





Abstract
The United Nations Millennium Development Goal of reversing the global spread of tuberculosis by 2015 has been offset by the rampant re-emergence of drug-resistant tuberculosis, in particular fluoroquinolone-resistant multidrug-resistant and extensively drug-resistant tuberculosis. After decades of quiescence in the development of antituberculosis medications, bedaquiline and delamanid have been conditionally approved for the treatment of drug-resistant tuberculosis, while several other novel compounds (AZD5847, PA-824, SQ109 and sutezolid) have been evaluated in phase II clinical trials. Before novel drugs can find their place in the battle against drug-resistant tuberculosis, linezolid has been compassionately used with success in the treatment of fluoroquinolone-resistant multidrug-resistant tuberculosis. This review largely discusses six novel drugs that have been evaluated in phase II and III clinical trials, with focus on the clinical evidence for efficacy and safety, potential drug interactions, and prospect for using multiple novel drugs in new regimens.
Abstract
A review of the efficacy, safety, and potential of new drugs to improve TB therapy from the perspective of clinicians http://ow.ly/Das5l
Introduction
Despite the advent of rifampicin and pyrazinamide almost half a century ago, tuberculosis (TB) has remained one of the leading causes of death worldwide [1–6]. Compared with HIV infection, there has been complacency and a lack of interest in TB drug development until the turn of the century. Notwithstanding the recognition of the standard 6-month regimen for drug-susceptible TB as “short-course” [6–11], 6 months is by no means short in comparison with most other bacterial diseases [12].
Not unexpectedly, the United Nations Millennium Development Goal of reversing the global spread of TB by 2015 has been offset by the rampant emergence of multidrug-resistant (MDR) and extensively drug-resistant (XDR) strains of Mycobacterium tuberculosis (fig. 1) [12–15]. Primarily occurring as a result of inadequate treatment, particularly in settings with low cure rates and high rates of default and relapse, MDR-TB refers to TB with bacillary resistance to both isoniazid and rifampicin, and XDR-TB, a subgroup of MDR-TB with additional resistance to any fluoroquinolone and at least one second-line injectable agent. In some areas of Eastern Europe, MDR-TB was found in 20% to 45% of all strains of M. tuberculosis isolated from patients [15].

Anti-tuberculosis drug development and the increase in number of notified multidrug-resistant tuberculosis (MDR-TB) cases worldwide.
MDR-TB poses problems for the global control of TB. Using second-line treatment regimens in programme settings, the overall cure rate is approximately 60% for MDR-TB, and 40% for XDR-TB [16]. Corresponding rates in the current surveillance data from Europe were 32% and 19% of patients, respectively, which are not better than spontaneous cure rates of TB [17]. Routine use of the World Health Organization (WHO) category II regimen for programmatic management of previously treated patients can fuel the spread of MDR-TB [18, 19]. Although second-line treatment-naïve patients with MDR-TB, often caused by fluoroquinolone-susceptible strains of M. tuberculosis, may be successfully treated within 9 to 12 months using second-line regimens that contain high-dose later-generation fluoroquinolone [20], the WHO for many years recommended treatment for 18 months past culture conversion [14] with the latest update in 2011 recommending a total treatment duration of at least 20 months for MDR-TB [21]. Given the need to treat MDR-TB with expensive second-line drugs for a prolonged period [22], drug-resistant TB has drained invaluable resources, thereby offsetting global TB control efforts and threatening to subvert the WHO Stop TB Strategy by diverting attention and resources from the management of drug-susceptible cases, which still represent the main patient group worldwide [23].
