Article Text

Abstract
Background: Sleep-disordered breathing (SDB) is common after stroke, but it is unclear whether it should be treated.
Objective: To conduct a randomised controlled trial of continuous positive airway pressure (CPAP) after stroke.
Methods: Patients with stroke with ⩾30 apnoeas and hypopnoeas per hour ((A+H)/h) with predominant obstructive sleep apnoea or hypopnoea were randomised to either CPAP treatment or conservative treatment for 8 weeks. Outcomes were measured blind to treatment allocation at 8 weeks and 6 months after the stroke. The primary outcome was physical function on the Nottingham Extended Activities of Daily Living Scale.
Results: Of 658 patients with stroke screened, only 71 (10.7%) were eligible and consented to a sleep study 14–19 days after stroke. 66 patients completed the sleep study (21 women; mean age 72 years), 33 (50%) had ⩾30 (A+H)/h that were predominantly obstructive. 15 were randomised to CPAP treatment and 15 to conventional treatment. Despite intensive efforts, objective use of CPAP was poor, averaging 1.4 h a night. CPAP treatment resulted in no significant improvements (p>0.1) in the primary outcome or in neurological function or sleepiness, and in poorer health status on some measures.
Conclusions: This trial showed no benefit from CPAP treatment, the relevance of the observed detrimental effects is questionable. Even in our highly selected patients with stroke, use of CPAP was poor. At present, CPAP treatment should be advocated for patients with stroke only if they have symptoms of SDB.
- ACE, Addenbrooke’s Cognitive Examination
- CPAP, continuous positive airway pressure
- EADL, Extended Activities of Daily Living
- HADS, Hospital Anxiety and Depression Scale
- IQR, interquartile range
- RCT, randomised controlled trial
- SDB, sleep-disordered breathing
Statistics from Altmetric.com
- ACE, Addenbrooke’s Cognitive Examination
- CPAP, continuous positive airway pressure
- EADL, Extended Activities of Daily Living
- HADS, Hospital Anxiety and Depression Scale
- IQR, interquartile range
- RCT, randomised controlled trial
- SDB, sleep-disordered breathing
In the past decade, a link between stroke and sleep-disordered breathing (SDB) has been recognised. Longitudinal studies have shown that people with SDB have a greater risk of stroke,1 although this relationship is partly explained by the association between SDB, obesity and hypertension. SDB is also common after stroke2–5 and has been associated with poor outcomes.6,7,8,9,10 Continuous positive airway pressure (CPAP) treatment improves daytime function,11 blood pressure12 and cerebral blood flow13 in stroke-free people with SDB and may reduce their risk of cardiovascular event.14 The question then arises whether CPAP treatment in patients with stroke with SDB might improve outcomes. Martinez-Garcia et al15 showed that patients with SDB after stroke who complied with CPAP use had fewer vascular events during follow-up than those who did not. To reliably determine whether CPAP use improves outcome, however, we need to conduct randomised controlled trials (RCTs). There have been few trials of CPAP use for SDB in patients with stroke, and only one entailed random allocation to CPAP use or control.16
We conducted an RCT in patients with stroke with SDB to examine whether CPAP use is beneficial. Specifically, we hypothesised that nasal CPAP use might improve sleepiness, fatigue, cognitive function and mood in patients with stroke with SDB, we also postulated that nasal CPAP might make this group more compliant with rehabilitation and stabilise circadian blood pressure in the recovery phase of stroke; thus CPAP use would result in better functional outcome.
PATIENTS AND METHODS
Recruitment
We approached consecutive patients with stroke admitted to two acute stroke units in the university hospitals in Edinburgh, UK from March 2001 until May 2003. The diagnosis of stroke was confirmed by neurological assessment and computed tomography scans or magnetic resonance images. Ischaemic strokes were classified according to the Oxford Community Stroke Project.17 Patients were asked to consent to an initial screening for SDB and, if this was positive, to be enrolled into an RCT on CPAP use. The local ethics committee approved the study.
