





Abstract
Inhaled glucocorticosteroids may reduce airway mucosal oedema in acute asthma. Inhaled platelet-activating factor (PAF) provokes pulmonary gas exchange disturbances, similar to those shown in severe asthma, which may be due to increased airway plasma leakage.
This randomized, double-blind, placebo-controlled, crossover study investigated the effects of high doses of inhaled fluticasone propionate (FP) in 12 patients with mild asthma before and after PAF inhalation. Patients were studied before and 12 h after inhaling FP (6 mg) or placebo (P), and then at 5, 15 and 45 min after PAF challenge.
Compared with vehicle, FP inhaled before PAF improved forced expiratory volume in one second and respiratory system resistance (Rrs), increased peripheral blood neutrophils and reduced eosinophil counts. After PAF, FP enhanced transient neutropenia at 5 min and facilitated the recovery of oxygen tension in arterial blood (FP: 93±4 mmHg; P: 83±4 mmHg) at 45 min, without influencing the increases in Rrs.
In conclusion, the improvement of platelet-activated factor-induced oxygen tension in arterial blood disturbances after fluticasone proprionate suggests that inhaled glucocorticosteroids may possess vasoconstrictor properties in the pulmonary circulation.
- chronic airway diseases
- inflammatory mediators
- inhaled glucocorticosteroids
- neutrophil kinetics
- pulmonary gas exchange
This study was supported by Grant 99/0135 from the Fondo de Investigación Sanitaria (FIS) and the Comissionat per a Universitats i Recerca de la Generalitat de Catalunya (1999 SGR0228), and a grant-in-aid from GlaxoSmithKline (Research and Development, Greenford, Middlesex, UK and Madrid, Spain). A.A. Acuña was supported by Fundación Gran Mariscal de Ayacucho, Caracas, Venezuela and Instituto de Cooperación Iberoamericana (ICI), Spain. E.M. Uribe was supported by GlaxoSmithKline, Argentina.
Platelet-activating factor (PAF)-induced lung function abnormalities may be predominantly related to airway narrowing due to increased microvascular leakage 1–3. Like many other putative inflammatory mediators in the lung, PAF provokes vascular hyperaemia and/or engorgement, vasodilatation and increased vascular permeability within the airways, thereby facilitating exudation of protein-rich plasma and cells within and around the airway lumen 4, 5.
The predominant therapeutic site of inhaled glucocorticosteroids is in the airways. However, the potency of the topical glucocorticosteroids used for asthma is usually ranked by measuring local cutaneous vasoconstrictor effects when applied to the skin of healthy individuals 6. The clinical effects of glucocorticosteroids are mostly explained by their anti-inflammatory properties, which are time dependent. Beneficial short-term effects of inhaled glucocorticosteroids in asthma have recently been reported 7–9. High doses of inhaled flunisolide 7 and fluticasone 8 were superior to placebo (P) in the treatment of acute asthma in adults, and a vasoconstrictor effect of inhaled fluticasone propionate (FP) on bronchial blood flow has been demonstrated in mild intermittent asthmatics 9, 10. These effects may be enhanced by the increased vascularity of the bronchial wall, seen as part of the airway remodelling process in asthma 11, 12, and reduced by inhaled glucocorticosteroids 9, 10, 12.
The authors hypothesized that inhaled FP, a highly potent selective glucocorticosteroid with a low oral bioavailability 13, could prevent airway plasma leakage provoked by a laboratory-induced model of PAF challenge in patients with mild asthma, thereby leading to improvement in systemic, cellular, and lung function disturbances. Accordingly, the effects of a single high dose of inhaled FP on PAF-induced effects in patients with stable mild asthma were examined.
Methods
Study population
Twelve patients with stable mild intermittent asthma (table 1⇓) were recruited from the outpatient department of the Hospital Clínic of Barcelona, which was approved by the Ethics Research Committee of the centre. All patients received financial support for their participation in the study and gave informed written consent after the purpose, risks and potential benefits of the study were explained. The inclusion criteria were: forced expiratory volume in one second (FEV1) ≥80% of predicted (according to the authors' predicted equations 14) or ≥1.5 L; positive methacholine challenge (provocative dose causing a 20% fall in FEV1 (PD20) <1.9 µmol); positive PAF challenge, as shown by increases in respiratory system resistance (Rrs) ≥35% from baseline after PAF bronchoprovocation (18 µg), based on previous findings 1–3, 15, 16; absence of respiratory infection or exacerbation of asthma within the preceding 6 weeks; no previous regular treatment with oral corticosteroids; absence of any systemic or cardiopulmonary disease other than asthma. Maintenance therapy included short-acting β2-adrenergics with inhaled glucocorticosteroids (11 patients) and long-acting selective adrenergic agonists (one patient). All subjects were nonsmokers and atopic.