Fluoroquinolone-resistant MDR-TB, including XDR-TB, is particularly difficult to treat. As later-generation fluoroquinolones (such as levofloxacin, moxifloxacin, gatifloxacin) may be efficacious against ofloxacin-resistant strains [24], WHO has recommended that later-generation fluoroquinolones be used in the treatment of XDR-TB [14]. A systematic review with meta-analysis of observational studies has corroborated this recommendation by demonstrating that later-generation fluoroquinolones significantly improve treatment outcomes of XDR-TB [25]. Before there is sufficient clinical evidence to support the use of novel drugs in the treatment of MDR-TB, linezolid has been compassionately used as a repurposed agent in the treatment of fluoroquinolone-resistant MDR-TB with success [26–28] and a formal early bactericidal activity (EBA) trial of linezolid is in the final planning stage. A consensus for the management of patients with MDR-TB and XDR-TB has recently been released providing state-of-the-art treatment guidance [29].
The past decade has witnessed the advent of many novel compounds and drugs, of which six have been evaluated in phase II and III clinical trials (fig. 2 and table 1), and two (bedaquiline and delamanid) have been conditionally approved for the treatment of MDR-TB (table 1). Novel drugs will substantially influence future treatment of drug-resistant TB. An important issue is the emergence of bacillary resistance to new drugs, as has happened to streptomycin, isoniazid, and rifampicin after their introduction as a result of multiple avoidable factors [30, 31]. It is thus imperative that novel drugs be used in adequate dosages and combinations under an optimal healthcare infrastructure [32] to forestall the occurrence of drug resistance.
{kind=link}
{kind=link}
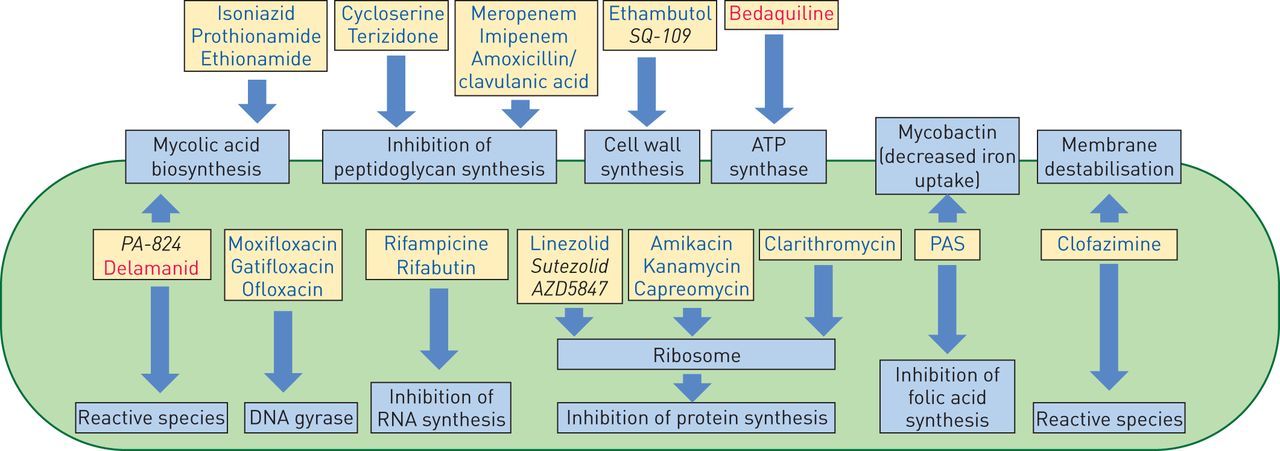
Mechanisms of action of anti-tuberculosis drugs. Drugs already in use are shown in blue, the newly approved drugs are shown in red and drugs undergoing clinical trials are shown in black.
To help clinicians better understand the latest development in the clinical management of drug-resistant TB, this review mainly discusses six novel drugs that have been evaluated in phase II and III trials (bedaquiline, delamanid, PA-824, sutezolid, AZD5847 and SQ109), with focus on the clinical evidence for efficacy and safety, potentially important drug interactions, and prospect for using multiple novel drugs in new regimens.