Inclusion criteria were as follows: age 21–90 years; stroke 14–19 days previously; pre-stroke Modified Rankin Score ⩽2; National Institutes of Health Stroke Score ⩾4.18 We selected patients at 14–19 days after stroke so that they were likely to be clinically stable and had had a longer time to adjust to the stroke, and so greater potential to use nasal CPAP.
Exclusion criteria were as follows: severe or unstable medical conditions including dementia; severe dysphasia or confusion that would inhibit the patient cooperating with the diagnostic study or CPAP treatment; unusual stroke (eg, venous infarction, vasculitis, brain tumour, myocardial infarction); insufficient hand function to use a mask and no overnight care giver to help.
Baseline assessment and sleep study
Demographic information was collected from case notes. Between days 14 and 19 after stroke, recruited patients had a limited sleep study using a validated19 system (Embletta Portable Diagnostic System, Medcare Flaga, Iceland) incorporating nasal pressure, oral thermistor, thoracoabdominal movement, finger pulse oximetry and body position.
The portable device was programmed to record from 21:00 to 06:00. Data were downloaded on to a computer and scored manually. As the Embletta Portable Diagnostic System does not record sleep, the onset of sleep was taken as the onset of rhythmic stable breathing. The end of the study was taken as the patient’s or care giver’s report of final awakening time or continuous movement artefacts without coming back to regularity of breathing pattern. Apnoeas and hypopnoeas were scored using standard criteria,20 and the total number of apnoeas and hypopnoeas per hour in bed after sleep onset was reported as (A+H)/h.
Baseline assessments were carried out the morning after the sleep study. They included Stanford Sleepiness Scale, a 7-point Likert scale21 assessing current sleepiness after stroke, Epworth Sleepiness Scale assessing pre-stroke sleepiness if patients were clear and cooperative enough to fill in the questions, Barthel Index22 indicating their functional independence in everyday activities, Hospital Anxiety and Depression Scale (HADS)23 measuring psychological distress, and Addenbrooke’s Cognitive Examination (ACE)24 assessing cognition and allowing derivation of the Mini-Mental State Examination.25
Randomised trial of nasal CPAP use
Between days 21 and 25 after stroke, patients who had (A+H)/h ⩾30 with <30% of events due to central apnoeas or Cheyne–Stokes respiration were enrolled into our RCT. The cut-off point ⩾30/h was set to recruit a group of patients with stroke who had severe SDB.20 Patients were randomly allocated to receive either 8 weeks of CPAP treatment with Autoset T (ResMed, SanDiego, California, USA) or conservative treatment for SDB. Intensive input by a senior sleep research nurse who was experienced in CPAP treatment was arranged on day 1, day 3, day 5, week 1, week 2, week 4 and week 6 of treatment to optimise compliance. The nurse managed all problems related to mask, machine and complications of CPAP. The treatment period lasted 8 weeks, unless the patient asked for CPAP to be withdrawn. Hours of CPAP usage were downloaded from the machine. Both groups received advice on weight loss and alcohol avoidance when appropriate and all drugs and rehabilitation programmes were maintained as usual.
C-YH identified patients and MV allocated treatment using sealed opaque envelopes with balanced blocks of six and delivered the treatment. Thus C-YH was blind to the allocated treatment and carried out all outcome assessments.
Outcome measures
The Nottingham Extended Activities of Daily Living (EADL)26 Index was chosen as the primary outcome measure for assessing functional capacity in four domains in terms of mobility, kitchen, domestic activity and leisure activity. It is sensitive to change and does not have a ceiling or floor effect, and so is suitable for use in mild to moderate stroke.
Secondary outcome measures included subscales of EADL, National Institutes of Health Stroke Score, Barthel Index, Stanford Sleepiness Scale, ACE and Mini-Mental State Examination, HADS (anxiety and depression subscales), MOS Short Form 36 Health Survey and subscales, and ambulatory blood pressure27—measured using Spacelabs 90207 (Spacelabs, Redmond, Washington, DC, USA). The blood pressure monitor was programmed to measure every 30 min for 24 h, starting between 14:00 and 15:00. We defined pressures between 06:00 and 21:59 as occurring during daytime and those between 22:00 and 05:59 as occurring during night, corresponding to the schedule of the stroke wards.
