





Abstract
Asthma is a heterogeneous airway disease with various clinical phenotypes. It is crucial to clearly identify clinical phenotypes to achieve better asthma management.
We used cluster analysis to classify the clinical groups of 724 asthmatic patients from the Cohort for Reality and Evolution of Adult Asthma in Korea (COREA), and in 1843 subjects from another independent Korean asthma cohort of Soonchunhyang University Asthma Genome Research Centre (SCH) (Bucheon, Republic of Korea). Hierarchical cluster analysis was performed by Ward's method, followed by κ-means cluster analysis.
Cluster analysis of the COREA cohort indicated four asthma subtypes: 1) smoking asthma; 2) severe obstructive asthma; 3) early-onset atopic asthma; and 4) late-onset mild asthma. An independent cluster analysis of the SCH cohort also indicated four clusters that were similar to the COREA clusters.
Our results indicate that adult Korean asthma patients can be classified into four distinct clusters.
Asthma is a heterogeneous airway disease with various clinical phenotypes of differing severity [1]. Recent studies have identified different asthma subtypes based on clinical features and pathophysiological mechanisms [2–6]. Given the heterogeneous nature of asthma, it is crucial to clearly define certain subtypes of asthma with homogeneous clinical characteristics in order to search for better asthma management and to develop novel therapeutic strategies. Clinically well-defined asthma phenotypes will be a solid foundation not only for elucidating the precise pathogenesis of asthma but also for developing new drugs.
Despite the urgent need for an improved classification of asthma subtypes, methods needed to classify subtypes of asthma have not yet been clearly established. Cluster analysis is one method that can be used to classify asthma subtypes, although some limitations exist with this method. Cluster analysis uses a set of observations to create subsets, in which members of the same subset are similar to one another in some critical characteristics and different from other subsets in the same critical characteristics.
Several previous studies have defined clinical phenotypes of asthma by use of cluster analysis. Haldar et al. [7] identified three distinct clinical phenotypes in asthmatics from primary care clinics, four phenotypes of refractory asthma patients and two phenotypes that were common in both asthma populations. Subsequently, the US National Heart, Lung and Blood Institute (sponsors of the Severe Asthma Research Program (SARP)) characterised five distinct clinical phenotypes of asthma based on cluster analysis of 726 asthma subjects [4]. Moreover, they suggested a functional “tree analysis” using three common variables, such as baseline forced expiratory volume in 1 s (FEV1), maximal FEV1 after albuterol and age at asthma onset [4]. Another population-based study of 175 subjects with obstructive airway patterns, including asthma and chronic obstructive pulmonary disease, identified five distinct clinical phenotypes of airflow obstruction by use of cluster analysis [8].
Asthma is a multifactorial disorder with clinical features that are affected by genetic and environmental factors. Thus, the clinical phenotypes of asthmatic patients from Korea may differ from those of other populations. To date, the clinical characteristics of different subtypes of asthmatic patients in Korea have not been reported. In the present study, we used cluster analysis to identify the clinical groups of asthma in two large independent cohorts of Korean adult asthma patients. The aim of this study was to identify novel phenotypes of Korean asthma patients that may finally lead to better understanding of asthma heterogeneity and provide a worthy foundation for further elucidation of the pathogenetic mechanisms of each phenotype of asthma.
METHODS
Study populations
The first cohort, patients from the Cohort for Reality and Evolution of Adult Asthma in Korea (COREA), were recruited by allergists or pulmonologists from 11 referral centres in diverse areas of the Republic of Korea [1]. These patients had dyspnoea, cough, sputum production or wheezing for >3 months. All subjects had significant airway hyperresponsiveness (AHR), as indicated by provocative concentration causing a 20% fall in FEV1 (PC20) <16 mg·mL−1 in a methacholine bronchial provocation test or positive bronchodilator responsiveness (>12% improvement in FEV1 after administration of 180 μg of albuterol by a metered-dose inhaler). At enrolment, the patients were in stable state with regular medications. Subjects with destroyed lungs, bronchiectasis or lung resection were excluded [1].
