





Abstract
Inhaled short-acting β2‐agonists provide greater protection against airway responsiveness (AR) to the mast-cell stimulus, adenosine 5′‐monophosphate (AMP), than to histamine, a direct spasmogen. Both terbutaline and albuterol exhibit this mast-cell stabilizing property in a dose-dependent manner. A single dose of the long-acting β2‐agonist formoterol has also been reported to have a mast cell-stabilizing effect, whereas salmeterol has not. To explore the dose-related actions of the long-acting β2‐agonist formoterol on AR, the authors compared the acute effects of three doses of formoterol and terbutaline on AR to AMP and histamine.
In a double-blind, randomized, placebo-controlled, cross-over study, 25 mild, steroid naive, asthmatic subjects attended on 10 occasions. At each visit, subjects inhaled either a single dose of terbutaline (500 µg), formoterol (6, 12 or 24 µg) or a matched placebo, administered via Turbuhaler®, 30 min prior to challenge with both AMP and histamine.
Each dose of β2‐agonist reduced AR to AMP and histamine. The bronchoprotective effects of formoterol (6 µg) and terbutaline (500 µg) were similar in magnitude in reducing AR to histamine (mean±sd: 3.6±0.3 and 3.1±0.3 doubling doses (DD)) and AR to AMP (3.5±0.5 and 3.3±0.4 DD, respectively). Overall, formoterol reduced AR to both spasmogens in a dose-dependent manner. In addition, formoterol (12 and 24 µg) provided a significantly greater protective effect against AMP than against histamine challenge. It decreased AR by 5.7±0.6 and 6.3±0.7 DD against AMP and 4.3±0.4 and 4.8±0.43 DD against histamine, respectively.
The results of this study indirectly demonstrated an in vivo dose-dependent mast-cell stabilizing effect of formoterol, in addition to functional antagonism on airway smooth muscle. This property of β2‐agonists may have clinical benefits in asthma management.
The long-acting β2‐agonists formoterol and salmeterol are effective bronchodilators with a much longer duration of action than the short-acting β2‐agonists albuterol and terbutaline 1. Their addition to low-dose inhaled glucocorticosteroids (GCS) is now recommended as an alternative to the use of high-dose inhaled corticosteroids in asthma management, especially in patients with nocturnal asthma or exercise-induced symptoms 2. In a similar manner to short-acting β2‐agonists, a single dose of formoterol may have a greater bronchoprotective effect on the indirect spasmogen, adenosine 5′‐monophosphate (AMP), than on the direct-acting spasmogen, histamine 3–5. In vitro and in vivo evidence of mast-cell mediator release and the attenuation of the bronchoconstrictive effects of AMP by the cromones and antihistamines suggest that AMP acts primarily as a mast-cell stimulus 6–8. This implies an in vivo mast-cell stabilizing effect of formoterol, in addition to functional antagonism on airway smooth muscle, an observation which, to date, has not been demonstrated with salmeterol 9, 10.
To further evaluate the in vivo mechanisms of formoterol, the effects of a single dose of formoterol (6, 12 and 24 µg), terbutaline 500 µg (control) and a placebo on both AMP and histamine challenges were investigated. The authors aimed to prove that formoterol produced a dose-related reduction in airway responsiveness (AR). It was hypothesized that formoterol would provide greater, dose-dependent bronchoprotection against the mast-cell stimulus AMP, than against the direct histamine stimulus.
Methods
Subjects
Twenty-five nonsmoking subjects (12 males and 13 females) aged 23–42 yrs, took part in this study. All subjects had had mild asthma (forced expiratory volume in one second (FEV1) >70% predicted), a positive skin-prick test to common airborne allergens (Dermatophagoides pteronyssinus, mixed grass pollen, or cat fur), a documented sensitivity to histamine (geometric provocative concentration causing a 20% fall in FEV1 (PC20) <2 mg·mL−1) and AMP (geometric PC20 <25 mg·mL−1) during the previous 4 weeks. No subjects had an exacerbation of asthma or respiratory infection in the preceding 6 weeks. Each subject had infrequent symptoms, controlled with occasional inhaled short-acting β2‐agonists alone. No subject was taking any regular anti-asthma therapy and none had taken inhaled corticosteroids for at least 3 months prior to entry. Written informed consent was obtained from each subject and the study was approved by the Ethics Committee of King's College Hospital.