Follow-up
C-YH, a neurologist, conducted two face-to-face interviews. To ensure blinding to treatment allocation, MV informed the patient, care giver or nursing staff to hide any CPAP machine when C-YH visited the patient. All outcomes were recorded in the 8th week after randomisation. The EADL, Barthel Index and Short Form 36 Health Survey were measured at 6 months after stroke in both groups.
Sample size
Before the study, we estimated that 40 patients using CPAP (CPAP group) and 40 controls (undergoing conventional treatment) were needed for 80% power at 5% significance level to show 0.57 point standardised mean difference in the EADL. This was on the basis of outcome data from an RCT of outpatient occupational therapy for stroke.28
Statistical analyses
These were based on intention to treat. All continuous data with normal distribution are presented as mean (standard deviation (SD)) and those without normal distribution as median (interquartile range (IQR)). Non-parametric tests were used, including Mann–Whitney’s U test and χ2 test (Fisher’s test if <20 patients in a category) for between-group comparisons; p<0.05 was considered significant.
Multiple linear regression and logistic regression were used to adjust for baseline imbalance. All predictors with p<0.1 in univariate regression analysis were entered into the model, and coefficient and confidence interval (CI) were expressed. Data were statistically analysed by SPSS V.11.0.
RESULTS
Recruitment and demographic characteristics
We screened 658 patients with suspected stroke between March 2001 and June 2003. Only 96 of 658 patients were eligible (fig 1). Of the 66 patients who completed their sleep study, 45 (68%) were men, mean age 72 years, and their pre-stroke Modified Rankin Scores were 0 in 56, 1 in 7 and 2 in 3 patients. Their median National Institutes of Health Stroke Scale at 3 weeks after stroke was 6 (IQR 2–10). Of the 66 patients, 60 had first-ever strokes. According to the Oxford Community Stroke Project classification, 13 patients had total anterior circulation infarct, 41 had partial anterior circulation infarct, three had posterior circulation infarct, four had lacunar infarct and the remaining five had primary intracerebral haemorrhage. The baseline data of 25 patients who declined to give informed consent and five patients who had inadequate sleep studies were not significantly different from those of recruited patients (p>0.7).

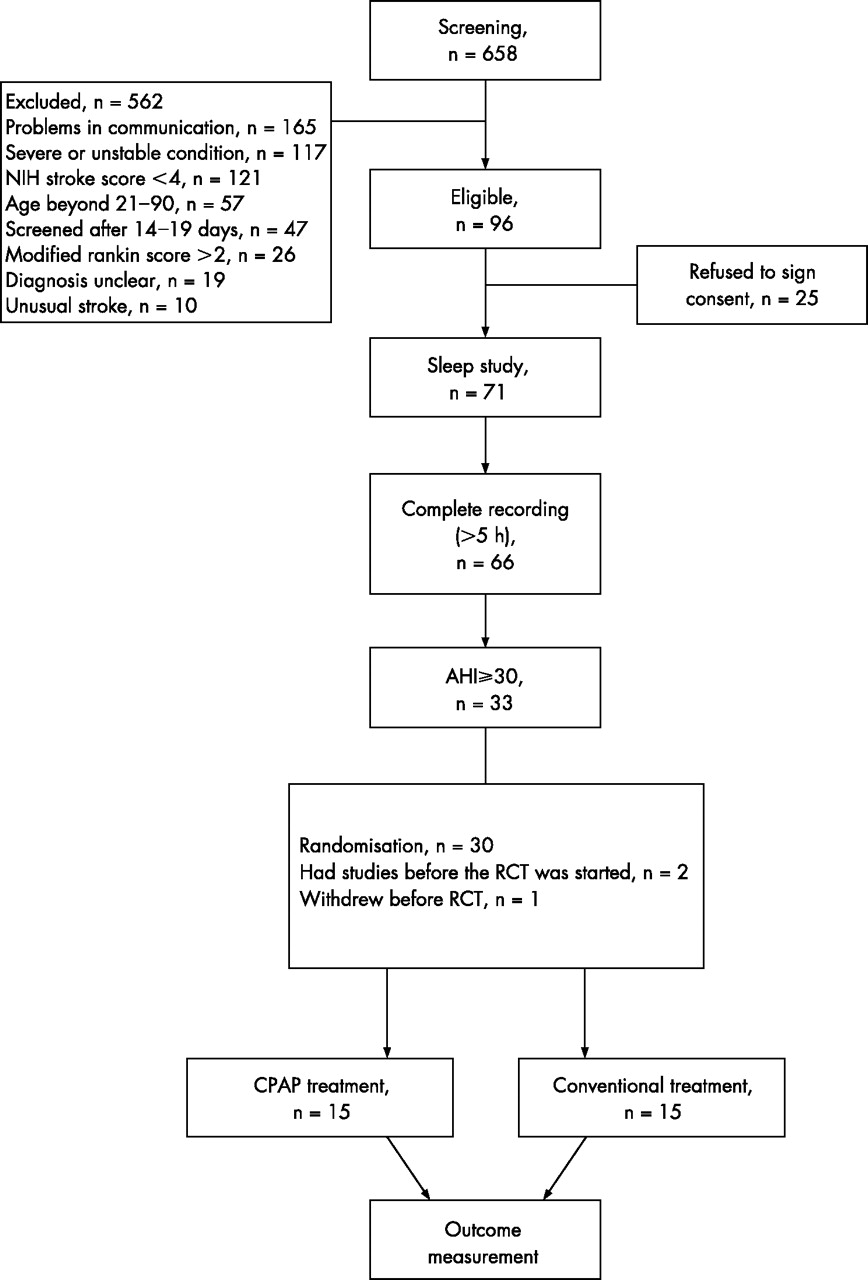{kind=link}