Another independent cohort of patients (Soonchunhyang University Asthma Genome Research Centre (SCH), Bucheon, Republic of Korea), were adult asthma patients registered at the Korea Genome Research Centre for Allergy and Respiratory Diseases (Bucheon, Republic of Korea). Asthma diagnosis was based on the Global Initiative for Asthma (GINA) guidelines, as described previously [9]. All patients were ethnic Koreans aged >18 years and were regularly followed and treated with appropriate medications based on the 2002 GINA guidelines [9]. Like the COREA cohort, the patients were in stable state with regular medications at enrolment.
The design and protocol for this cohort study were approved by the institutional review board of each centre.
Assessments and measurements
Demographic parameters, body mass index (BMI), complete blood cell count and total serum IgE levels were recorded. Pulmonary function tests were used to determine FEV1, forced vital capacity (FVC) and the FEV1/FVC ratio [10]. AHR was measured using the methacholine bronchial provocation test [11] and skin prick tests with 12 common allergens (Allergopharma, Reinbek, Germany) were used to detect atopy [12]. Smoking status and history of hospital visits due to asthma exacerbation during the previous year were recorded. All data were collected when patients were medically stable.
Statistical analysis
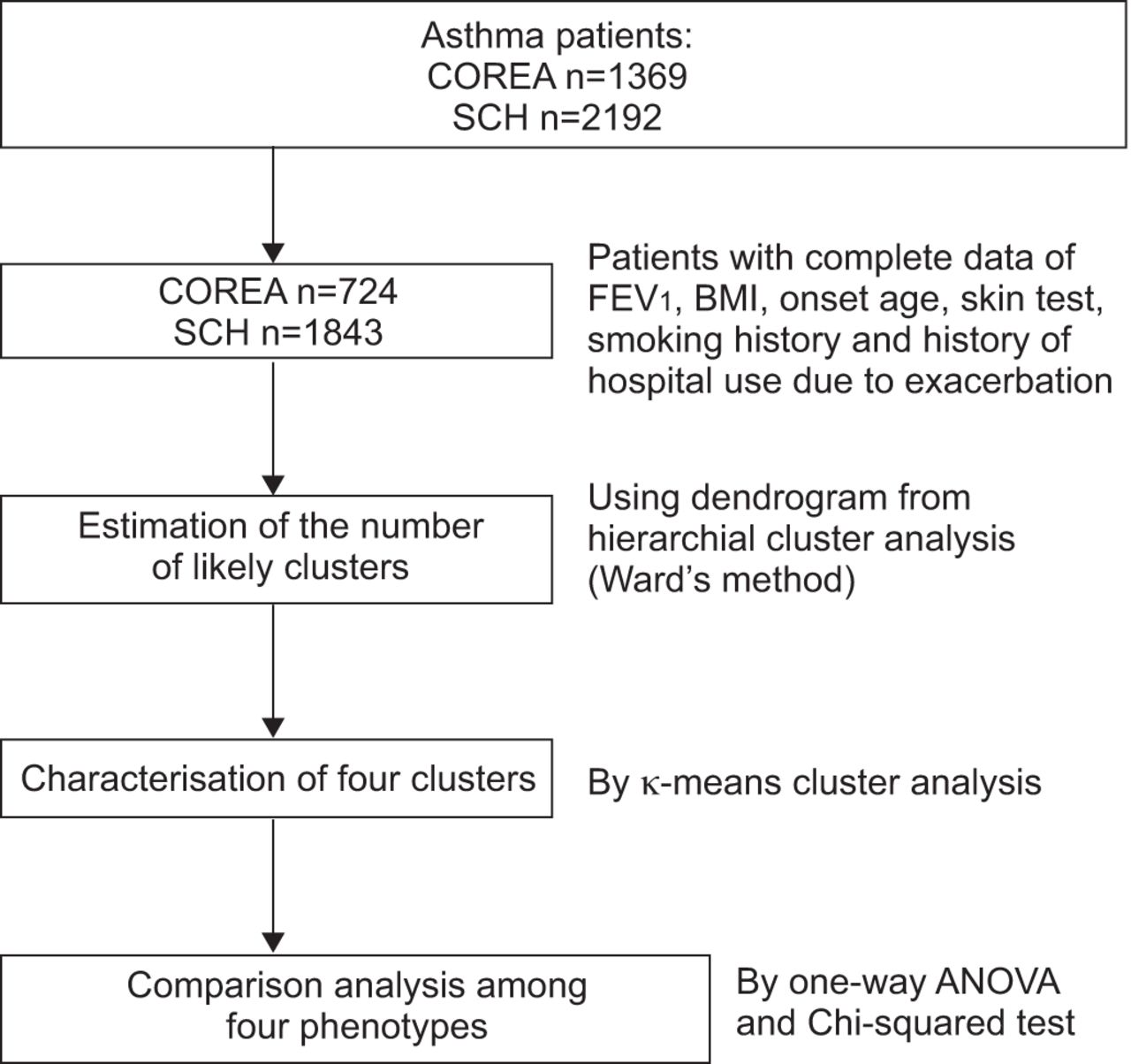
Uniform cluster analysis methodology with a two-step approach was used to classify patients from COREA and the SCH cohort. In brief, hierarchical cluster analysis using Ward's method followed by κ-means cluster analysis was performed. In the first step, hierarchical cluster analysis using Ward's method generated a dendrogram for estimation of the number of likely clusters within each population. This estimate was pre-specified in a κ-means cluster analysis that was used as the principal clustering technique [7]. Variables for cluster modelling were selected based on their contribution to characterisation of the asthma phenotype. All measurements were standardised using z-scores for continuous variables and as 0 or 1 for categorical variables. Six variables, including FEV1, BMI, age at onset, atopic status, smoking history and history of hospital use due to exacerbation, were used to characterise the asthma clusters for the COREA and SCH cohorts.