Study design
It was a double-blind, placebo-controlled, cross-over study and consisted of 10 treatment visits 3–7 days apart. Each subject received either terbutaline (500 µg), formoterol (6 µg), formoterol (one inhalation of 12 µg), formoterol (24 µg, two inhalations of 12 µg) or a placebo at each visit, followed by either histamine or AMP challenge. Treatments were randomized using a Latin-square design. The order of the challenge was also randomized and subjects were blinded to the spasmogen delivered. Subjects received each treatment twice, once prior to histamine, the other before AMP challenge. Following baseline FEV1 (performed by an independent observer), subjects inhaled one actuation from each of three individual Turbuhalers® (Astra Draco AB, Lund, Sweden). At each visit, subjects were instructed in the correct use of the Turbuhaler® by an experienced Asthma Nurse Specialist to ensure they had the correct inhalation technique, flow rate and inspiratory hold time. Two inhalers were identical in appearance and contained 6‐µg formoterol, 12‐µg formoterol or matched placebo and the other contained 500-µg terbutaline or a matched placebo. Thirty minutes later, spirometry was repeated by a second operator, blinded to initial FEV1, and subjects were then challenged with either histamine or AMP. Subjects refrained from using rescue medication and caffeinated beverages for ≥8 h prior to each visit and attended the laboratory at the same time each morning.
Bronchial provocation and pulmonary function measurement
Fresh solutions of histamine (Northwick Park and St Marks Hospitals, Harrow, UK) and AMP (Sigma, Poole, UK) were made up in 0.9% saline in concentrations from 0.0625–32 mg·mL−1 for histamine and 0.39–800 mg·mL−1 for AMP. Each solution was administered from a nebulizer attached to a breath-activated dosimeter (Mefar, Brescia, Italy). The nebulizer delivered particles with an aerodynamic mass median diameter of 3.5–4 µM at a mean output of 9 µL·breath−1.
Pulmonary function was assessed by measurement of FEV1 using a dry-wedge spirometer (Vitalograph, Buckingham, UK). A standard challenge protocol was used for all provocation tests. Following a 15-min rest period, subjects performed three measurements of FEV1, 1 min apart, the best of which was taken as baseline. Subjects then inhaled five breaths of saline as a control, with an inhalation time of 1 s and breath-hold time of 6 s. Providing FEV1 remained within 10% of the baseline, subjects continued by inhaling five breaths of doubling concentrations of spasmogen at 3‐min intervals. FEV1 was measured at 1.5- and 2.5-min intervals following each challenge, and the highest value was recorded for analysis. Challenges were terminated when a ≥20% fall in FEV1 from postsaline was recorded or the maximum concentration had been given. A logarithmic concentration/response curve was constructed and the PC20 calculated by linear interpolation. If a 20% fall in FEV1 was not achieved after inhalation of the final concentration of spasmogen, the PC20 was estimated by applying the actual fall in FEV1 to the slope of the log concentration/response curve obtained at screening and a value obtained by linear extrapolation. The assumption that this dose/response curve did not change in the presence of β2‐agonist was made.
Statistical methods
Results are presented as mean±sem, unless otherwise stated. Serial measurements within groups (baseline FEV1, change from baseline following treatment) were analysed by repeated-measures analysis of variance (ANOVA) and the difference between means was analysed using a paired t‐test with Bonferroni's correction. PC20 values following inhalation of active and placebo treatments on each study day were logarithmically transformed for analysis, and the protective effect on each challenge was calculated using the formula: The results are expressed in terms of doubling dose (DD), mean±sem.
The results are expressed in terms of doubling dose (DD), mean±sem.