Patients characteristics and baseline lung function
Measurements
Blood samples were collected anaerobically through a catheter inserted into the radial artery. Arterial oxygen pressure (Pa,O2), carbon dioxide pressure (Pa,CO2) and pH were analysed in duplicate using standard electrodes and haemoglobin concentration was measured by a co-oximeter (Ciba Corning 860 System; Ciba Corning Diagnostics Corporation, Meadfield, MA, USA). Arterial blood gas measurements were not available in one patient.
Both minute ventilation and respiratory rate were measured using a calibrated Wright spirometer (Respirometer MK8; BOC-Medical, Essex, UK). The alveolar-arterial pressure gradient for oxygen (PA-a,O2) was calculated according to the alveolar gas equation assuming a standard respiratory exchange ratio (r=0.8). Total white cell counts in arterial blood were measured with a Technicon H.1TM System (Technicon, Tarytown, New York, NY, USA). The measurement of Rrs was performed using the forced oscillation technique and its analysis was restricted to 8 Hz 1–3. Three-lead electrocardiogram, heart rate (HR), systemic arterial pressure, and arterial oxygen saturation through a pulse oximeter (HP M1166A; Hewlett-Packard, Boblingen, Germany) were continuously recorded throughout the whole study (HP 7830A Monitor and HP 7754B Recorder, Hewlett-Packard, Waltham, MA, USA). Concentrations of urinary cysteinyl leukotriene E4 (uLTE4), corrected for urinary creatinine, were measured with a validated enzyme immunoassay (EIA) 17. uLTE4 determinations were not available in two patients.
Study design
A randomized, double-blinded, placebo-controlled, crossover design was used. All patients were challenged twice, 1 week apart, with PAF after the administration of either FP (6 mg, 12 puffs; GlaxoSmithKline, Madrid, Spain) or P (lactose), both given as dry powder from the Accuhaler® device (GlaxoSmithKline), while breathing room air. All asthma medication was with-held for 48 h before arrival to the laboratory on each study day. The evening before each study day, at 20:00 h, Rrs and forced spirometric recordings, venous blood sampling (available in six patients only) and urinary samples for LTE4 measurements were taken. Twelve hours after FP/P administration (08:00 h), all measurements, except urine collection, were repeated, with the addition of arterial blood sampling and ventilatory and haemodynamic recordings. Measurements of Rrs before PAF inhalation were carried out three times (every 0.5 h) over a 1.5 h period and averaged. Patients were then challenged with 18 µg PAF (1-0-Hexadecyl-2-acetyl-sn-glycero-3-phosphocholine; Novabiochem AG, Laufelfingen, Switzerland) 14 h after FP and vehicle administration, as previously reported 1–3. All sets of measurements were taken in duplicate immediately before and after PAF inhalation, in the following sequence: Rrs, arterial blood sampling, and ventilatory and haemodynamic recordings. One-hundred and twenty minutes after PAF, urine was collected again for LTE4 measurements. All patients tolerated the challenges without major problems.
Statistical analysis
Results were expressed as mean±sem or 95% confidence intervals (CI). Changes before (20:00 versus 08:00 h) and after PAF challenge were separately assessed by a two-way repeated measure analysis of variance (ANOVA). Baseline values for PAF challenge were those obtained in the mornings. This model was considered appropriate to the two-period, two-treatment, crossover design used to determine the effect of FP compared with P and allowed for intrasubject comparisons at each time point, as previously shown 15, 16. Newman-Keuls multiple range tests were used to determine the significance of paired isotopic variables between FP and P at each time point. Statistical significance was set at p<0.05.
Results
Effects of fluticasone before platelet-activating factor
Table 1⇑ shows the characteristics and baseline functional measurements of all patients and table 2⇓ includes lung function and haemodynamic findings, peripheral cell counts and uLTE4 concentrations before and after FP and vehicle administration. Compared with P, the inhalation of FP provoked an improvement in airway calibre, as assessed by mild favourable changes in FEV1, either expressed as absolute values (p<0.04) or % pred (p<0.003), and Rrs (p<0.008) (fig. 1⇓ and table 2⇓). Likewise, inhaled FP increased peripheral blood neutrophils (p<0.004) but reduced eosinophil counts (p<0.008), without inducing changes in the concentrations of uLTE4 (table 2⇓). The functional and cellular findings during P administration may be ascribed to the circadian rhythm. There were no differences in ventilatory, haemodynamic, and gas exchange indices between the morning set points after each pre-treatment.