Novel drugs
Bedaquiline
Bedaquiline is the first novel drug that has been conditionally approved for treating adult pulmonary MDR-TB by the US Food and Drug Administration (FDA) in December 2012, and by the European Medicines Agency (EMA) in March 2014 [33–36].
Bedaquiline (Sirturo, Janssens Pharmaceuticals) is a diarylquinoline with a new mechanism of action. By inhibiting the mycobacterial ATP synthase, thereby leading to intracellular ATP depletion [37], bedaquiline acts on both actively replicating and dormant mycobacteria, which still maintain residual ATP synthase activity [38]. Resistance develops through point mutations in the gene atpE, which encodes part of the ATP synthase, at predictable rates that are similar to those observed for rifampicin. Mutations conferring bacillary resistance to bedaquiline do not cause cross-resistance to other anti-TB drugs, except for clofazimine, possibly due to the upregulation of a multi-substrate efflux pump [39], which has also been found in clinical isolates [40]. With extensive tissue distribution and a long half-life, the recommended dose of bedaquiline for pulmonary MDR-TB in adults is 400 mg once daily for 2 weeks, followed by 200 mg three times weekly, for a total duration of 24 weeks [41].
The clinical evidence for using bedaquiline mainly came from one phase II clinical trial carried out in two stages [41], which showed that adding bedaquiline to a standard background MDR-TB treatment regimen significantly decreased the time to sputum culture conversion with a hazard ratio of 11.8 (95% CI 2.3–61.3), significantly increased the proportion of patients with culture conversion from 9% to 48% at 8 weeks [42], and from 57.6% to 77.6% at 24 weeks [43], and nonsignificantly prevented the acquisition of additional resistance to other accompanying drugs [43].
At the end of the 120 weeks of evaluation period of the trial cure rates according to WHO definitions were 58% in the bedaquiline group and 32% in the placebo group (p=0.003) [44]. However, an unexplained increase in the risk of mortality was observed among the bedaquiline treatment group [43, 44]. Whether bedaquiline may shorten TB treatment, as has been suggested by animal studies [45, 46], should be interpreted with caution as bedaquiline was given with pyrazinamide, and in vitro data have also suggested that its EBA may be substantially dependent on concurrent use of pyrazinamide [47].
Besides an unexplained increase in the risk of mortality, bedaquiline may be associated with nausea, arthralgia, headache, liver injury, and QT prolongation [41]. Although QT prolongation cannot explain the significant increase in the risk of death, both the phase II clinical trial and another single-arm open-label trial have suggested that bedaquiline prolongs QT, and this risk is additively increased by concurrent use of other QT prolonging drugs [41]. It is thus important to take precaution in combining bedaquiline with other QT-prolonging drugs, which include clofazimine, fluoroquinolone (especially moxifloxacin [48]), and delamanid (see below) [49, 50].
Delamanid
Approved by EMA in November 2013 for conditional use in the treatment of MDR-TB, delamanid is the second (and the last one to date) novel drug that has been licenced for treating adult pulmonary MDR-TB [51, 52].
Delamanid (Deltyba, Otsuka Pharmaceuticals) is a derivative of metronidazole and a nitroimidazopyran (nitro-dihydro-imidazooxazole, 6-nitro-2,3-dihydroimidazo(2,1-b) oxazole). As a prodrug that requires activation for pharmacological activity, delamanid works by inhibiting mycolic acid biosynthesis. There is as yet no recommendation about dosage, pending the release of data from a completed multi-centre phase III trial that has evaluated use of delamanid 100 mg twice daily for 2 months followed by 200 mg once daily for 4 months. By sharing similar structure as nitro-dihydro-imidazooxazole derivatives, there may be cross-resistance between delamanid and PA-824 [53].
