





Abstract
Interventional Radiology is a technique based medical specialty, using all available imaging modalities (fluoroscopy, ultrasound, computed tomography, magnetic resonance, angiography) for guidance of interventional techniques for diagnostic or therapeutic purposes.
Actual, percutaneous transthoracic needle biopsy includes core needle biopsy besides fine needle aspiration. Any pleural, pulmonary or mediastinal fluid or gas collection is amenable to percutaneous pulmonary catheter drainage.
Treatment of haemoptysis of the bronchial artery or pulmonary artery origin, transcatheter embolization of pulmonary arteriovenous malformations and pseudoaneurysms, angioplasty and stenting of the superior vena caval system and percutaneous foreign body retrieval are well established routine procedures, precluding unnecessary surgery. These techniques are safe and effective in experienced hands.
Computed tomography is helpful in pre- and postoperative imaging of patients being considered for endobronchial stenting. Many procedures can be performed on an outpatient basis, thus increasing the cost-effectiveness of radiologically guided interventions in the thorax.
Percutaneous nonoperative procedures in the chest were applied before the advent of imaging. Leyden 1 performed the first transthoracic needle lung biopsy in 1882 to confirm pulmonary infection. During the first half of the twentieth century, lung biopsy was mainly used to establish the microbiological diagnosis of extensive infectious lobar consolidation, which was easy to localize. Percutaneous needle sampling in the chest however, fell into disrepute, due to an unacceptable high rate of complications, caused by the large calibre of needles. Despite the use of smaller needles, pathologists remained reluctant to formulate a diagnosis on small samples or smears. Fluoroscopically guided bronchial brush biopsy was described in the sixties 2. At the same time, the innovating work of Nordenström and Zajicek 3 at the Karolinska Hospital in Stockholm popularized the technique of transthoracic fine needle sampling in the chest. The rate of pneumothorax was dramatically reduced with the systematic use of small gauge needles, although the rate of inadequate cellular material or false negative diagnoses in the confirmation of malignancy persisted in the 15–25% range. False positive diagnoses did not exceed 2%. Transthoracic needle biopsy of mediastinal lymph nodes was described by a transjugular, a paraxiphoid or a paravertebral approach 4, 5. These transthoracic approaches were adopted on a routine basis, when computed tomography (CT) became available. Mediastinoscopy was also developed at the Karolinska Hospital, following the description of “artificial pneumomediastinum” 6. A rigid cystoscope was introduced by Nordenström in the mediastinum under combined fluoroscopic and direct vision control (Nordenström, Karolinska Hospital, Stockholm, Sweden; personal communication). Percutaneous mediastinal puncture however, was not widely carried out before the advent of CT with reduced scanning times. Percutaneous insertion of drainage catheters in fluid collections of the pleura, lung or mediastinum, guided by fluoroscopy or CT was introduced in the late seventies using basic catheter-guidewire techniques, which were applied already in the abdomen 7. Arteriography of the bronchial arteries was also described in Sweden in the sixties. Chemo-infusion in bronchomediastinal arteries for treatment of inoperable bronchial carcinoma was the first clinical application of vascular interventional techniques in the chest, but was not widely spread 8. Catheter embolization of bronchial or systemic arteries for treatment of haemoptysis was introduced in the next decade 9. Miniaturization of catheters and refinement in embolic agents definitely established bronchial artery embolization as an accepted technique. Similar vascular occlusion techniques were applied in pulmonary arteries, first for treatment of haemoptysis, then as a means of occlusion of pulmonary arteriovenous fistula, with coils or detachable balloons 10, 11.
When adequate vascular catheters, wires and other devices, such as snare loops became available, percutaneous foreign body retrieval from the heart or pulmonary arteries became applicable 12. The introduction of expandable metal vascular stents further broadened the spectrum of closed minimally invasive techniques in the chest, allowing for minimally invasive treatment of superior vena cava (SVC) obstruction with an immediate clinical result 13. The most prominent interventional radiological techniques in the chest mentioned earlier will be discussed in this paper.
Percutaneous nonvascular interventions
The various percutaneous nonvascular applications that are in clinical use in the authors’ department are listed in table 1⇓.
Percutaneous imaging guided nonvascular interventions in the thorax
Imaging guidance modalities
Imaging techniques used for the guidance of interventional procedures include fluoroscopy and cross‐section imaging or a combination of both 14. A comparison of the different imaging modalities for percutaneous biopsy or drainage of thoracic lesions is given in table 2⇓.