Changes in the individual values of resistance of respiratory system (Rrs) (a and b) and forced expiratory volume in one second (FEV1) (c and d) after placebo (○) and fluticasone propionate (•) pretreatment before platelet-activating factor challenge. —: mean values. p<0.008 comparing Rrs and p<0.04 comparing FEV1 between placebo and fluticasone groups.
Changes between placebo and fluticasone propionate before platlet-activating factor challenge
Effects of platelet-activating factor after vehicle
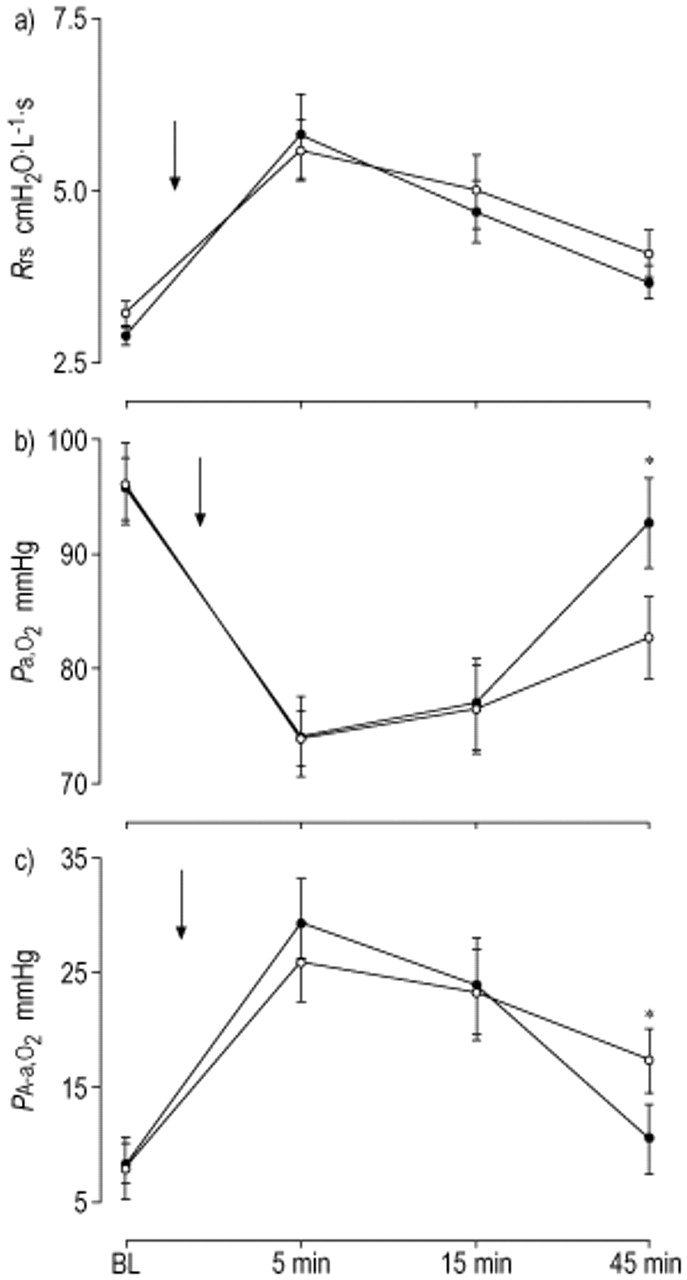
Effects of PAF after vehicle are shown in table 3⇓ and figure 2⇓. Ten patients noticed facial flushing, 11 felt shortness of breath, and six coughed immediately after PAF challenge. Five min after PAF, Rrs increased by 73% (from 3.23±0.18 to 5.60±0.45 cmH2O·L−1·s, p<0.01), Pa,O2 decreased by 23% (from 96±4 to 74±2 mmHg), PA-a,O2 increased (from 8±3 to 26±3 mmHg, p<0.001), and peripheral blood neutrophils decreased (from 2.76±0.30 to 1.66±0.36×109 L−1, p<0.01). This neutropenia was followed by a rebound neutrophilia at 15 and 45 min (4.47±0.58 and 4.82±0.69×109 L−1, respectively, p<0.05). Both ventilatory and haemodynamic variables and Pa,CO2 and arterial pH remained unchanged.