The clinical evidence for using delamanid is based on short-term phase II clinical trial data. A phase II multi-centre randomised placebo-controlled trial involving 481 MDR-TB patients showed that delamanid added to an optimal background regimen significantly increased the proportion with sputum culture conversion at 2 months from 29.6% (placebo) to 45.4% (delamanid 100 mg twice daily), and 41.9% (delamanid 200 mg twice daily) [49]. An open-label extension of this phase II trial showed that delamanid use for more than 6 months in comparison with use for less than 2 months significantly increased the proportion with favourable outcomes (cure or treatment completion) from 55% to 74.5% and significantly reduced mortality from 8.3% to 1.0% [54].
Delamanid significantly prolongs the QT interval from 3.8% (placebo arm) to 9.9% (delamanid 100 mg twice daily) and 13.1% (delamanid 200 mg twice daily) [49]. Despite the lack of clinical events [49], it is thus important to increase vigilance when combining delamanid with bedaquiline, clofazimine, and fluoroquinolones (especially moxifloxacin).
PA-824 (pretomanid)
PA-824 is a bicyclic nitroimidazole and a prodrug that requires intracellular activation by a F420-dependent glucose-6-phosphate-dehydrogenase pathway. Activation produces a des-nitro metabolite that generates reactive nitrogen species (including NO) leading to a decrease in intracellular ATP and anaerobic killing (similar to the action of cyanide) [55, 56]. Although PA-824 seems to be more effective in anaerobic conditions [57], it also kills aerobically by inhibiting cell wall mycolic acid biosynthesis (similar to the action of isoniazid) [56]. As such, PA-824 expectedly showed activity against both replicating and non-replicating bacteria [58], and both drug-resistant and drug-susceptible TB [58–61]. Mutations have been identified in fgd1 and ddn [57, 62, 63], with cross-resistance to 5-nitrothiophenes (a tuberculostatic compound) [64] as well as delamanid [53]. With minimal inhibitory concentration (MIC) around 0.15–0.3 μg·mL−1 [58, 63], the activity of PA-824 is comparable to a combination of isoniazid and rifampicin in the continuation phase of a murine drug model [61]. As a large fraction of the active compound is plasma bound, its activity may be reduced in cavitary TB [65].
A phase II randomised controlled trial of EBA (NC-003) involving patients with smear-positive pulmonary TB suggested that the EBA of PA-824 was greatly dependent on its synergy with pyrazinamide, and a triad of PA-824, moxifloxacin and pyrazinamide gave the highest EBA, thereby suggesting its potential for further clinical trials [47]. The treatment efficacy of this triad has been evaluated in a phase II randomised controlled trial, pending the release of findings [66].
In humans, PA-824 has been well tolerated with constant pharmacodynamic parameters when given once daily, with the maximum serum drug level reached about 4–5 h following oral administration [59, 67, 68]. In a phase II dose-finding EBA study in which PA-824 was given over 14 days, the drug appeared safe and efficacious when given between 100 mg and 200 mg once daily [69]. PA-824 might induce a mild QT-interval prolongation [69] as well as a slight transient increase in creatinine that is not linked to a decrease in the glomerular filtration rate [59]. The effect of PA-824 and moxifloxacin in combination on the QT-interval is currently under evaluation [70].
Sutezolid
Sold to Sequella in July 2013, sutezolid (PNU-100480) is a linezolid analogue initially developed by Pfizer for evaluation of potentially better in vivo activity and less toxicity in comparison with linezolid [71]. With a substantially lower MIC against M. tuberculosis and reduction of MIC in acidic pH, sutezolid has demonstrated higher bactericidal activity than linezolid, as well as perhaps potential sterilising activity [72]. The whole-blood bactericidal activity of sutezoid 600 mg twice daily is higher than that of linezolid 300 mg once daily [73]. Although the EBA of sutezolid is significantly lower than that of the standard regimen [74] a whole blood bactericidal activity assay has demonstrated its synergistic activity with pyrazinamide [73].
