates increased significantly (chi square test for trend p<0.05) with crowding quintiles for the total population, migrants from high-incidence countries and the NZ-born population ⩾40 years (fig 2). For all groups, the most crowded quintile (quintile 5) had the highest TB-incidence rates.

The pattern of TB rates according to the proportion of migrants born in high-incidence countries (fig 3) was less consistent than for crowding. Crude TB rates in the migrant population were significantly (chi square test for trend p<0.05) higher in CAUs that had a large migrant population from high-TB-incidence countries. However, there was no consistent pattern for other subpopulations or for the total population.

{kind=link}
{kind=link}
{kind=link}
TB incidence did not have a consistent relationship with mean equivalised household income. In NZ-born people, TB incidence generally decreased with rising income, though this trend was only significant (chi square test for trend p<0.05) for NZ-born subpopulations. No such trend was observed in migrants born in high-incidence countries nor in the total population.
TB incidence in the total population was correlated, at the CAU level, with all of the explanatory variables except income. In addition, high correlations (⩾0.6) were noted between crowding (PCROWD) and ethnic composition variables (PEUR, PMAO) and also between the proportion of immigrants born in high-TB-incidence countries (PMIG) and ethnic composition (PPAC and POTH).
Multivariate analysis
Results of the multivariate analysis using the negative binomial regression model are presented in table 2. These results show that in the full model (total population), TB rates were significantly associated with crowding (PCROWD) after controlling for migration from high-TB-incidence countries (PMIG), median income (INCOME), proportion of people aged <40 years (P<40) and existing TB burden (TB5YR). In the sub-model, incident TB cases (TBNZ<40) were significantly associated with Income (INCOMENZ<40) and P<40. While PMIG was statistically significant in the full model, it was not significant in the sub-model (in NZ-born people <40). Existing TB burden (TB5YR in full model or TBMIG5YR and TBNZ5YR in sub-model) did not make a statistically significant contribution, either in the full or in the sub-model.
The incidence rate ratio (IRR) of 1.05 in the full model means that for every 1% increase in the average crowding level of a CAU there would be a 5% increase in the expected TB count in that CAU, assuming the other variables were held constant. This means that if the least crowded quintile of housing was used as a reference (median crowding level of 0.94%), the TB count in the most crowded quintile (median crowding level of 9.49%) would be expected to be approximately 41% higher if all the other variables were held constant (based on an approximately 8% increase in crowding level). For the sub-model, with an IRR of 1.08, the effect would be even stronger with the expected TB count approximately 71% higher in the most crowded quintile.
DISCUSSION
The findings of this study suggest that household crowding is contributing to TB incidence in NZ. A multivariate analysis showed that TB incidence in the total population was associated with both the level of household crowding and the proportion of migrants from high-TB-incidence countries within the CAU. It was also found that in an analysis focused on the subgroup of people likely to have been infected more recently in NZ (NZ-born people aged <40 years), household crowding continued to be significantly associated with TB incidence. However, TB incidence among NZ born people <40 years was not significantly associated with the proportion of the CAU population who were migrants born in high-incidence countries. This finding suggests that migrants are not an important source of infection for the NZ-born population. The assumption that TB burden in the CAU over the previous five-year period would be a predictor of subsequent TB incidence was not supported in either of the models.
The finding that TB rates are associated with crowded living conditions is hardly surprising from what is known about the effective transmission of this bacteria in households via small droplet nuclei.35 What is perhaps surprising is the small number of reported studies that have attempted to investigate and quantify the importance of TB risk factors using robust analytical methods. Only one case–control study of TB carried out in a low-incidence developed country could be found.28 While that study did not find any association between TB and household crowding, this result could have been caused by the high level of control matching that it used (postcode and ethnicity, as well as age and sex).28 By contrast, more than 20 ecological studies could be identified that investigated risk factors for TB in developed countries by correlating disease rates in small geographical areas with census-derived demographic and socioeconomic factors. Of these, eight studies 2 4 7 8 16 17 20 24 included a specific measure of household crowding along with use of multivariate methods to control for sociodemographic factors and migration. All but one of these studies found a positive association between TB risk and levels of household crowding.8
The strengths of this study were the ability to control for covariates, the large number of units for analysis, the investigation of the association in the NZ-born <40-year subgroup, and use of a conceptual framework based on existing evidence about TB transmission pathways. In this study, unlike some previous studies, the association between household crowding and TB incidence remained statistically significant even after controlling for migration from high-TB-incidence countries.8
A possible weakness of this research was that several potential confounders were not included in the regression models. Two of the four ethnicity variables (PPAC and POTH) were highly correlated with the proportion of migrants from high-TB-incidence countries (PMIG), and two (PEUR and PMAO) with crowding (PCROWD). To avoid multicollinearity, the ethnicity variables were not put into the model. Consequently, this study was not able to determine whether ethnicity (particularly non-European ethnicity) has an independent effect on the risk of TB, over and above that mediated through household crowding and low income. Determining whether ethnicity does indeed have an independent effect on TB risk will require further study, probably using individual level data. Also, it would have been ideal to use a variable representing deprivation or socioeconomic status, but not containing crowding, and fitted this to the regression model. Because the New Zealand deprivation index (NZDEP) includes household crowding, it was considered inappropriate to include this variable in the model. Instead another indicator of socioeconomic status—median equivalised household income—was fitted into the model. As expected, income was negatively and significantly associated with TB incidence in the multivariate models (table 2).