The time course of resistance of a) the respiratory system (Rrs), b) oxygen tension in arterial blood (Pa,O2) and c) the alveolar-arterial oxygen pressure gradient (PA-a,O2) at baseline (BL) and at 5, 15, and 45 min after inhaled platelet-activating factor (PAF). ○: pretreatment with placebo; •: pretreatment with flucticasone propionate; arrows: PAF challenge. *: p<0.05 between placebo and fluticasone propionate.
Changes induced by platlet-activating factor after placebo (P) and fluticasone propionate (FP) pretreatments
Effects of platelet-activating factor after fluticasone propionate
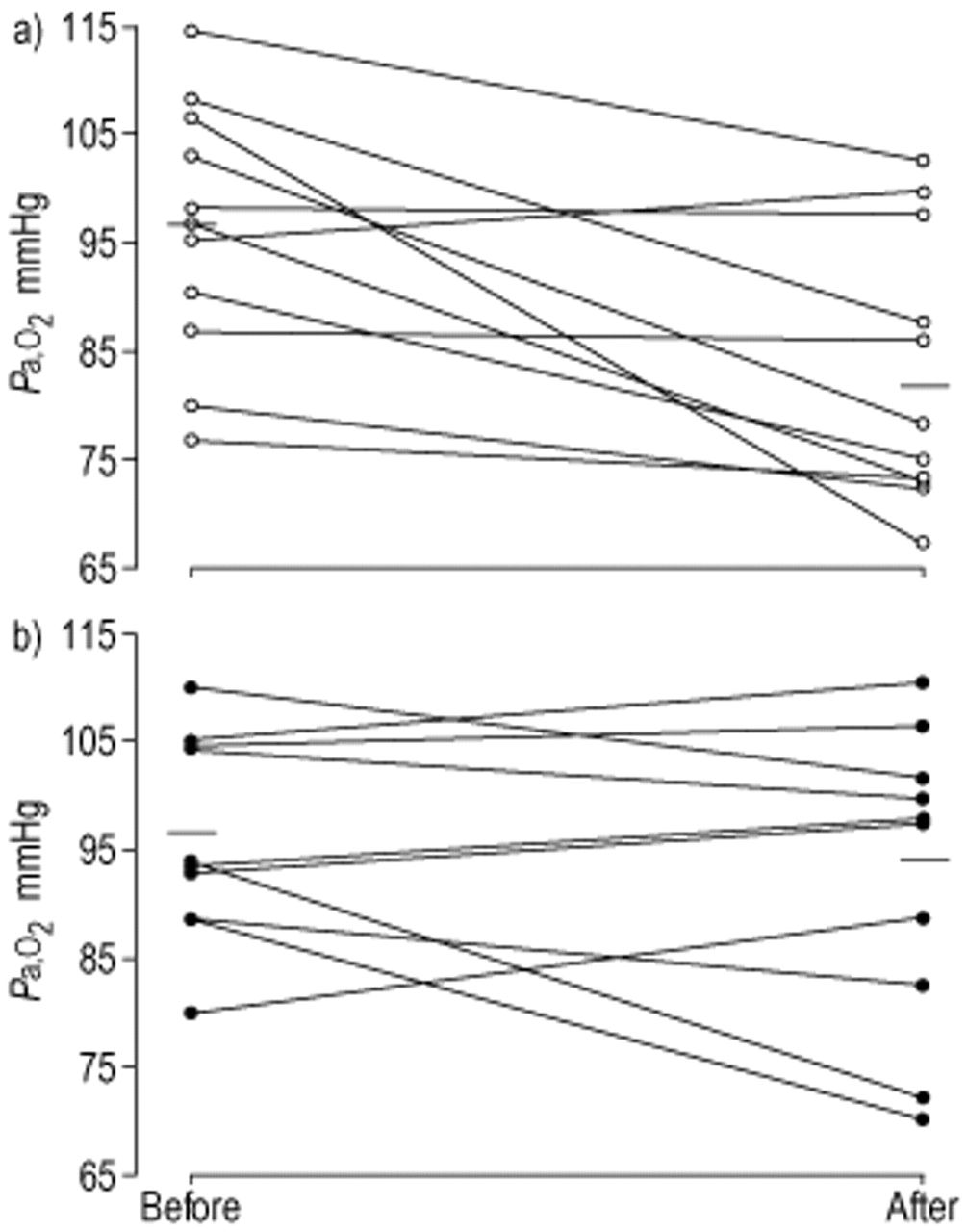
Effects of PAF after FP are shown in table 3⇑ and figure 2⇑. Pretreatment with FP did not modify or abolish PAF-induced systemic effects: 10 patients noticed facial flushing, 11 shortness of breath, and three cough. Inhaled FP, as compared with vehicle, enhanced the PAF-induced decrease in circulating neutrophils at 5 min (from 3.93±0.40 to 1.71±0.43×109 L−1; FP −57%; P -40%; p<0.05), whereas the rebound neutrophilia observed at 15 and 45 min (5.20±0.61 and 5.56±0.67×109 L−1, respectively) did not differ from that shown after P. Moreover, FP inhalation exhibited modest but significantly greater Pa,O2 (FP 93±4 mmHg; P 83±4 mmHg; p<0.01) (fig. 3⇓) and lower PA-a,O2 (FP 11±3 mmHg; P 18±3 mmHg; p<0.02) values at 45 min, as compared with P. Compared to baseline (±1 mmHg) (fig. 3⇓), mean Pa,O2 after P was reduced in eight patients (−18.3±4.3 mmHg), was similar in two patients (−0.9 mmHg), and increased in the remaining patient (4.4 mmHg). Conversely, Pa,O2 after FP was reduced in five patients (−11.7±5.9 mmHg) and increased in the other six (5.0±0.9 mmHg). Remarkably, there were no differences in the increases in Rrs after PAF between the two interventions. The significant increase in uLTE4 concentration observed after PAF inhalation in the FP arm (from 355±104 to 1,608±352 pg·mg−1) was not different from that measured after P (from 305±34 to 1,421±401 pg·mg−1, p<0.0001).

{kind=link}
{kind=link}
{kind=link}
Individual changes in oxygen tension in arterial blood (Pa,O2) after placebo (○) and fluticasone propionate (•), before (and after each pretreatment) and 45 min after platelet-activating factor challenge. —: mean values. p<0.01 comparing placebo and fluticasone.