Sutezolid does not appear to cause QT-interval prolongation or bone marrow suppression [73], although there are still concerns regarding potential neurotoxicity and hepatotoxicity. With a similar mitochondrial protein synthesis safety profile as linezolid 300 mg once daily, prolonged use of sutezolid 600 mg twice daily may cause peripheral neuropathy [27, 75]. A phase II randomised controlled trial of EBA has demonstrated the occurrence of transient and asymptomatic elevation of alanine transaminase among 14% patients in the sutezolid arm [74].
AZD5847
Like linezolid, AZD5847 is an oxazolidinone that inhibits mycobacterial protein synthesis by binding to the 50S ribosomal subunit; its in vitro bactericidal activity is superior to that of linezolid [76]. AZD5847 appears to be safe and well tolerated in healthy volunteers, with nausea being the most common adverse effect occurring at higher dosages [77]. A phase IIa trial of EBA with four different dosing strategies has been completed and results will hopefully be available in 2014 [78].
SQ109
Structurally related to ethambutol, SQ109 is a 1,2-ethylenediamine with a different mechanism of action and preserved activity against ethambutol-resistant M. tuberculosis isolates. Targeting the transmembrane transporter encoded by the mmpL3 gene, SQ109 interferes with cell wall assembly [79].
In Russia and Kazakhstan, clinical trials of 6 months of SQ109 added to a background MDR-TB treatment regimen given over 18 months will be compared to the background regimen alone. However the number of patients is relatively small and the resulting data might not suffice to register SQ109 outside Russia and the Commonwealth of Independent States [80].
SQ109 appears to be safe and well tolerated in human studies. However, all SQ109-containing arms have been terminated in the multi-arm, multi-stage trial due to lack of sufficient efficacy.
Interactions with antiviral drugs and azoles
TB disease commonly coexists with HIV that requires simultaneous treatment with antiviral drugs. Azoles may be used among immunocompromised patients with coexisting fungal infection.
Bedaquiline is metabolised via the cytochrome (CYP) P450 3A4 leading to the formation of a much less active but potentially more toxic N-monodesmethyl metabolite [81]. In one study bedaquiline given with efavirenz, which is a CYP3A4 inducer [82], led to only a slight decrease in bedaquiline concentrations [83]. In contrast a nonlinear-mixed effects model evaluating the interaction between bedaquiline and efavirenz predicted that simultaneous treatment would lead to a 52% reduction in steady state concentrations of both bedaquiline and its metabolite. Reduced exposure could be prevented by adjusting the bedaquiline dose during concomitant treatment [81]. Co-administration of bedaquiline with nevirapine did not influence bedaquiline exposure [84]. Bedaquiline should be used with caution in patients receiving ritonavir-boosted lopinavir because co-administration was shown to cause a 22% increase in bedaquline exposure [72, 85].
It has been estimated that 30% of sutezolid and 20% of PA-824 are also metabolised by CYP3A4 [86]. Co-administration of PA-824 and efavirenz reduces the peak serum concentration and the area under concentration–time curve of PA-824 each by around 30%. Clinical significance is unknown [73].
With no influence on the CYP enzymes, delamanid has a low potential for drug interactions. There are no clinically significant changes in drug exposure on co-administration of delamanid with efavirenz [87], ritonavir-boosted lopinavir or tenofovir [88].
SQ109 is neither activated nor metabolised via CYP3A4, but it is partially metabolised by CYP2C19, which is in turn strongly inhibited by fluconazole [86, 89]. The clinical implications of these interactions are yet to be investigated.
Clinical trials involving novel drugs used in combination
To expedite the development of better TB treatment, it is probably necessary to use novel drugs in combination to formulate new TB drug regimens that rapidly reduce mortality and infectiousness with good bactericidal activity, maximally safeguard against the emergence of bacillary drug resistance with different mechanisms of action and, preferably, shorten treatment with prominent sterilising activity [90]. Given relatively scarce data on the use of novel drugs in combination, vigilance is always needed to closely monitor potential drug interactions and toxicity.