The initial dataset included 1369 subjects in the COREA cohort and 2192 in the SCH cohort. Both cohorts did not completely exclude smoking asthma patients if their asthma was soundly confirmed when the asthma patients were enrolled. Thus, to select pure asthma patients among the cohort, only the patients who had completely normal chest radiography and whose data included no missing values in essential variables such as FEV1, BMI, age at onset, skin test, smoking history and history of hospital use due to exacerbation were selected for cluster analysis. The final analysis was performed with 724 subjects from the COREA cohort and 1843 subjects from the SCH cohort (fig. 1 and table 1). We compared the main clinical characteristics of excluded subjects with included subjects (online supplementary tables S1 and S2). Our data showed that there were no differences among most variables between two groups, except one or two variables. In the COREA cohort there was a difference in age at onset and minimal difference in smoking history. In the SCH cohort, only smoking history showed difference.

Summary of statistical methods. COREA: Cohort for Reality and Evolution of Adult Asthma in Korea; SCH: Soonchunhyang University Asthma Genome Research Centre; FEV1: forced expiratory volume in 1 s; BMI: body mass index.
A between-cluster comparison was performed using ANOVA or a Chi-squared test using the SPSS statistical package (version 12.0; SPSS Inc., Chicago, IL, USA). A p-value <0.05 was considered statistically significant.
RESULTS
Cluster analysis of the COREA cohort
We used Ward's method to obtain dendrograms that estimate the number of likely clusters, and then used κ-means analysis to determine that a four-cluster model best fit the COREA cohort (fig. 2 and table 2).

Four clusters in the Cohort for Reality and Evolution of Adult Asthma in Korea (COREA). They indicated four asthma subtypes: smoking asthma (A), severe obstructive asthma (B), early-onset atopic asthma (C) and late-onset mild asthma (D). Sphere size represents the size of the population distributed to each cluster.
Cluster A (81 subjects) was the smallest group and mainly consisted of male patients (97%) with a mean onset age of 46 years. Approximately 34% had positive skin prick tests and 22% had a history of healthcare usage due to asthma exacerbation. They had relatively well-preserved FEV1 of 82.47±16.45% predicted. This cluster had the greatest number of smoking pack-years, 34.4±14.1 pack-years, thus we named it the “smoking asthma” group.