Flow chart of patient recruitment and randomisation. AHI, apnoeas and hypopnoeas per hour; CPAP, continuous positive airway pressure; NIH, National Institutes of Health; RCT, randomised controlled trial.
Results of sleep studies
The sleep study analysis had high intrarater (intraclass correlation coefficient 0.983, p<0.001) and inter-rater reliability (intraclass correlation coefficient 0.977, p<0.001). (A+H)/h was ⩾30 in 33 patients, ⩾20 in 40, ⩾15 in 46 and ⩾10 in 56 patients. The median (A+H)/h was 31. All patients with SDB had predominantly obstructive sleep apnoea and hypopnoea. The median central apnoea index was 0.4 (IQR 0.0–1.1). Nine patients had a few episodes of Cheyne–Stoke respiration, but none fulfilled the criteria for central sleep apnoea.3
Of the 33 patients with (A+H)/h ⩾30, 2 had sleep studies before the RCT of CPAP use was started and another dropped out before randomisation. Thus 30 patients were randomised—15 to CPAP treatment and 15 to conservative treatment for SDB. In the CPAP group, 14 patients had first-ever strokes. 4 had total anterior circulation infarct, 9 had partial anterior circulation infarct, 2 had posterior circulation infarct and 0 had intracerebral haemorrhage and lacunar infarct. In the conventional group, 14 patients had first-ever strokes. Four had total anterior circulation infarct, 7 had partial anterior circulation infarct, 2 had lacunar infarct, one had posterior circulation infarct and one had intracerebral haemorrhage. The trial was terminated before we had recruited our target of 80 patients because recruitment was much more difficult than expected and funding ended.
Baseline data
Patients randomised to CPAP use were similar to those allocated conservative treatment for SDB (table 1). The median Stanford Sleepiness Score was 3 (IQR 1–4) and median pre-stroke Epworth Sleepiness Score was 6 (IQR 3–11).
Baseline data in the continuous positive airway pressure treatment group (n = 15) and controls (n = 15)
Outcome assessment
The primary outcome measurement occurred at 80 (5) days after stroke in the CPAP group and at 79 (4) days in the controls. Two patients died before this assessment, one from each group; their Barthel Index and EADL at follow-up were scored as 0 and other scales were not scored. One patient from the controls agreed only to telephone interview so results of the National Institutes of Health Stroke Score, ACE and Mini-Mental State Examination, which need face-to-face assessment, were not available.