The proportion of people aged <40 years in a CAU was negatively associated with incident TB cases in the multivariate analysis (table 2), but positively associated in the univariate analysis. The opposite direction of the association in the two models could be explained by the effect of migration. The main driver of TB incidence in NZ is migration from high-TB-incidence countries,33 and cases in this population are generally younger than NZ-born cases.11 When the proportion of high-TB-incidence country migrants was controlled for in the multivariate model, the effect of younger people (P<40) in a CAU, independent of the proportion of migrants from high-TB-incidence countries was revealed as negative.
Other analysis methods were investigated. An attempt was made to construct a regression model with ‘standardised TB notification ratio’ (indirectly age standardised notification rate), as done by some other researchers.16 However, in the present study this alternative model was a poor fit. Moreover, this approach is not considered appropriate for comparing rates in different geographic areas.36 Poisson models are widely used in the regression analysis of count data. The Poisson model was first fitted to the TB count data. The counts displayed substantial extra-Poisson variation or over-dispersion relative to a Poisson model. Consequently, the data was modelled using a NBM, a zero-inflated Poisson (ZIP) model and a zero-inflated negative binomial (ZINB). The Vuong test of ZINB versus the standard negative binomial did not favour either model. The NBM models between-subject heterogeneity has been used recently in a similar ecological study of TB and transmission in California.8 It was, therefore, considered the preferred approach.
The ‘ecological fallacy’ is a limitation of ecological studies. Although an association was found between overall crowding levels in CAUs and TB incidence, due to lack of individual data it is not clear that cases were from crowded households. However, this may not always be a valid concern. MacRae argued that association between socioeconomic deprivation and health status found in ecological studies should not be ignored on the grounds of ecological fallacy.37 It is likely that living in a crowded CAU increases the risk of living in a crowded household, which in turn affects individual TB risk, which can be classified as an indirect cross-level effect.38
Another limitation is that the census did not include a measure of crowding levels outside the household. Houses are only one of the several settings where TB transmission can occur (see fig 1). Other sites include prisons,39 churches40 and workplaces,41 which are well recognised and have all been documented in New Zealand. The possibility cannot be excluded that the association observed between household crowding and TB incidence is due to CAUs with high levels of household crowding also containing populations having high exposure to crowding in other settings.
Determining whether TB developed from recent infection or from reactivation of old infection is not accurate with conventional epidemiologic techniques. Dividing all TB cases into <40 and ⩾40 year age groups, and assigning recent transmission to <40-year-olds and reactivation to those ⩾40 is logical but somewhat arbitrary. Molecular techniques are a promising tool for differentiating these two groups and also for shedding light on the relationship between immigration and TB in the non-immigrant population.42 Cases arising from recent TB transmission are detected even in elderly populations when molecular methods are combined with classical epidemiology techniques such as contact tracing.42–44
Further New Zealand research could use a case-control or cohort design to investigate risk factors at the individual level, ideally combined with molecular techniques to identify and focus on the subgroup of recently infected cases. Such studies would help clarify the relation between household crowding and TB risk, particularly if they included other known TB risk factors and potential confounders such as smoking status.45 A further refinement to these models would be to use a more specific indicator of the level of exposure to TB infection in the community, such as incident cases of infectious pulmonary disease, as a replacement for total number of incident cases.
In conclusion, findings from this study suggest that TB incidence in NZ is independently associated with household crowding, particularly among NZ-born people aged <40 years. Reducing household crowding would, therefore, reduce TB incidence. This conclusion is probably even more valid for developing countries, where most of the huge global burden of TB falls and where many people live in conditions of extreme household crowding. While the focus of global TB control is on prompt case detection and effective treatment, housing interventions in the form of crowding reduction also have a role in TB control in NZ and internationally.
What is already known on this subject
TB is a disease of poverty though the cause for this association is not fully understood.
TB incidence in developed countries is driven by immigration, local transmission and reactivation of old infections.
What this study adds
Household crowding makes an independent contribution to TB transmission within a developed country (New Zealand).
There is little evidence of TB transmission from migrants to the local-born population.
Policy implications
TB control programmes should include strategies to reduce household crowding particularly for populations with high rates of TB and high levels of household crowding.
Acknowledgments
This work was carried out in the He Kainga Oranga (Housing and Health Research Programme) at the Department of Public Health, Wellington School of Medicine and Health Sciences. Parts of this work are based on data provided by the Institute of Environmental Science & Research Limited (on behalf of the Ministry of Health) and Statistics New Zealand. However, the analyses, conclusions, opinions and statements expressed herein are those of the authors, and not necessarily those of the Institute of Environmental Science & Research Limited, the Ministry of Health or Statistics New Zealand. The authors thank Associate Professor Richard Edwards (Department of Public Health, Wellington School of Medicine and Health Sciences) and Dr Colleen Kelly (School of Mathematics Statistics and Computer Science, Victoria University), for helpful comments on the manuscript.
REFERENCES
Supplementary materials
web only appendix 62/8/715
Files in this Data Supplement:
Footnotes
▸ Additional appendices are published online only at http://jech.bmj.com/content/vol62/issue8
Funding: This study was funded by the Health Research Council of New Zealand. Dilip Das was partly supported by endowment from New Zealand Population Health Charitable Trust.
Competing interests: None declared.
Linked Articles
- In this issue