Cluster B (151 subjects) was the second-smallest cluster and about half of the subjects had atopy. The mean age at onset was 39 years and 46% of the subjects used healthcare services because of asthma exacerbations. The mean FEV1 was the lowest of all clusters, 56.5±13.7% pred, and the increase in FEV1 after bronchodilator use was the greatest of all clusters, at 12.0±12.1% pred. Based on the methacholine provocation test, the PC20 was the lowest of all clusters (3.1±5.4 mmol·L−1). This group had a lower rate of smoking than cluster A (3.2±6.5 pack-years). We named this cluster the “severe and obstructive asthma” group.
Cluster C (253 subjects) was the largest cluster. This group had the youngest mean age at onset, 21 years, and about two-thirds of the patients had atopy. The FEV1 was 88.6±11.2% pred and the rate of smoking was 2.0±3.7 pack-years, the lowest of all clusters. We named this cluster the “early-onset atopic asthma” group.
Cluster D (239 subjects) had the highest FEV1 of all clusters, 97.9±11.5% pred and the mean age at onset was 48 years, the oldest of all the clusters. Other clinical characteristics, such as the prevalence of rhinitis and eosinophil counts in blood samples, were not significantly different from the other clusters. We named this cluster the “late-onset mild asthma” group.
Because FEV1 is a highly variable factor, we analysed longitudinally the variability of FEV1 % pred over 12 months after the time of the first cluster analysis using the linear mixed-effect model. The consistent differences between the four clusters throughout the 12-month follow-up period was statistically significant (p<0.001), showing the stability of the four groups created by the cluster analysis despite of asthma treatment (fig. 3).

{kind=link}
{kind=link}
{kind=link}
Longitudinal assessment of forced expiratory volume in 1 s (FEV1) over 12 months according to each cluster in the Cohort for Reality and Evolution of Adult Asthma in Korea (COREA). Cluster A: smoking asthma; cluster B: severe obstructive asthma; cluster C: early-onset atopic asthma; cluster D: late-onset mild asthma. The consistent differences between the four clusters throughout the 12-month follow-up period was statistically significant (p<0.001) when the linear mixed-effect model was used.
Cluster analysis of the SCH cohort
We used the same methodology to classify the SCH cohort to determine whether the results of the COREA cohort could be replicated. This analysis also led to the identification of four clusters, each with characteristics similar to those of the COREA cohort (table 3).
Cluster A′ was the smallest group (217 subjects), was predominantly male (88%), had the greatest mean age at onset (52 years) and the highest rate of cigarette smoking (37.2±16.0 pack-years). The mean FEV1 was slightly lower than the COREA Cluster A, but was also well-preserved, as in the COREA Cluster A.
Cluster B′ consisted of 479 subjects, most of whom had atopy. The mean age at onset was 42 years and the FEV1 was the lowest of all clusters (54.3±13.3% pred), similar to Cluster B in the COREA cohort. This cluster also had a low rate of cigarette smoking (4.52±7.23 pack-years).
Cluster C′ consisted of 585 subjects, and was the largest cluster. Consistent with our analysis of the COREA cohort, the mean age at onset was 21 years, the lowest of all clusters, and the rate of atopy was the highest of all clusters (74.2%). The mean FEV1 value was relatively well preserved (88.56±12.71% pred) and the smoking rate was also the lowest of all clusters (2.7±6.0 pack-years).
Cluster D′ comprised 562 subjects. This group had the greatest FEV1 (97.70±13.92% pred) and the mean age at onset was 50 years. This cluster closely resembled Cluster D from the COREA cohort (table 3).
DISCUSSION
In the current study, we used cluster analysis to identify four distinct clinical groups of asthma in two independent cohorts of Korean adult asthma patients. We assigned the following names to these four clusters based on their distinguishing characteristics: smoking asthma, severe obstructive asthma, early-onset atopic asthma and late-onset mild asthma. Although we have not determined the clinical implications of our classification, it seems likely that each cluster has a different underlying pathophysiology and clinical course, and that different therapeutic approaches should be used for the different clusters.