As bacillary resistance to fluoroquinolones [91, 92] and pyrazinamide [93, 94] is substantial among patients with MDR-TB, particularly in some geographical areas, it is probably better to use at least two, and perhaps three, novel drugs in combination, notwithstanding the preliminary promising activity from use of single novel agents, such as PA-824 alongside moxifloxacin and pyrazinamide [47]. This approach would help better safeguard against the amplification of bacillary resistance to both novel and existing TB drugs.
There are at least two conducted clinical trials involving novel drugs used in combination. The Global Alliance for TB Drug Development (TB Alliance) has sponsored a phase II randomised controlled trial of EBA (NC-001) involving patients with smear-positive pulmonary TB, which showed that the multi-agent EBA of PA-824 and bedaquiline was substantially lower than that of pyrazinamide with either PA-824 or bedaquiline [47]. The TB Alliance has also spearheaded a phase II randomised controlled trial involving patients with smear-positive pulmonary TB to further evaluate the EBA of PA-824 and bedaquiline in the presence of clofazimine, pyrazinamide or both [95].
There are at least two planned trials that will evaluate regimens containing multiple novel drugs: NiX-TB and MARVEL [78]. NiX-TB is a phase III non-controlled trial of a 6-month salvage regimen comprising linezolid, bedaquiline and PA-824. MARVEL is a phase II study of 8-week treatment with various combinations of sutezolid, bedaquiline, PA-824, pyrazinamide, levofloxacin and clofazimine.
A number of factors might have influenced the choice of combining novel drugs in clinical trials: in vitro data and findings from murine TB models about efficacy of certain combinations (table 2), concerns about life-threatening arrhythmia during concurrent use of novel (bedaquiline, delamanid) and existing (moxifloxacin, clofazimine) QT-prolonging drugs, synergistic activity of most novel drugs (bedaquiline, delamanid, PA-824, sutezolid) with pyrazinamide [53, 73, 99, 100], and possibly the relative difficulty in procuring delamanid and SQ109 in clinical trials.
Novel designs for clinical trials
Useful for screening and selecting potential drug candidates, in vitro data and animal models can never replace clinical trials in the evaluation of treatment efficacy and safety. Murine TB models have important disadvantages including the lack of full knowledge on the bioequivalent doses and also difference in pathogenetic mechanisms. There have been instances when observations derived from murine TB models were discordant with those observed in human trials [101]. Additionally, given the current recommendation of treating MDR-TB for nearly 2 years [21], and the small sample size often used in animal experiments, it is difficult to evaluate sterilising activity in non-primate animal models.
The required sample size increases with the stage of drug development (table 3). In the absence of reliable surrogate markers for treatment outcomes, it is challenging to thoroughly evaluate treatment efficacy and safety in phase III clinical trials. In an attempt to expedite drug development, new methods such as EBA studies and multi-arm, multi-stage adaptive design have been adopted, although none can replace phase III trials.
EBA studies measure the fall in colony forming units (CFU) or the time to detection in liquid culture. This method provides reproducible results regarding efficacy although it does not reliably predict sterilising activity. The technique is mainly used for dose finding and preliminary evaluation of toxicity in a small sample [102] up to 14 days. Using this approach to evaluate PA-824, it has been shown that the mean multi-agent 14-day EBA of PA-824, moxifloxacin and pyrazinamide is comparable with that of the current standard treatment and significantly higher than those of bedaquiline, bedaquiline with pyrazinamide, and bedaquiline with PA-824 [47].
Previously used in other fields such as oncology, multi-arm, multi-stage adaptive design involves planned interim analyses at pre-specified time points to expedite the evaluation of different arms [103]. Weaker arms that do not meet pre-specified efficacy criteria are terminated, thereby focusing resources on alternative arms that are potentially more efficacious. Additionally, new arms can be flexibly added while the trial is in progress. A caveat is the need of reliable surrogate biomarkers at the pre-specified time points and an adequate number of comparison arms. Meanwhile, the hunt for reliable biomarkers and biosignatures that could help clinicians personalise TB treatment continues. Candidate markers are still in preclinical or early clinical evaluation; none can be recommended for routine use [12].