The protective effects (log10 active−log10 placebo) of the different β2‐agonist doses were analysed using two-way factorial analysis with repeated measures. Differences between means were analysed using an unpaired t‐test with a Bonferroni's correction.
FEV1 values, following inhalation of the final four concentrations of spasmogen for each treatment (where a PC20 was achieved), were calculated as a percentage of the postsaline value (expressed as mean±sem) and concentration/response curves were constructed and compared using one-way repeated ANOVA.
Using individual subject data, linear regression analysis of the log active–log placebo for each β2‐agonist dose was used to determine the dose-dependency of the bronchoprotective response. A p‐value <0.05 was considered to be statistically significant.
Results
After screening, all 25 randomized subjects (mean age 26.6±0.7 yrs), completed the study. The mean screening PC20 of spasmogen was 0.3±1.1 mg·mL−1 and 3.55±1.2 mg·mL−1 for histamine and AMP, respectively.
Bronchodilation
Mean baseline FEV1 was 91±2% pred, with no significant differences between visits. There was a significant increase in baseline FEV1 30-min postinhalation of a single dose of formoterol (6, 12 and 24 µg) and terbutaline (500 µg) relative to placebo (p<0.0002), prior to histamine and AMP challenges on each study day. Although there was a trend towards a dose-dependent increase in FEV1 following formoterol, this did not achieve significance (table 1⇓).
Airway calibre measured as forced expiratory volume in one second at baseline and 30 min after treatment prior to challenge with histamine and adenosine 5′-monophosphate (AMP)
Bronchoprotection against histamine and adenosine 5′‐monophosphate
Following formoterol (24 µg), 11 subjects failed to achieve PC20 after inhalation of the final concentration of AMP (800 mg·mL−1). Following 12-µg formoterol, nine subjects failed to achieve PC20, whereas one and two subjects failed to achieve PC20 after 6‐µg formoterol and 500-µg terbutaline, respectively. Following challenge with the highest concentration of histamine (32 mg·mL−1), only one subject failed to achieve PC20 and this was after inhalation of 12-µg formoterol.
