





Abstract
The association between bronchiolitis and recurrent wheezing remains controversial.
In this prospective study, we assessed risk factors for recurrent wheezing during a 12-month follow-up in 313 infants aged <12 months hospitalised for their first episode of bronchiolitis. Demographic, clinical and laboratory data were obtained with a questionnaire and from medical files. A total of 14 respiratory viruses were concurrently assayed in nasal washings. Parents were interviewed 12 months after hospitalisation to check whether their infants experienced recurrent wheezing.
The rate of recurrent wheezing was higher in infants with bronchiolitis than in controls (52.7 versus 10.3%; p<0.001). Multivariate analysis identified rhinovirus (RV) infection (OR 3.3, 95% CI 1.0–11.1) followed by a positive family history for asthma (OR 2.5, 95% CI 1.2–4.9) as major independent risk factors for recurrent wheezing.
In conclusion, the virus most likely to be associated with recurrent wheezing at 12 months after initial bronchiolitis is RV, a viral agent that could predict infants prone to the development of recurrent wheezing.
Bronchiolitis, an airway disease primary located in the small peripheral bronchioles, is among the major causes of hospital admission in infants aged <1 yr [1]. Bronchiolitis can also cause long-term respiratory sequelae. Despite numerous clinical studies conducted since the 1950s to investigate the association between bronchiolitis and the subsequent development of asthma, the link between recurrent wheezing, asthma, atopy and bronchiolitis remains controversial [2–4]. The main reason for this is that bronchiolitis is a clinical diagnosis encompassing various disease entities whose immunopathogenesis differs according to viral aetiology, wheezing phenotype and preceding inflammatory state. About half the clinical trials conducted over recent years have used 12 months, and the remaining 24 months, as an upper age limit of bronchiolitis, and half the studies have focused on the first episode of wheezing [5]. A study conducted in children with suspected bronchiolitis showed that the two clinical factors linked to inflammatory (atopy-related factors) and virological risk factors for asthma are age and number of previous wheezing episodes [5]. To avoid confounding in long-term results, prospective follow-up studies designed to determine how genetic predisposition, demographic characteristics and viral aetiology influence the development of recurrent wheezing and asthma should define bronchiolitis according to strict clinical criteria, excluding asthma-prone children.
Although infants hospitalised for bronchiolitis are frequently infected with other viruses, the primary infection causing bronchiolitis is respiratory syncytial virus (RSV) [6]. To date, most studies on recurrent wheezing and asthma after bronchiolitis have focussed nearly exclusively on RSV, but increasing, evidence now suggests that other viruses, and principally rhinovirus (RV), play an equally important role [7–9].
In a well-characterised cohort of infants aged <12 months with acute bronchiolitis, we have already shown that although the major pathogen responsible for bronchiolitis remains RSV, the infection can also be caused by RV and human bocavirus (hBoV) [6]. Few data are available on the relationship between respiratory viruses other than RSV and recurrent wheezing after bronchiolitis in infants aged <1 yr [10].
Our main purpose in this prospective, single-centre study designed to continue our previous research [6] was to assess the risk factors for recurrent wheezing during a 1-yr follow-up in a well-characterised, homogeneous cohort of infants aged <1 yr hospitalised for the first episode of acute bronchiolitis caused by RSV and other respiratory viruses. We concurrently assayed a battery of 14 viruses known to cause bronchiolitis. To analyse possible risk factors for recurrent wheezing, we obtained demographic, clinical and virological features at hospital admission, and compared rates of recurrent wheezing 12 months later.
PATIENTS AND METHODS
Patients
We prospectively enrolled 313 consecutive full-term infants (median age 2.0 months, range 7 days–11 months; 170 (54%) males) with a diagnosis of acute bronchiolitis hospitalised in the Paediatric Emergency Department (“Sapienza” University Rome, Rome, Italy) during five consecutive annual epidemic periods from October 2004 to the end of May 2005, October 2005 to the end of May 2006, October 2006 to the end of May 2007, October 2007 to the end of May 2008, and October 2008 to the end of May 2009.