Comparison of imaging techniques for guidance of thoracic interventions
Fluoroscopy
Uni- or bi-planar fluoroscopy was the first technique to be used as a guidance of percutaneous transthoracic needle biopsy (TNB) and drainage of fluid collections 3, 16–27. Advantages are familiarity to most operators, real-time control of the procedure, and its wide availability in radiological departments. Fluoroscopy allows adjustment of the tip of a catheter previously inserted into a fluid collection with ultrasonography (US) or CT control 28. Opacification of fistulous tracts is best documented with fluoroscopy and plain films, in some occasions in combination withCT.
Computed tomography
CT offers exquisite anatomical display of all the thoracic structures and allows percutaneous access to all spaces with equal ease 14, 19–23, 28–33. Intravenous contrast medium injection is mandatory for identification of necrosis, fluid content, normal vascular structures and false aneurysm located in an abscess wall, and also contributes to a precise delineation of a lesion with regard to the anatomical environment. CT is particularly useful for guiding puncture of a mediastinal lesion and an intrapulmonary lesion that is difficult to localize with fluoroscopy alone 29, 34. CT allows for determination of an optimal cutaneous entry point in such a way as to avoid transgression of a pleural fissure or puncture of large vessels, bronchi and the oesophagus. The spiral scanning capability was not proved superior to sequential scanning 35. Real time CT (fluoro-CT or continuous CT) is now widely available and combines the advantages of cross-section imaging and real time control of the procedure 36, 37.
Ultrasonography
Apart from it being the primary imaging guidance for biopsies of the chest wall or pleural lesions as well as lesions located in the anterior mediastinum 38, 39, ultrasonography (US) is particularly indicated to guide bedside percutaneous aspiration and catheter drainage of a pleural or pericardial fluid collection, even of only small amounts 19–22, 28, 40–43. A subpleural pulmonary effusion and some pulmonary lesions with a parietal contact can also be punctured with US control 44–47. The percutaneous approach is performed in the patient's position that optimally displays access to the lesion.
Transthoracic needle biopsy
In general, percutaneous tissue sampling of a pulmonary, pleural, or mediastinal lesion is performed when histological diagnosis will modify staging of the disease, influence therapeutic strategy, and when the diagnosis cannot be established by bronchoscopic techniques. TNB can be used as a less invasive alternative to mediastinoscopy in some mediastinal lesions as well as medical thoracoscopy in pleural pathologies.
Indications
Main indications for TNB are 14: indeterminate thoracic nodule or mass; pulmonary nodule suggestive of malignancy, surgery being postponed after chemotherapy and/or radiotherapy or replaced by these treatments; nodule in a patient with a clinical history of extrapulmonary primary malignancy, the patient being in clinical remission or presenting multiple primary malignancies; residual nodule following radiotherapy or chemotherapy; tissue sampling for therapeutic sensitivity tests, measurements of tumour markers, hormonal dependence, deoxyribonucleic acid (DNA) analysis, etc; chronic diffuse pulmonary infiltrate and evaluation of suspected focal infectious disease in normal or immunocompromised patients. The need for preoperative diagnosis of a solitary pulmonary nodule varies between institutions, and depends on the pretest probability of diagnosing a lesion that would obviate an unnecessary surgical thoracoscopy or thoracotomy 15. The technique is faster, better tolerated and less expensive than surgery. Percutaneous puncture could also be indicated in localization of a lung nodule with a wire or a hook, or pleural tagging prior to video-assisted thoracic surgery (VATS) 50–53. All mediastinal compartments are accessible to TNB, which is a useful alternative or add-on to mediastinoscopy or mediastinotomy for cytologic or histologic diagnosis of a hilar or mediastinal mass and for staging of lung cancer.
Contra-indications
There is virtually no absolute contra-indication to TNB 14, 54. A vascular structure, hydatid cyst, meningocele or mediastinal pheochromocytoma is usually correctly diagnosed with imaging and/or laboratory tests. Coagulation disturbances should be recognized and corrected before sampling. Puncture of only one functional lung, chronic respiratory insufficiency, pulmonary arterial hypertension, cardiac insufficiency and severe emphysema are relative contra-indications that may increase the complication rate of TNB or render any complication more significant. Dyspnoea or intractable cough or any other inability of the patient to cooperate may be overcome by the use of real time guidance techniques, such as fluoroscopy, US, or fluoro-CT and, if possible, appropriate medication.