Discussion
In this study, three main effects of administration of a single high dose of inhaled FP in patients with mild intermittent asthma were observed. Firstly, FP to some degree prevented the diurnal fall in bronchial tone. Secondly, immediately after PAF challenge, there was a more pronounced reduction in circulating neutrophils without differences in the subsequent rebound neutrophilia. Finally, FP attenuated gas-exchange defects by the end of PAF challenge, as shown by a greater recovery of arterial oxygenation, without modifying the bronchoconstrictor response.
In this study, the effects of FP 12 h after inhalation were investigated following a previous preliminary study that examined the inhalation of low-to-high doses of budesonide (≤1,600 µg) in patients with mild asthma 18. In the study by Le Merre et al. 18, the inhaled glucocorticosteroid improved lung function maximally at 12–14 h. In addition, the authors own preliminary studies, including inert gas measurements, showed no effects of FP when studied at 2 h, using 2 and 6 mg, and 6 h, using 6 mg (data not shown). There is evidence of diurnal variation in FP pharmacokinetics, with higher than expected plasma drug concentrations in the morning than in the evening 19. In this study, a high dose of FP (6 mg) was used, which was likely to contribute to systemic levels. Challenge with PAF, a mediator that may be involved in the pathogenesis of asthma, causes moderate-to-severe gas exchange deterioration 1–3, 20, similar to that seen in spontaneously-occurring acute asthma. This indicates that the principal mechanism of PAF-induced arterial hypoxaemia, i.e. ventilation perfusion inequalities, could result more from increased vascular permeability than from bronchoconstriction per se 2, 20.
The authors suggest that the three principal effects of FP observed in the current study may be related to the pharmacological properties of inhaled glucocorticosteroids.
Firstly, the bronchodilator effect before PAF challenge could be due to the anti-inflammatory effects of the drug exerted on the bronchial mucosa, although a vasoconstrictor effect on bronchial blood flow cannot be disregarded (see later) 9, 10.