Bronchiolitis was defined as the first episode of acute lower airway infection characterised by a history of upper respiratory tract infection followed by acute onset of respiratory distress with cough, tachypnoea, retraction and diffuse crackles on auscultation (having wheezing alone was not considered sufficient for inclusion in the study) [11]. Exclusion criteria were underlying chronic diseases (including cystic fibrosis, chronic pulmonary disease, congenital heart disease and immunodeficiency).
Controls
We prospectively enrolled 39 consecutive infants (median age 4.2 months, range 24 days–12 months, 17 (44%) males) with an acute disease unrelated to the respiratory system, hospitalised in our paediatric department during the first annual epidemic period from October 2004 to the end of May 2005. Detailed demographic, clinical and laboratory data were obtained from parents of patients and controls with a structured questionnaire and from patients' medical files. Studied variables included age at recovery, sex, type of delivery, breastfeeding history, family smoking habits, number of siblings, family history of asthma and atopy, presence of atopic eczema, white blood cell count, blood eosinophil count, blood C-reactive protein (CRP) concentration, chest radiological findings and number of days hospitalisation. On hospital admission, each infant was assigned a clinical severity score ranging from 0 to 8 according to respiratory rate (0: <45 breathes per min; 1: 45–60 breathes per min; 2: >60 breathes per min), arterial oxygen saturation in room air (0: >95%; 1: 95–90%; 2: <90%), presence of retractions (0: none; 1: present; 2: present plus nasal flare) and ability to feed (0: normal; 1: reduced; 2: intravenous fluid replacement) [6].
Parents of all infants were asked to participate in the study and gave written informed consent. The study was approved by the hospital institutional review board (Dept of Paediatrics, Policlinico "Umberto I", "Sapienza" University of Rome, Italy).
Follow-up
At 12 months after discharge, one of the authors (F. Midulla) interviewed parents of all infants using a standardised telephone procedure with a structured questionnaire seeking information on recurrent wheezing. Of the 39 families in the control group, all replied, whereas of the 313 families of infants with bronchiolitis contacted, only 262 (83.7%) replied (fig. 1). The only reason for drop-out was a change in telephone number. The term “recurrent wheezing” was defined as two or more physician-verified episodes of wheezing during a 1-yr follow-up. None of the control infants had bronchiolitis during the first year of life.