Results
TNB has an accuracy varying 80–95% in the confirmation of pulmonary malignancy or malignant mediastinal adenopathy 14, 29, 34, 55–63. The negative predictive value of pulmonary biopsy is 84–96% and false positive results are noted in 2–4% 3, 64. The diagnostic accuracy for small nodules with a diameter of <2 cm is similar to that of larger lesions in experienced hands 65, 66 (fig. 1⇓). A large number of cutting or aspiration needles, including automatic guns, with a needle calibre of <1 mm and a variable tip design are currently used. Almost all needles allow cytological and histological sampling and give similar rates of results and complications concerning diagnosis of malignant or infectious disease. A specific benign diagnosis is more frequently established using a core biopsy needle than on aspiration of clusters of cells (44–100% versus 12–47%) 67–74. Cutting needle biopsy also provides sufficient diagnostic material in patients with mediastinal lymphoma to guide therapy in 81–95% of patients, as well as in diffuse pleural thickening 15, 67, 75–79 (fig. 2⇓). If the sampled material is inadequate or insufficient, but there is a cytologic or clinical suspicion of malignancy, biopsy should be repeated.

Percutaneous transthoracic needle biopsy. a) 11 mm left parahilar nodule (arrow) in a 65-yr-old female. The procedure is performed in right lateral decubitus with a 20 G aspiration needle. Pathology revealed neuroendocrine tumour, confirmed by subsequent surgery. b) 70-yr-old male presenting with a recent history of hepatocellular carcinoma and a past history of melanoma. Transthoracic needle biopsy (TNB) of a 7 mm nodule located in the right upper lobe (arrow) showed metastasis of melanoma. c) 20 mm right hilar mass (arrow) in a 53-yr-old male. Bronchoscopy was unremarkable. TNB performed during contrast medium injection to avoid vascular injury showed small cell lung carcinoma. d) Asymptomatic 45-yr-old female working in a microbiology dept, and presenting with a 35 mm mass (arrow) located in the right upper lobe. Bronchoscopy, bronchial biopsy and bronchoalveolar lavage were negative. TNB demonstrated positive culture for Mycobacterium tuberculosis.

Percutaneous transthoracic pleural biopsy. Right pleural masses in a 33-yr-old female with a past history of invasive lympho-epithelial thymoma treated by surgery and radiation therapy 3 yrs earlier. a) Axial computed tomography (CT) slices demonstrate mild right pleural thickening (arrow) in contact with the 9th vertebral body and rib. b) Three-dimensional reconstruction (surface-shaded display) shows an endopleural view of the pleural surface with a posterior bulging corresponding to the findings of the native scan. Note also two pleural masses located along the diaphragm (arrowheads). c) Transthoracic needle biopsy (TNB) of the posterior pleural thickening confirmed recurrent thymoma.
Complications
The most common complications of TNB are pneumothorax and haemoptysis. The incidence of pneumothorax varies 8–60%, with a mean of 20%. Less than 5% of patients have persistent clinical symptoms and require aspiration or drainage 14, 18, 19, 25. Factors influencing pneumothorax are: chronic obstructive pulmonary disease, especially emphysema, age, poor patient collaboration, experience of the operator, duration of the procedure, number of transpleural needle passes, diameter and flexibility of the needle, depth and diameter of the target, difficulty of localization, cavitary lesion, and mechanical ventilation. Preoperative recognition of risk factors may lead to their correction, by administration of antitussives or bronchodilatators 54, or to the use of more sophisticated techniques, such as a co-axial needle technique, using a larger needle as a guide. In all cases, transgression of the needle through bullae should be avoided and the needle path through the normal lung should be kept to a minimum 80, 81 (fig. 3⇓). Haemorrhage, with or without haemoptysis, is encountered in <10% of TNB, most of which are self-limited 14, 55, 64. Other complications, such as malignant seeding along the needle tract or air embolism, have become exceptional observations since the introduction of fine needle biopsy 82, 83. TNB related death rate is estimated at 0.02% 55.

Artificial widening of the extrapleural space for safe transthoracic needle biopsy (TNB) of mediastinal lesion by an extrapleural approach. A 66-yr-old male presented with dysphagia and altered general condition for since 6 months. Chest radiography showed a middle mediastinal mass. a) Computed tomography (CT) confirms a large mediastinal subcarenal soft tissue mass (arrow). Flexible fibroscopy was unremarkable. Transcarinal needle biopsies were negative. b) CT guided TNB was performed in a prone position. Absence of extrapleural fat prohibits a safe mediastinal access (arrowhead). c) Widening of the extrapleural space was obtained by injection of 50 mL of saline (arrowhead), which displaces the pleura laterally. d) Using a coaxial technique, a small cutting needle was advanced into the lesion through a larger outer needle. Pathology showed poorly differentiated adenocarcinoma.