In the evaluation of new treatment combinations, it cannot be overemphasised that clinical trials be designed such that the risk of acquiring bacillary resistance to novel drugs is minimised.
Future outlook
In the coming decade, there are likely some newly developed anti-TB drugs that can substantially improve the current treatment of MDR/XDR-TB. Although the high efficacy of the newly developed anti-TB agents is unequivocal, the safety and tolerability of these novel drugs [104, 105] remain to be further evaluated in larger studies, and the resources that would be incurred are yet to be determined.
In harnessing repurposed agents to strengthen current treatment regimens for drug-resistant tuberculosis [106, 107] it is highly warranted to fathom novel approaches in the administration schedules that can concomitantly optimise the efficacy and safety of these drugs, especially linezolid. Further studies involving sizeable samples may be required to delineate the clinical role of other repurposed agents, which include clofazimine, meropenem and other carbapenems, thioridazine, and possibly co-trimoxazole [106].
Pharmacogenomics furnish great promise as an important tool to help in the evaluation of drug-associated toxicity [108], using different animal models including the mouse, possibly the zebra-fish [109] and non-human primates [110]. Such data might also have utility in clinical trials and settings to manage toxicity incurred by anti-TB drugs [111].
There are grounds for rekindling an interest in exploring the inhaled route of drug administration [112]. In the 1950s, streptomycin was first successfully used by an inhaled route to treat childhood TB with advanced radiographic lesions [113]. The advent of MDR-TB prompted further exploration using inhaled kanamycin and gentamicin [112, 114, 115]. The rationale was to attempt delivering a higher dose of the aminoglycoside to achieve better efficacy, without concomitant escalation in systemic toxicity, in these formidable drug-resistance settings. The preliminary results portrayed good patient outcome. A recent phase I, single-dose, dose-escalating study aimed at demonstrating the safety and tolerability of capreomycin, administered through a dry powder inhalational device in healthy subjects [116]. By the same token, much enthusiasm has been devoted to exploring the potential use of inhaled clofazimine in the treatment of pulmonary TB [112]. A recent study examined the efficacy of inhaled riminophenazine in dry powder leucine microparticles against M. tuberculosis in the human macrophage cell culture and aerosol-infected mouse model [117]. The inhaled route of delivering fluoroquinolones has also been studied in some preliminary experiments using ofloxacin [118] and levofloxacin [119], respectively. If a high-dose fluoroquinolone given by the oral route is limited by tolerability, as shown in the ongoing trials, an alternative approach may be to combine the oral and inhaled routes of drug delivery. Use of inhaled pyrazinamide proliposome for targeting alveolar macrophages has been recently evaluated [120]. A similar approach may be considered for novel drugs such as PA-824, which has been administered in dry powder aerosol to guinea pigs with less rapid clearance from the lungs by the inhalation route than oral delivery [121, 122]. However, it might be simpler to licence the use of a repurposed agent through a new route of delivery than a novel drug.
Host immunity plays a pivotal role in the manifestation of TB disease. Adjunct immunotherapy, which includes host-directed therapies with immunoadjuvants [123–125], recombinant cytokines [126–128] or therapeutic vaccinations [128–138], should be further explored to possibly improve the treatment outcome of drug-resistant TB, especially difficult forms of MDR/XDR-TB [139].
TB with increasingly drug-resistant forms has clearly posed a gigantic threat to global health. With rapidly evolving development of new diagnostic tools and drugs, the battle against this old foe of mankind may not be insurmountable.
Footnotes
Support statement: C. Lange is funded by the German Center for Infection Research (DZIF).
Conflict of interest: Disclosures can be found alongside the online version of this article at erj.ersjournals.com
- Received September 3, 2014.
- Accepted October 9, 2014.
- Copyright ©ERS 2015
References