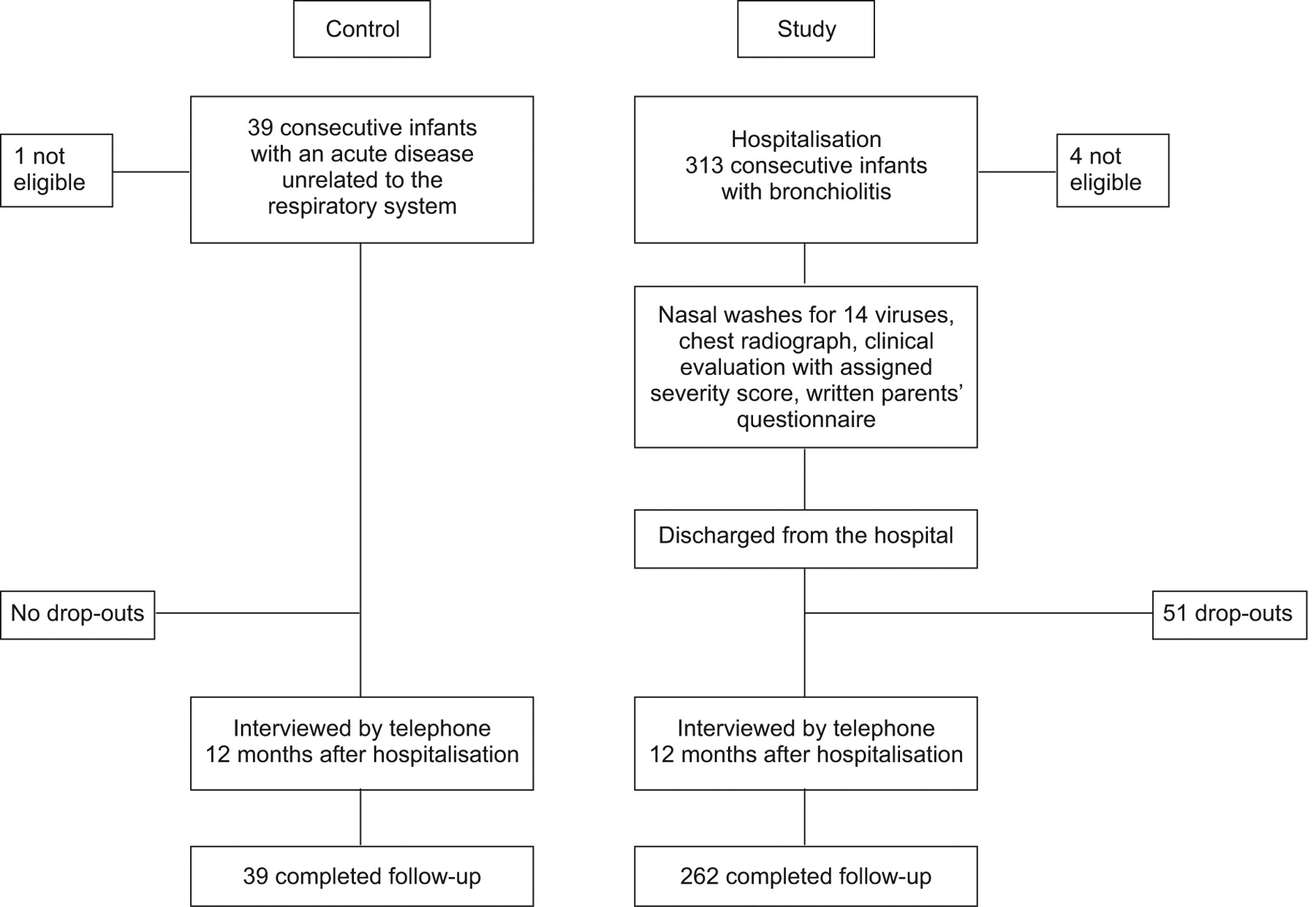{kind=link}
Study flow chart.
Virus detection
From 1 to 3 days after hospitalisation, all infants underwent nasal washing obtained with 3 mL sterile saline solution injected into each nostril and collected with a syringe. All samples were delivered on ice within 1–2 h to the virology laboratory and on arrival, if needed, they were vortexed with beads to dissolve mucous. 200 μL of respiratory specimens was subjected to nucleic acid extraction with the total nucleic acid isolation kit (Roche Diagnostics, Mannheim, Germany), eluting with 50 μL of the supplied elution buffer. A panel of either reverse transcriptase (RT)-PCR or nested PCR assays was developed for detecting 14 respiratory viruses, including RSV, influenza virus (IV) A and B, human coronavirus (hCoV) OC43, 229E, NL-63 and HUK1, adenovirus, RV, parainfluenza virus (PIV) 1–3, hBoV and human metapneumovirus (hMPV), as previously described [12]. During the course of the study, a novel group of previously unrecognised human rhinoviruses was recognised, established and named RV species C [13]. The RV PCR primers used throughout our study target highly conserved regions in the 5′-untranslated region (UTR) (forward primer position 436–453, reverse primer position 537–555, according to human RV35 genome numbering), corresponding to the P2 and P3 regions reported as conserved among all RV genotypes, including RV group C [13]. Hence, our RV PCR primers almost certainly detected RV C, as well as RV species A and B. Even though RV genotyping was beyond the purpose of this study, we retrospectively tried to amplify a larger genomic sequence in the 5′-UTR [14] from frozen stored samples to prove RV C detection. Owing to the frailty of the respiratory samples stored at -80°C for a number of years, we succeeded in sequencing and genotyping only nine RV-positive samples, seven being RV A- and two RV C-positive.
At study entry on admission, a total of 195 viruses were detected in the nasal wash specimens from 174 (55.6%) of the 313 infants with bronchiolitis: RSV was found in 130 (74.7%), hBoV in 25 (14.4%), RV in 24 (13.8%), PIV 1–3 in six (3.4%), hMPV in five (2.8%), IV A in two (1.1%) and hCoV in one (0.6%). Of the 130 RSV-positive infants, 15 (11.5%) had co-infection with hBoV, one with IV A, one with PIV 3 and one with RV. One of the hMPV-positive infants had co-infection with hBoV and one with RV. No viruses could be detected in nasal wash specimens from 139 (44.4%) infants. The prevalence of respiratory viruses in our study sample has been addressed in a previous study [6].