The log PC20 for histamine and AMP challenge following placebo and β2‐agonist are presented in table 2⇓. Formoterol induced dose-dependent bronchoprotection against both AMP (p=0.001) and histamine (p=0.033).
Bronchoprotective effect of formoterol and terbutaline on airway responsiveness to histamine and adenosine 5′‐monophosphate (AMP)
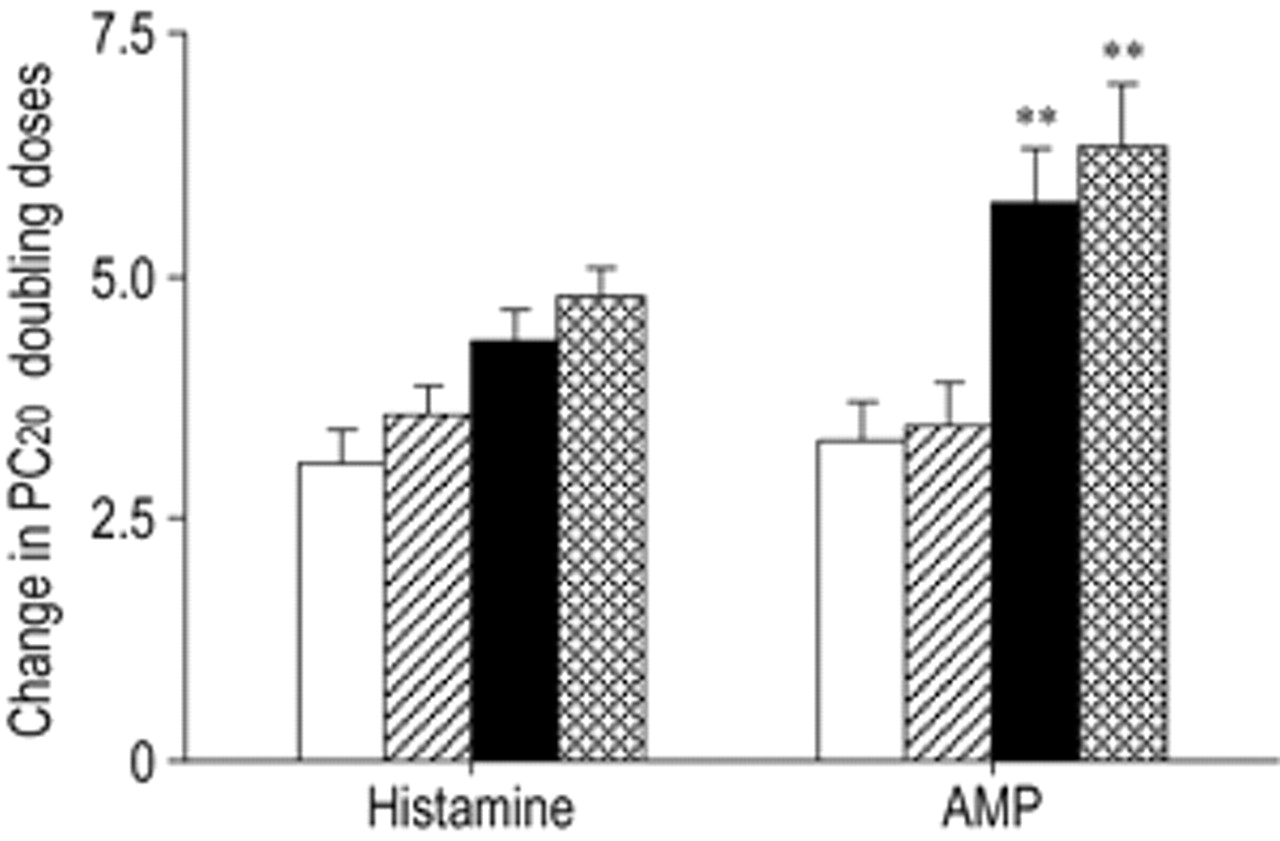
Analysis of the log active−log placebo data revealed that the β2‐agonist provided significant bronchoprotection against spasmogen (F(3,72)=34.9, p<0.01). However, the bronchoprotection provided by the β2‐agonist was dependent upon the stimulus used, as reflected by a significant interaction (F(3,72)=4.53, p≤0.01). The bronchoprotective effect of 12-µg formoterol was significantly greater against AMP (5.7±0.6 DD) than against histamine (4.3±0.4 DD) (p<0.01). Bronchoprotection following 24-µg formoterol was also significantly greater against AMP (6.3±0.7 DD) than against histamine (4.8±0.43 DD) (p<0.01). In contrast, there was no significant difference between the bronchoprotective effect of inhaled formoterol at a dose of 6 µg against AMP (3.5±0.5 DD) and histamine (3.6±0.3 DD) or following inhaled terbutaline 500 µg against AMP (3.3±0.4 DD) and histamine (3.1±0.3 DD) (fig. 1⇓).

Doubling dose bronchoprotection of formoterol (└: 6 µg; ▪: 12 µg;  : 24 µg) and terbutaline (□: 500 µg) relative to the placebo on airway responsiveness, 30 min before challenge with histamine and adenosine 5′‐monophosphate (AMP). PC20: Provocative concentration of spasmogen causing a 20% fall in the forced expiratory volume in one second. Results are presented as means±sem. **: p<0.01, AMP versus histamine.
: 24 µg) and terbutaline (□: 500 µg) relative to the placebo on airway responsiveness, 30 min before challenge with histamine and adenosine 5′‐monophosphate (AMP). PC20: Provocative concentration of spasmogen causing a 20% fall in the forced expiratory volume in one second. Results are presented as means±sem. **: p<0.01, AMP versus histamine.