We found no significant differences in outcome with respect to any of the primary or secondary measures at the 3-month follow-up (p>0.1, table 2).
Outcome measurement in the continuous positive airway pressure treatment group and controls at 3 months (post-treatment phase)
Retrospective exploratory analyses showed that patients randomised to CPAP use had significantly lower scores on the mobility subscale of EADL (p = 0.048). However, they also tended to have lower Barthel Index at baseline. Having adjusted for baseline imbalance by multivariate analysis, this difference in the mobility subscale was not significant (p = 0.077). The CPAP group also had significantly lower scores in the physical summary score of the Short Form 36 Health Survey (p = 0.022). This difference remained even after adjusting for baseline imbalance (p = 0.008). At 6 months after stroke, there was no difference between the CPAP group and the controls (table 3).
Outcome measurements at 6 months after stroke in the continuous positive airway pressure treatment group and controls
Ambulatory blood pressure monitoring
We found no significant difference in 24-h, daytime and night-time systolic blood pressure, diastolic blood pressure and mean arterial pressure between the CPAP group and controls. Systolic blood pressure over 24 h was 126.2 (21.5) and 130.0 (18.4) mm Hg and diastolic blood pressure was 71.6 (6.7) and 73.7 (12.3) mm Hg in the CPAP group and controls, respectively (table 4; p>0.4).
Comparison of ambulatory blood pressure monitoring between the continuous positive airway pressure treatment group and controls
Compliance with nasal CPAP use
Despite intensive education and encouragement, only 7 of 15 patients who were randomised to CPAP use kept the machine for more than 4 weeks. The duration of CPAP treatment was negatively correlated with the depression subscale score of HADS (p = 0.039) and positively correlated with the language subscale score of the ACE (p = 0.036) at baseline—that is, better cognition and less depression were associated with using the CPAP machine longer.
Among the 15 patients randomised to CPAP use, two patients rejected CPAP after mask fitting and a brief trial in the afternoon on day 1 of the treatment phase, one patient rejected CPAP after the first night of CPAP use, one died of adult respiratory distress syndrome on day 4 of the CPAP limbs, and one rejected CPAP after 1 week of CPAP use.
Mean CPAP use in 15 patients was 1.4 h/night (median 0.16 h/night) when averaged over the 8-week treatment period. Mean CPAP usage exceeded 6 h a night in only two patients. The baseline data of five patients with better compliance (⩾1 h, mean 3.8 (SD 2.8, range 1.0–7.3) h/night) had mean (SD, range) (A+H)/h 46 (10, 36–58), body mass index 29.3 (5.9, 21.8–38.1) kg/m2, Epworth Sleepiness Scale 6 (4, 3–14), Stanford Sleepiness Scale 2 (1, 1–3), National Institute of Health Stroke Score 6 (4, 4–13) and Barthel Index 15 (6, 4–19). These were not significantly different from other patients who were randomised (p>0.05).
Problems with CPAP use in the 15 patients were categorised into the following four groups.
-
Problems with the machine: Eight patients had problems with either mask or machine. Four of them abandoned CPAP use quickly, including two who had claustrophobia.
-
Complications of CPAP use: Eight patients developed upper airway symptoms after treatment and three of them withdrew due to these symptoms.
-
Complications of stroke: Nine patients had stroke-related problems that caused non-compliance, including facial palsy, nocturnal confusion and involuntary movement of head or wounds on the face due to falling down.
-
Lack of belief in treatment: Two patients did not think that they needed CPAP on a nightly basis.
CPAP use was positively correlated with a better Barthel Index (p = 0.035) and language subscale of ACE (p = 0.013), but negatively correlated with depression subscale in HADS (p = 0.032) at baseline. The median depression subscale of the HADS in the five patients with better use (5, IQR 3–5) was lower than in patients with poor use (7, IQR 3–10.5, p = 0.031).