Statistical analysis
A descriptive analysis included calculating percentages, mean±sd and median (range) for demographic variables and virological results. Distributions of continuous variables were examined for skew and kurtosis. Differences between groups (with or without recurrent wheezing) were tested for significance using an unpaired t-test (two-tailed) for normally distributed data or nonparametric Mann–Whitney test for non-normally distributed data. The Chi-squared test was applied to analyse categorical independent variables qualitatively. Multivariate logistic regression models were used to identify clinical and virological variables associated with the main end-points (to assess the risk factors for recurrent wheezing during a 1-yr follow-up after the first episode of acute bronchiolitis caused by RSV and other respiratory viruses). Only variables with p<0.15 in the univariate analysis were included in the multivariate model. Results from logistic models were described by odds ratios and 95% confidence intervals. p-values <0.05 were considered to indicate statistical significance. Data were analysed using SPSS version 13.0 (SPSS Inc., Chicago, IL, USA).
RESULTS
Infants with bronchiolitis versus controls
No differences were observed for sex, family history of asthma, family history of atopy and smoking exposure between infants with bronchiolitis and controls. The median age was higher in the control group than in infants with bronchiolitis (4.2 months, range 24 days–12 months versus 2.0 months, range 7 days–11 months; p<0.001). Within the first year after hospital admission for bronchiolitis, a higher percentage of infants with bronchiolitis had episodes of recurrent wheezing than controls (52.7% versus 10.3%; p<0.001).
Children hospitalised for acute bronchiolitis with and without recurrent wheezing
Of the 262 infants whose parents answered the telephone interview at the 1-yr follow-up, 138 (52.7%) infants experienced recurrent wheezing and 124 (47.3%) did not. Several demographic characteristics differed in infants with and without recurrent wheezing. For example, the percentage of male infants was higher in the group with recurrent wheezing than in that without, albeit not significantly (60.9% versus 50.8%; p<0.09). Infants with recurrent wheezing also had a significantly higher rate of family history of asthma than infants without recurrent wheezing (28.3% versus 14.3%; p<0.001). No significant differences were found in relation to demographic characteristics, including type of delivery, birthweight, age at recovery, weight at recovery, breastfeeding, exposure to smoking, family history for atopy, atopic eczema, clinical severity score and days of hospitalisation (table 1).
The total number of blood eosinophils and the percentage of infants with an absolute number of blood eosinophils >400 cells·μL−1 were higher in infants with recurrent wheezing than in those without (p<0.01 and p<0.02). The number of children with a CRP concentration <0.8 mg·dL−1 and absence of lung consolidations on chest radiograph differed significantly between children with and without recurrent wheezing (p<0.01 and p<0.01) (table 1).
The distribution of viruses differed in infants with and without recurrent wheezing (table 2). The rates of recurrent wheezing differed also according to the virus causing acute bronchiolitis: 80% for RV, 66.7% for hBoV, 50% for other viruses, 45.5% for RSV plus hBoV (p<0.05 versus RV) and 43.3% for RSV (p<0.005 versus RV).
Odds ratios assessing possible demographic and clinical factors influencing the development of recurrent wheezing after acute bronchiolitis indicated an increased risk of wheezing during the first year of follow-up for blood eosinophils >400 cells·μL−1 (OR 4.9, 95% CI 1.1–22.9), RV bronchiolitis (4.0, 1.3–12.2), family history for asthma (2.7, 1.5–4.9), CRP <0.8 mg·dL−1 (1.9, 1.1–3.1) and absence of lung consolidation (1.7, 1.0–3.1).
The multivariate logistic regression model identified RV infection (3.3, 1.0–11.1) as the most important independent risk factor for recurrent wheezing followed by a positive family history for asthma (2.5, 1.2–4.9). Another independent risk for recurrent wheezing was the absence of lung consolidation on chest radiograph (2.6, 1.1–6.1) (table 3).