Dose/response curves
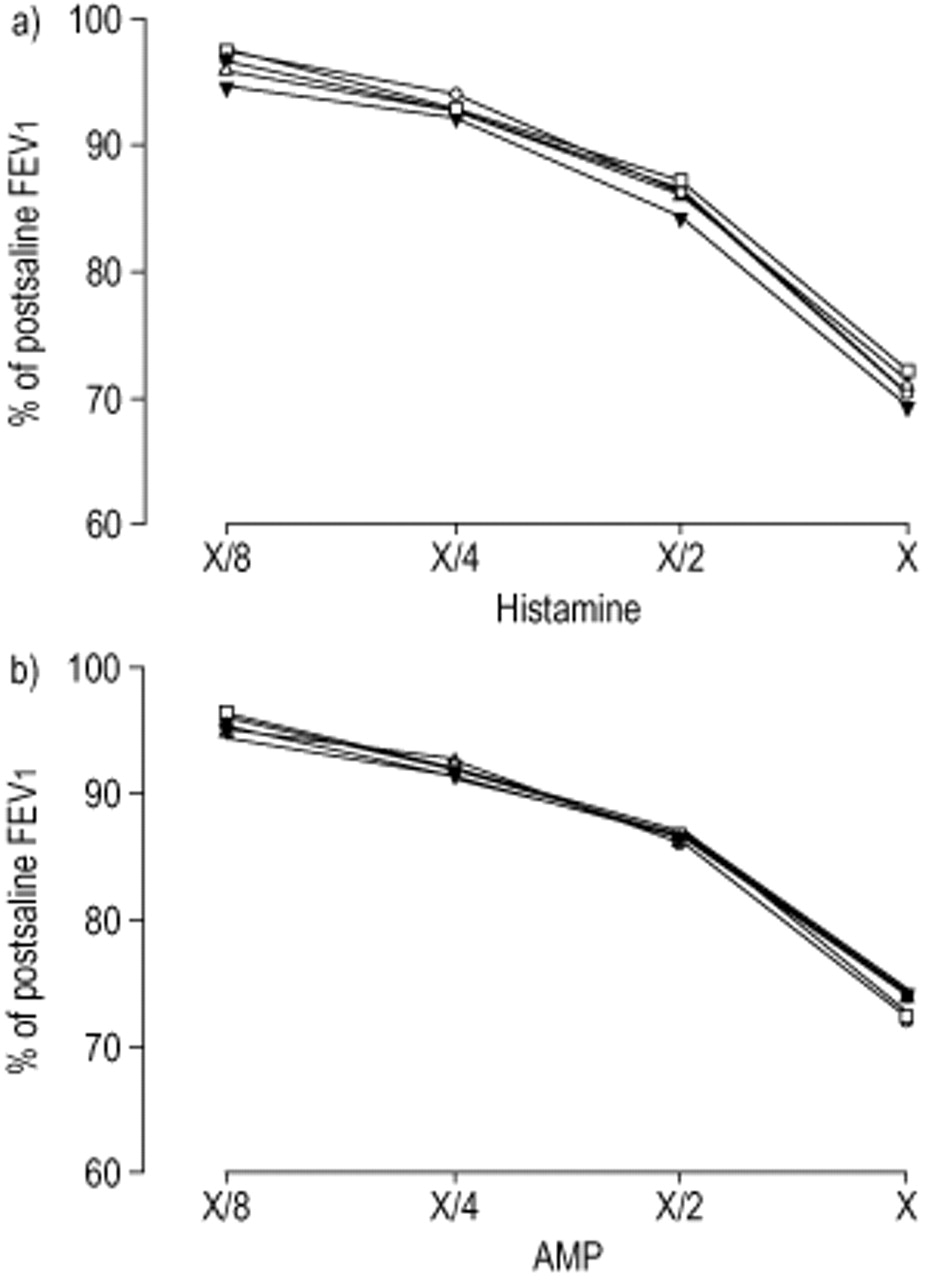
The dose/response curves for AMP and histamine were similar in slope after inhalation of placebo and were not significantly altered by either terbutaline (500 µg) or formoterol (6, 12 or 24 µg) (fig. 2⇓).