Many previous studies have also classified asthma subtypes. However, many of these studies used methods that are susceptible to bias due to historical factors or preconceived ideas for classification of asthma [2, 13–15]. The clinical features of asthma are heterogeneous, so there is a need for a reliable classification system that incorporates multiple clinical features and provides accurate and easily identified subtypes. Recently, researchers from the UK [7] and USA [4] conducted cluster analyses of asthma patients, an objective method with no preconceived hypothesis. In the UK study, Haldar et al. [7] classified asthma phenotypes from primary care clinics as: early onset, atopic asthma, obese, noneosinophilic asthma and benign asthma. They also classified refractory asthma patients as early symptom-predominant asthma and inflammation-predominant asthma [7]. An analysis of the SARP cohort in the USA [4] identified five distinct asthma clusters, ranging from mild to severe asthma: mild atopic asthma, mild-to-moderate atopic asthma, late-onset nonatopic asthma, severe atopic asthma and severe asthma with fixed airflow.
Asthma is a multifactorial disease in which genetic factors, environmental factors and social background affect the clinical features [13, 16]. To the best of our knowledge, the present study is the first to classify Asian asthma patients by cluster analysis. In contrast to the studies from the UK [7] and USA [4], we identified four distinct phenotypes of asthma among Korean asthma patients. Cluster B/B′ in our study was more likely to include patients with severe asthma, in terms of airway obstruction in particular. The cluster analysis performed in SARP [4] also indicated a cluster with severe obstruction and very poor lung function, similar to our cluster B/B′. These results suggest that our cluster B/B′ may be closely associated with severe refractory asthma, a disease subtype that has attracted significant research into new therapies. The clinical implications of cluster B/B′, however, are not yet clear and future long-term studies are needed to better characterise this cluster.
Our cluster C/C′ appears to be very similar to the “early onset, atopic asthma” group in the UK study and “cluster 1 and 2” in the USA study, in terms of clinical features (early age at onset, high prevalence of atopy and well-preserved FEV1). Our cluster D/D′ also resembles the “benign asthma” group in the UK study (relatively late age at onset, similar rates of atopy and the greatest FEV1 values). These results indicate that the subtypes of asthma appear to be similar for subjects from the USA, UK and Korea.
The present study included asthma patients with a history of cigarette smoking, regardless of the number of pack-years and current smoking status. In contrast, the UK study only enrolled current nonsmokers or ex-smokers who had a history of <10 pack-years [7]. In addition, many previous studies of asthma have only analysed nonsmokers to exclude the effect of smoking and smoking-related airway diseases. Cigarette smoking, however, is considered an important environmental risk factor for the development of asthma, and is known to negatively influence the clinical course of asthma. In particular, smoking is associated with severe asthma, aggravation of asthma symptoms, accelerated decline of lung function [17] and limited responses to corticosteroids [18, 19]. Furthermore, a previous study indicated that more than half of the asthma patients in Korea were current or ex-smokers [1]. Thus, excluding asthmatic patients with a history of substantial smoking would lead to an unrepresentative sample. Interestingly, we identified a cluster that we called “smoking asthma” (cluster A/A′). We suggest further analysis of other ethnic groups to evaluate the clinical significance of this cluster.
One remarkable observation of our study is that BMI was close to normal in Korean refractory asthmatics, in contrast to European and US asthmatics [16, 20, 21]. In addition, the proportion of atopy is lower in Korean asthmatics (<50%) than in European and US patients. These results are consistent with our previous study of an adult asthma cohort in Korea, which showed that BMI was not associated with asthma severity, and that there was no relationship between atopy status and asthma severity [1].