DISCUSSION
In this prospective, single-centre study conducted in a university hospital paediatric department, we found that among infants aged <1 yr hospitalised for their first episode of acute bronchiolitis, those with bronchiolitis caused by RV and a positive family history of asthma have a substantially higher risk for recurrent wheezing during 1-yr follow-up after their initial episode than those with bronchiolitis caused by RSV and other respiratory viruses.
A distinctive point in our study is that unlike previous studies, we prospectively investigated recurrent wheezing in a clinically well-characterised cohort of infants aged <12 months admitted to hospital for their first episode of acute bronchiolitis, already studied in our previous research [6], and also assayed their nasal washes simultaneously for a large battery of 14 different respiratory viruses. Conversely, other studies defined bronchiolitis differently (infants aged <24 months and with wheezing) and enrolled only those with RSV bronchiolitis [15–17].
Our decision to define bronchiolitis according to strict clinical criteria ensured that we provide homogeneous data suitable for future prospective long-term follow-up and excluded patients with various differing clinical entities, such as wheezing bronchitis, and asthma-prone children. Despite its high frequency, bronchiolitis remains a clinical diagnosis without a common international definition. Whereas some investigators define bronchiolitis as an episode of viral wheezing in infants aged <24 months [18], others define it as the first episode of a lower respiratory tract infection with diffuse bilateral crackles in infants aged <12 months of age [11]. By selecting infants aged <12 months with their first acute respiratory infection and crackles at chest auscultation, our study therefore avoids factors that might confound clinical trials and long-term follow-up of bronchiolitis. It also provides new evidence underlining how risk factors such as genetic predisposition, demographic characteristics and viral aetiology can influence the development of recurrent wheezing.
When we analysed the number of infants with episodes of recurrent wheezing during a 1-yr follow-up, as expected, we found a considerably higher rate of recurrent wheezing in infants with bronchiolitis than in the control group (52% versus 10.3%). Notwithstanding these findings, like other studies, we found similar hereditary factors in infants with and without bronchiolitis [4, 15–17]. In their longitudinal study, Sigurs et al. [17] also found that despite similar hereditary factors in infants with and without bronchiolitis, a significantly larger percentage of the infants with RSV bronchiolitis had episodes of recurrent wheezing after a 1-yr follow-up [17]. Collectively, these findings confirm that having bronchiolitis during the first year of life is a risk factor for the subsequent development of recurrent wheezing [3–4, 17]. The mechanisms underlying this increased incidence of wheezing after bronchiolitis are still unclear [19, 20].
When we compared demographic characteristics and clinical findings in infants with and without recurrent wheezing after bronchiolitis, we found several differences. First of all, we confirmed the tendency towards male predominance in infants with recurrent wheezing [17]. The slightly higher frequency of wheezing in males seems to fit in well with current knowledge that high airway resistance in male infants and low functional residual capacity in female infants predispose male infants to wheezing in association with lower respiratory tract infection [21].
Two demographically and clinically important differences we observed between the two groups were the significantly higher percentage of infants with a positive family history for asthma and the significantly higher number of blood eosinophils in infants with recurrent wheezing. Other studies of bronchiolitis also found heredity for asthma and blood eosinophilia risk factors for the development of recurrent wheezing and asthma [22, 23]. Hence, infants with bronchiolitis in whom wheezing develops might be genetically predetermined to do so, and severe respiratory disease might ultimately develop whatever respiratory virus they encounter early in life. This finding is in accordance with Ehlenfield et al. [24], who concluded that eosinophilia at the time of bronchiolitis predicts the development of wheezing persisting into later childhood. Whether eosinophils play important roles in the onset of recurrent wheezing or are just a marker of allergic symptoms remains uncertain.
Another finding that may help to characterise children with recurrent wheezing was the significant difference between the two groups in the blood CRP level and in the percentage of infants with radiological lung consolidations. Infants with recurrent wheezing had a lower blood CRP concentration and a fewer radiologically documented lung consolidations than nonwheezing infants. These radiological findings suggest that the two groups of infants (those with and those without recurrent wheezing) differ not only in having risk factors for atopy and asthma (family history of asthma and eosinophilia), but also in their pathogenetic response to the different viruses.