{kind=link}
{kind=link}
Dose/response curves for each spasmogen, a) histamine and b) adenosine 5′‐monophosphate (AMP), following inhalation of placebo (□), formoterol (•: 6 µg; ▵: 12 µg; ▴: 24 µg) and terbutaline (○: 500 µg). Measured by forced expiratory volume in one second (FEV1) values (expressed as a percentage of the postsaline value), following the final four doubling doses of spasmogen in those subjects achieving a provocative concentration of spasmogen causing a 20% fall in FEV1.
Discussion
The results of this study demonstrate the bronchodilator and bronchoprotective effects of acute administration of both the short-acting β2‐agonist terbutaline and the long-acting β2‐agonist formoterol. A significant improvement in FEV1 30 min after each active treatment and a dose-dependent reduction in AR to both AMP and histamine following formoterol was observed. The two higher doses of formoterol produced a greater bronchoprotective effect against AMP compared to that against histamine, whereas 6‐µg formoterol and 500-µg terbutaline reduced AR to both spasmogens to a similar extent.
The similarity between AMP and histamine dose/response curves following placebo and each active treatment allows direct comparison of the bronchoprotection against each spasmogen. Thus, to explain the findings, it is likely that there are additional mechanisms to β2‐agonist-mediated functional antagonism against induced airway smooth muscle contraction. The greater degree of bronchoprotection against AMP afforded by formoterol compared with histamine, is consistent with previous studies on the differential effects of short-acting β2‐agonists on AR to these spasmogens 3. This effect has been previously reported 30 min after a single dose of formoterol (12 µg) 5 but not 2 or 14 h after a single dose of salmeterol (50 µg) 9, 10.
Both short- and long-acting β2‐agonists inhibit mast mediator release in vitro 11–13. As the major bronchoconstrictive effect of AMP results from mast-cell degranulation and mediator release 6–8, the additional bronchoprotection seen with the higher doses of formoterol is likely to be due to its mast-cell stabilizing properties. The difference between the in vivo effect of formoterol and salmeterol is surprising as they have similar effects on mast cells in vitro 11–13. The differences in the pharmacological properties of salmeterol and formoterol may provide an explanation for the lack of an additional effect of a single dose of salmeterol (50 µg), against AMP in previous studies 9, 10. Salmeterol, a partial agonist, may simply not achieve adequate levels of receptor occupancy on mast cells at this dose. Indeed, salmeterol is two-fold less potent than formoterol in relaxing human smooth muscle in vitro and is ≥20-fold less active than formoterol at inhibiting mast-cell degranulation 11.
An alternative explanation for the additional bronchoprotective effect of formoterol must be considered. In addition to its effect on mast-cell degranulation and mediator release, adenosine, the active metabolite of AMP, may have direct effects on mucosal blood flow, microvascular leakage and contractile neuropeptide release from sensory nerve endings via A2b receptors 14–16. Since formoterol inhibits plasma exudation on postcapillary venule cells and neuropeptide release from sensory nerves 17 via β2‐receptors, it is plausible that some of its nonsmooth muscle effects involve pathways that are independent of its mast-cell stabilizing properties.
As the authors had shown an additional bronchoprotective effect of 500-µg terbutaline against AMP in two previous studies 3, 18, they were surprised that there was no significant difference between the bronchoprotective effect of the same doses of terbutaline against histamine and AMP in the present study. The possibility that the bronchoprotective effect of terbutaline had worn off at the time of completion of AMP challenge was considered. The maximum possible time between inhalation of treatment and the completion of each challenge was 63 min for histamine and 69 min for AMP (30 min before the start of challenge and ≤39 min to administer all doses of spasmogen). Mean times (95% confidence intervals) for completion of histamine and AMP challenges were 53.6 min (50.3–54.9) and 58.9 min (56.1–61.7), respectively. Short-acting β2‐agonists protected against histamine for ≤4 h with a peak of between 1–2 h 19, 20 and 500-µg terbutaline protected against exercise-induced asthma for ≤2 h 21. It is unlikely, therefore, that the timing of the challenges could explain the results.