The present study has several limitations. First, cluster analysis may not be a perfectly appropriate method for the objective classification of a heterogeneous disease such as asthma. We think that the clusters identified in this study cannot be immediately applied to clinical practice and further studies are definitely needed to elucidate precise characterisation of each cluster scientifically. Nevertheless, trying hard to identify well-defined phenotypes of asthma is quite worthy, since proper classification of asthma is a crucial and fundamental pre-requisite for not only better management of asthma patients, but also elucidating the precise pathogenic mechanisms underlying the development of each phenotype of asthma, which is largely unclear so far. For example, the potential value of this cluster analysis would be found in the observation of the limitation of the current classification of asthma in genome-wide association studies (GWAS), because imprecise phenotyping is considered to be one of the reasons that GWAS have only revealed small genetic effects of genetic variants. In our study, patients were divided into several clusters based on overall similarity of multiple variables selected by researchers. We selected FEV1, BMI, age at onset, atopic status, smoking history and healthcare use due to exacerbation of asthma for our analysis. All of these can be considered important influences on asthma. These variables were chosen because they were measurable in clinical practice, contribute to clinical evaluation and are important in defining disease subtypes. However, these variables differ among studies. For example, Haldar et al. [7] included variables such as atopy, airway inflammation, peak expiratory flow variability, Juniper Asthma Control Score, sex, age at onset and BMI in their cluster analysis, and 34 variables were included in the SARP cluster analysis of asthma [4]. However, the appropriateness of the variables that we used needs to be verified.
A second limitation of this study is that we did not use patterns of airway inflammatory cells as a key variable for cluster analysis. However, precise data on airway inflammatory cells via induced sputum analysis is not always obtainable in clinical practice, and the results are not always definitive. In fact, sputum samples of quality acceptable for analysis could only be obtained from some of our subjects. Moreover, many of our patients were treated with an inhaled corticosteroid, and this can affect the results of induced sputum analysis. Thus, an attempt to identify phenotypes of asthma without sputum analysis might be rather more clinically feasible. We suggest that further studies examine airway inflammatory patterns as a critical variable to confirm the clinical implications of our study.
Finally, we did not consider quality of life as a variable, in contrast to the study by Haldar et al. [7]. Although we expect that exclusion of this variable would not seriously affect our results, further studies should consider this issue.
In conclusion, the results of this study demonstrate that cluster analysis can be used to identify discrete groups of Korean asthma patients. This cluster analysis has a potential to stratify the heterogeneous groups of asthma into more homogenous ones and significantly advance our understanding of asthma phenotypes. A long-term longitudinal study of each cluster would be able to determine whether the different clusters have different underlying pathophysiology, responses to treatment and prognosis.
Acknowledgments
The COREA Study Group includes the following investigators: Hee-Bom Moon, You Sook Cho and Tae-Bum Kim (University of Ulsan, Seoul, Republic of Korea); Sang-Heon Cho and Heung-Woo Park (Seoul National University, Seoul, Republic of Korea); Yoon-Seok Chang (Bundang Seoul National University, Seoul, Republic of Korea); Jung-Won Park (Yonsei University, Seoul, Republic of Korea); Byoung-Whui Choi (Chung-Ang University, Seoul, Republic of Korea); Young-Joo Cho (Ewha Womans University, Seoul, Republic of Korea); Ho-Joo Yoon and Sang-Heon Kim (Hanyang University, Seoul, Republic of Korea), An-Soo Jang, Sung-Woo Park and Choon-Sik Park (Soonchunhyang Univeristy, Bucheon, Republic of Korea); Dong-Ho Nam (Ajou University, Suwon, Republic of Korea); Soon-Seog Kwon (Catholic University, Seoul, Republic of Korea); and Yong Chul Lee (ChonBuk National University, Jeonju, Republic of Korea). The SHC cohort includes three referral centre hospitals (Soonchunhyang University Bucheon Hospital (Bucheon, Republic of Korea), Seoul Hospital (Seoul, Republic of Korea) and Cheonan Hospital (Cheonan, Republic of Korea)).
Footnotes
This article has supplementary material available from www.erj.ersjournals.com
For editorial comments see page 1247.
Support Statement
This study was supported by grants from the Korea Health 21 R&D Project (grant numbers A090548 and A102065) (Ministry of Health, Welfare and Family Affairs, Seoul, Republic of Korea) to C-S. Park, H-B. Moon and Y.S. Cho.
Statement of Interest
None declared.
- Received June 13, 2011.
- Accepted September 29, 2012.
- ©ERS 2013
REFERENCES