Secondly, FP enhanced the peripheral neutropenia usually caused by PAF. The authors surmize that FP before PAF facilitated the release of neutrophils from the bone marrow and that these new neutrophils might be less mature and more rigid, i.e. less deformable, and possibly larger than neutrophils that have been circulating. All other things being equal, this would favour a more pronounced retention in the lung after PAF challenge 21, 22. Inhaled PAF provokes considerable airway neutrophilia in asthmatics 21, 23 and neutrophilic airway inflammation has been shown to be predominant in persistent asthma 24. However, glucocorticosteroids do not reduce neutrophilic airway disease inflammation 25 and airway neutrophilia could even persist through glucocorticosteroid-induced inhibition of neutrophil apoptosis 26. Thus, FP is unlikely to modulate the PAF-induced airway response mediated in part by the release of leukotrienes 15.
Thirdly, the authors hypothesize that the late PAF-induced pulmonary gas exchange amelioration in the FP arm may reflect a predominant vasoconstrictor effect on the pulmonary circulation, possibly facilitating a better alveolar ventilation to pulmonary blood flow balance. As shown in previous studies with other interventions 2, 15, 16, the lack of an earlier beneficial Pa,O2 response after PAF may be due to the intense severity of lung function abnormalities at the nadir of the challenge, not offset by the high doses of FP given. It has been convincingly shown that ventilation perfusion mismatch instantly caused by PAF, steadily recovers as the effects of PAF vanish, with a trend toward baseline values by 45 min 1–3, 15, 16. The latter finding is at variance with the attenuation of arterial hypoxaemia shown at the end of this study in the FP arm. By contrast, PAF-induced systemic effects and increases in both Rrs and uLTE4 concentrations were not affected throughout the study period, without differences between the two interventions. These negative findings may indicate that FP could not exert a beneficial effect against PAF-induced airway inflammation, which can be mediated, at least in part, by an ongoing endogenous release of leukotrienes 15. However, complementary bronchial vasoconstriction cannot be overlooked 9, 10, as the methodology used for the assessment of PAF-induced increases in total Rrs may be less sensitive than gas exchange measurements in detecting an effect on airway vasculature.
The proposed mechanisms of inhaled glucocorticosteroids include upregulation of selective β-adrenergic receptors, vasoconstriction of the mucosa and decreased wall oedema within the airway 27. However, the rapid onset of the clinical response in some of these clinical studies 7, 9 would indicate that some beneficial effects of glucocorticosteroids may occur very rapidly, while other effects may occur very slowly, requiring a minimum of 6–12 h after medication 28. McFadden 29 postulated that the effects of flunisolide in patients with acute asthma 7 could result from a nonspecific generic phenomenon common to topical steroids, thereby causing substantial vasoconstriction in the larger airways and modifying, at least in part, some of the pathophysiological components of airway narrowing in bronchial asthma. A transient short-term vasoconstrictor effect in the airway mucosa has recently been demonstrated in mild intermittent asthmatics, after moderate-to-high doses of inhaled FP 9 and after a 2-week course of moderate doses of FP 10. Glucocorticoid-induced bronchial vasoconstriction could be related to noradrenaline uptake inhibition by nonneuronal cells, that may facilitate increased noradrenaline concentration at α-adrenergic receptors 30.
However, the precise pathogenic mechanism through which inhaled glucocorticosteroids cause bronchial vasoconstriction remains to be elucidated. It has been postulated that this vascular response may reflect a nongenomic mode of action 9, 27 related to stimulation of noradrenergic neurotransmission. However, glucocorticosteroids do not exhibit direct noradrenergic properties. Airway mucosal blood flow is increased in stable asthmatics 9, 10, 12, 31. These observations indicate that inhaled glucocorticosteroids, especially at higher doses, may downregulate airway wall vascularity 12 and restore downregulation of β-adrenergic agonist-mediated response in patients with asthma 9, 10, hence reflecting their anti-inflammatory properties 10, 12.
In conclusion, the authors have shown that a single administration of a high dose of inhaled fluticasone propionate facilitates a better recovery of decreased oxygen tension in arterial blood in a laboratory-induced model of bronchoconstriction caused by platelet-activating factor in mild asthmatics. High doses of this inhaled glucocorticosteroid may attenuate gas exchange defects provoked by platelet-activating factor, by inducing a vasoconstrictor effect within the pulmonary circulation, similar to that shown with a lower dose of fluticasone propionate in the bronchial blood flow compartment. Even though there is an effect of fluticasone propionate on wall oedema and/or bronchial vascular engorgement in peripheral airways with or without redistribution of platelet-activating factor, deposition within the airways cannot be overlooked.
- Received August 3, 2001.
- Accepted December 10, 2001.
- © ERS Journals Ltd
References