The 3.1 DD bronchoprotection against histamine was greater than the 2.1 and 2.7 previously reported by the authors and the DD protection following the same dose of terbutaline against methacholine 3, 18. The geometric mean PC20 to histamine of 0.28 mg·mL−1 after placebo was much lower than in a previous study by the authors, in which the values after placebo were 1.04 and 0.91 mg·mL−1. It is possible that the acute effect of terbutaline on histamine is greater in subjects with more severe AR. There was no other difference in subject characteristics and the same inhaler device was used in each of the studies.
Higher doses of the short-acting partial agonist albuterol (400 µg via Diskhaler) 9 and albuterol (2.5 mg nebulized) 4 provided greater bronchoprotection to AMP than histamine, a finding not seen at the lower dose of albuterol, 200 µg via Turbuhaler® 5. The authors have also previously demonstrated dose-dependent additional bronchoprotection of terbutaline against AMP relative to methacholine 3. Therefore, the lack of additional bronchoprotection following 6‐µg formoterol or 500-µg terbutaline in this study provides further evidence that the presumed mast-cell stabilizing effects of β2‐agonists are dose-dependent.
The failure of a number of subjects to achieve a PC20 to AMP following treatment with formoterol may have led to an underestimation of the bronchoprotective effect against AMP. The highest dose of AMP available for inhalation was 800 mg·mL−1, and a PC20 was not achieved in 11 of the 25 subjects after 24-µg formoterol, in nine subjects after 12-µg formoterol and in one subject after 6‐µg formoterol. To overcome this and to obtain an estimate of the true PC20 for these subjects, the slope of the screening AMP concentration/ response curve was utilized. By fitting the maximum per cent FEV1 fall achieved following 800 mg·mL−1 of AMP to that slope, the log PC20 by linear extrapolation was determined. This assumed that β2‐agonist treatment did not alter the slope of the AMP dose/response curve. The parallel shift in dose/response curves after each treatment in subjects achieving a PC20 suggested that the authors' assumption was correct (fig. 2⇑). Therefore, the failure of a number of subjects to achieve PC20 at the highest concentration of AMP was unlikely to have significantly influenced the true bronchoprotective effect of formoterol (12 and 24 µg).
The clinical relevance of the additional bronchoprotective effect of a single dose of formoterol against AMP compared to histamine remains uncertain. Long-acting β2‐agonists are not used as monotherapy but only in conjunction with inhaled GCS 2. Therefore, any mast-cell effects of long-acting β2‐agonists would be in addition to the known ability of inhaled corticosteroids to deplete airway mast-cell numbers 22, 23. However, inhaled corticosteroids do not fully protect against allergen- or exercise-induced bronchospasm, which are both regarded as mast-cell mediated events 23, 24. This suggests that even in the presence of inhaled corticosteroids there are potentially active mast cells residing in the airways and it is possible that β2‐agonists would confer additional benefit. The addition of formoterol to inhaled budesonide improves symptoms and lung function and reduces asthma exacerbations over a 12-month period 25. Furthermore, recent evidence from Tattersfield et al. 26 suggested that as-needed treatment with formoterol provided better asthma control than terbutaline in patients requiring moderate doses of relief medication, despite inhaled GCS treatment. Although this additional benefit of formoterol requires further explanation, it is probably due to a nonbronchodilator action that may involve modulation of the inflammatory process.
This study clearly shows a nonsmooth muscle action of formoterol, which the authors believe is due to an effect on the mast cells. This dose-dependent mast-cell stabilizing effect occurs 30-min after a single dose of formoterol. The rapid onset of both the bronchodilator and bronchoprotective effects of therapeutic doses of formoterol may have a beneficial effect against mast-cell stimuli, such as inhalation of allergen and exercise, in addition to functional antagonism on bronchial smooth muscle. These benefits may account for the improvement seen in asthma control with the combination of long-acting β2‐agonist and inhaled glucocorticosteroids. Further study of the mechanisms governing the action of formoterol and related molecules is required.
- Received March 14, 2001.
- Accepted November 9, 2001.
- © ERS Journals Ltd
References