Finally, in the group of infants with bronchiolitis, when we analysed the rate of recurrent wheezing in relation to specific viruses detected during the illness, we found a larger number of infants with recurrent wheezing among infants with RV than among those with hBoV, RSV, dual infection with RSV and hBoV, and other respiratory viruses. Multivariate logistic regression analysis of possible risk factors for the development of recurrent wheezing during 1 yr after the acute episode of bronchiolitis in the 138 infants identified RV bronchiolitis as by far the most important risk factor, whereas bronchiolitis from RSV and other respiratory viruses was not a risk factor. These so far unreported findings obtained by strictly defining bronchiolitis and simultaneously assaying 14 respiratory viruses provide reliable data that may confirm previous reports in various clinical settings that infants in whom RV is detected are those predisposed to asthma and atopy. Several studies conducted over the past 5 yrs have shown the relationship between RV infection in the first years of life and the development of recurrent wheezing and asthma. In two community-based cohort studies, Regamey et al. [25] and Kusel et al. [26] have shown that RV is the most frequent virological agent in upper and lower respiratory tract infections in both unselected infants and in infants with risk factors for atopic sensitisation followed for 1 yr. In their study evaluating how RV infection contributed to the subsequent development of wheezing during infancy in a high-risk birth cohort, Jackson et al. [8] found that moderate-to-severe RV wheezing illness in infancy was the most significant risk factor not only for the development of pre-school wheezing at the age of 3 yrs, but also for the development of asthma at age 6 yrs. Similar results came from a follow-up study of 82 infants aged <2 yrs, hospitalised for infection associated with wheezing and evaluated 3 yrs later, conducted by Kotaniemi-Syrjänen et al. [9], who found that RV infection leading to hospitalisation during infancy was an early predictor of the subsequent development of asthma. Finally, in a retrospective study with a 3-yr follow-up, Valkonen et al. [27] showed that recurrent wheezing develops at substantially higher rates in infants hospitalised with bronchiolitis (<2 yrs of age) caused by viruses other than RSV than in children with RSV-induced bronchiolitis. Unfortunately, in that early study, the investigators were unable to look for other respiratory viruses in infants with non-RSV bronchiolitis. Overall, the various reported results suggesting that the risk of wheezing develops after an initial episode of bronchiolitis in infancy differs according to the type of viral infection. The aforementioned studies all differ from our study in several important ways. First, in defining bronchiolitis, they included infants aged >12 months. Secondly, because they failed to specify whether they studied the first episode of bronchiolitis, they could have included infants with other clinical entities (wheezing bronchitis). Thirdly, none of the studies simultaneously tested for 14 different respiratory viruses likely to cause bronchiolitis.
Current knowledge therefore clearly links RV bronchiolitis and recurrent wheezing during the first year of life. It therefore raises the question whether RV bronchiolitis actually causes recurrent wheezing. Alternately, RV bronchiolitis might serve to disclose infants who are already predisposed to this disease owing to abnormal lung physiology or immune response, or both. Indeed, RV seems to preferentially affect the lower airways, causing bronchiolitis in atopic children prone to wheezing [28–30].
Our study has limitations. First, we studied fewer infants with RV than with bronchiolitis from RSV and other respiratory viruses. Secondly, we could not confirm whether parents gave reliable information in the phone interview. Thirdly, as we discussed in our previous article [6], our virus detection rate was poor. Finally, we did not test for RV subtypes, in particular species C.
In conclusion, the major risk factors for wheezing episodes after acute bronchiolitis are RV infection and a positive heredity for asthma. A major goal for future research efforts should therefore be to define genetic, environmental and viral factors that promote wheezing after RV bronchiolitis. A longer serial follow-up will show whether RV infection identifies those infants predisposed to persistent wheezing.
Footnotes
For editorial comments see page 238.
Support Statement
This study was supported by grants to G. Antonelli, F. Midulla and A. Pierangeli from “Sapienza” Università Roma (Fondi Ricerche Universitarie), and by grants to G. Antonelli and A. Pierangeli from the Italian Ministry of Health (Ricerca Finalizzata Conv. no. 88) and Pasteur Institute, Cenci Bolognetti Foundation.
Statement of Interest
None declared.
- Received December 7, 2010.
- Accepted July 4, 2011.
- ©ERS 2012
REFERENCES