DISCUSSION
Our sleep studies confirm that SDB is common after acute stroke and that most of the sleep-related breathing events are obstructive.4,5 However, we were unable to show any beneficial effect of CPAP treatment in patients in the subacute phase of stroke.
We cannot exclude a clinically relevant benefit of CPAP use in patients with stroke because we recruited fewer patients than planned and thus our trial had insufficient power to show anything other than large effects. Our failure to show any effect of CPAP, either positive or negative, may also be due to the poor use of CPAP in this trial.
CPAP use was poor despite our expertise in this area,29,30 our exclusion of many patients in whom we thought CPAP use would be difficult, our use of auto-titrating CPAP which may improve CPAP use in SDB,31 and the intensive input from an experienced specialist sleep nurse (MV). Many of the patients were inpatients during the treatment phase. Of the patients treated using CPAP, there were only two patients who on most criteria would have been regarded as having adequately used CPAP; of the five with “better use”, the other three used the treatment for only ⩽2 h/day on average. The two good compliers in CPAP group were relatively younger (ages 65 and 73 years) and had less severe stroke (Barthel Index 19 and 18 v 11). One had previously habitual snoring, witnessed apnoea and unrefreshed sleep. Another had previously unrefreshed sleep and mild excessive daytime sleepiness (postprandial). Both of them might have pre-existing obstructive sleep apnoea but their (A+H)/h was not higher than that of the rest of the CPAP group (35.9 and 35.6 v 43.1) and their Epworth Sleepiness Scale was normal (4 and 5). Compliance might be improved in future studies by focusing on less depressed and cognitively less impaired patients, but this would further reduce the generalisability of any result. Focusing on sleepy patients would also be interesting.
Compliance with CPAP after stroke has varied considerably in previous studies.16,32–34 This variation is likely to reflect differences in patient selection, environment in which treatment is given, the CPAP system used and the amount and type of support and training given.
Our study cannot support the recent studies,1,14,15 which suggested that treatment for SDB reduces the risk of vascular events. However, we studied unselected patients with stroke, whereas all these studies were on populations with pre-existing sleep apnoea.1,14,15 The only other RCT of CPAP use after stroke included 59 patients randomised between 7 and 28 days after stroke to either CPAP treatment for 4 weeks or conventional treatment.16 Outcomes were assessed at 7 and 28 nights, respectively. CPAP use had no effect on recovery from stroke, but there were fewer depressive symptoms among those treated with CPAP. Of the 31 patients, 16 (51.6%) used CPAP for >4 h/night, with a mean of 4.1 (SD 3.6, range 0–10.9). We found no improvement in depressive symptoms nor was there any such trend in our data. Similarly, we did not show any reduction in ambulatory blood pressure with CPAP use, which was reported in one non-RCT on 16 patients in which non-compliant patients were used as controls.34
We found that the CPAP group had considerably lower physical summary scores on Short Form 36 Health Survey after treatment even after adjusting for baseline Barthel Index. This may be due to chance given our multiple testing, but we cannot exclude the possibility that CPAP treatment might have a negative effect on certain aspects of outcome.
Although the severity of upper airway obstruction is associated with a worse functional outcome at 6 months after stroke,10 at present we believe that CPAP should be used only after stroke in those patients who satisfy the criteria for the sleep apnoea–hypopnoea syndrome20 but have no clinically noticeable dysphasia or depression. If improvements in equipment or techniques that could increase CPAP compliance in patients with stroke become available, then further randomised studies of the potential benefits of CPAP would be worthwhile.
REFERENCES
Footnotes
-
Published Online First 19 June 2006
-
Funding: This study was funded by Chest, Heart and Stroke Scotland (RO1/A54).
-
Competing interests: NJD is a medical adviser to ResMed Ltd, a company manufacturing CPAP machines.
-
Ethics approval: Ethics approval was obtained from the Lothian Research Ethics Committee (reference MREC/2000/4/44). Trust management approval was given by the Research & Developmental Office on behalf of the Trust Chief Executive and Medical Director (Reference R&D/99/17/08). All participants gave written informed consent.