Clinical usefulness and cost-effectiveness of transthoracic needle biopsy
A comparison of different diagnostic techniques of lung lesions is given in table 3⇓. A recent study on the influence of TNB on treatment showed that management was altered in 51% of patients and unaltered, i.e. confirmed the diagnosis of a resectable malignancy or provided nondiagnostic results in 49%. Surgery was avoided in 83% of biopsies that altered patient treatment 84. When the pretest likelihood of malignancy of a resectable lesion is high, proceeding directly to thoracotomy is appropriate since preoperative TNB is unlikely to alter patient management 15. Otherwise, TNB and fiberoptic bronchoscopy (FOB) must be considered complementary and TNB performed only after a negative FOB. In indeterminate pulmonary nodules, VATS may be the method of choice, providing simultaneous diagnosis and treatment and reducing total cost (table 3⇓).
Comparison of different diagnostic modalities of pulmonary lesions
Percutaneous drainage of thoracic fluid collections
Image guided percutaneous aspiration or drainage of fluid (or air) collection is considered a valid alternative to surgery. Increased safety and effectiveness compared to blind techniques have been largely demonstrated. Any collection located in the pleural space, pericardium, lung or mediastinum can be aspirated or drained percutaneously with catheter placement under imaging guidance.
Pleural collections
Pleural effusions, including empyema, haemothorax, chylothorax and pneumothorax can be considered for percutaneous closed catheter drainage.
Empyema
Indications for catheter drainage depend on the evolutionary stage of the pleural effusion, according to the classification of Light 85–87. The early stage (exsudative phase) corresponds to the secretion of a protein rich fluid by the pleura. This is a mandatory transitional phase for empyemas and does not require drainage. The second stage (fibrinopurulent phase) is characterized by a viscous and opaque fluid with increased cellularity. Deposition of fibrin layers on the pleural surface promotes the formation of pleural pockets and progressive lung entrapment. Medical treatment without effective fluid drainage might fail. The third stage (organizing phase) is characterized by fibroblastic infiltration of the pleura, limiting the expansion of the underlying lung due to pleural peels. Early drainage of a complicated effusion is necessary to prevent progression to the organized phase, which requires surgical decortication. In surgical treatment, blind placement of a thoracostomy tube (30F–34F) is followed by open surgical drainage if unsuccessful, although some surgeons recommend early open drainage, and pleural decortication, as the initial therapeutic approach 85, 88.
Imaging guided percutaneous drainage avoids the potential failures associated with blind chest tube placement, which can occur in about 50% of patients due to inadequate positioning of the tube or to undrained satellite pleural pockets 86, 87. The size of the percutaneous catheters that are in regular use varies from 7F–30F and is chosen according to the viscosity of the fluid to be drained. CT discloses all satellite noncommunicating pleural pockets, that are drained with multiple catheters. Pleural fluid, which is encapsulated in a fissure can also be adequately drained with CT control, most often without transgression of normal lung by the catheter. Technical success is achieved in almost all cases. Clinical success is achieved in 70–89% of the patients treated in a first intent, depending on the stage of empyema 14, 17, 20–22, 25, 27, 28, 31, 32, 41, 42. A similar success rate of 80% is obtained in patients treated in a second intent following failed surgical chest tube drainage 14, 17, 21–23, 27, 28. Failure of percutaneous drainage varies 11–30%, and usually occurs in chronic empyema (stage III), when extensive pleural peels have formed, which may prevent catheter insertion, or the cavity to collapse and obliterate. CT may have its difficulties to accurately differentiate between the fibrinopurulent and organizing phase of empyema 89. Medium sized catheters are better tolerated by the patient than large thoracostomy tubes, but their lumen is more prone to obstruction by fibrin products. Intrapleural injection of fibrinolytic agents was recently proven to be efficient in preventing fibrin deposit and formation of secondary loculation of the empyema, with a clinical success rate of 62–100% 14, 23, 26, 90–104. Local instillation of fibrinolytics also reduces the number of drainage catheters, that are necessary to drain all loculations, duration of drainage and hospitalization and prevents fibrosis of the pleural surface (fig. 4⇓). Table 4⇓ summarizes the basic principles and recommendations for successful treatment of complicated pleural empyema. Overall, the added cost of imaging guidance is largely compensated for by the savings from an increase in clinical success.
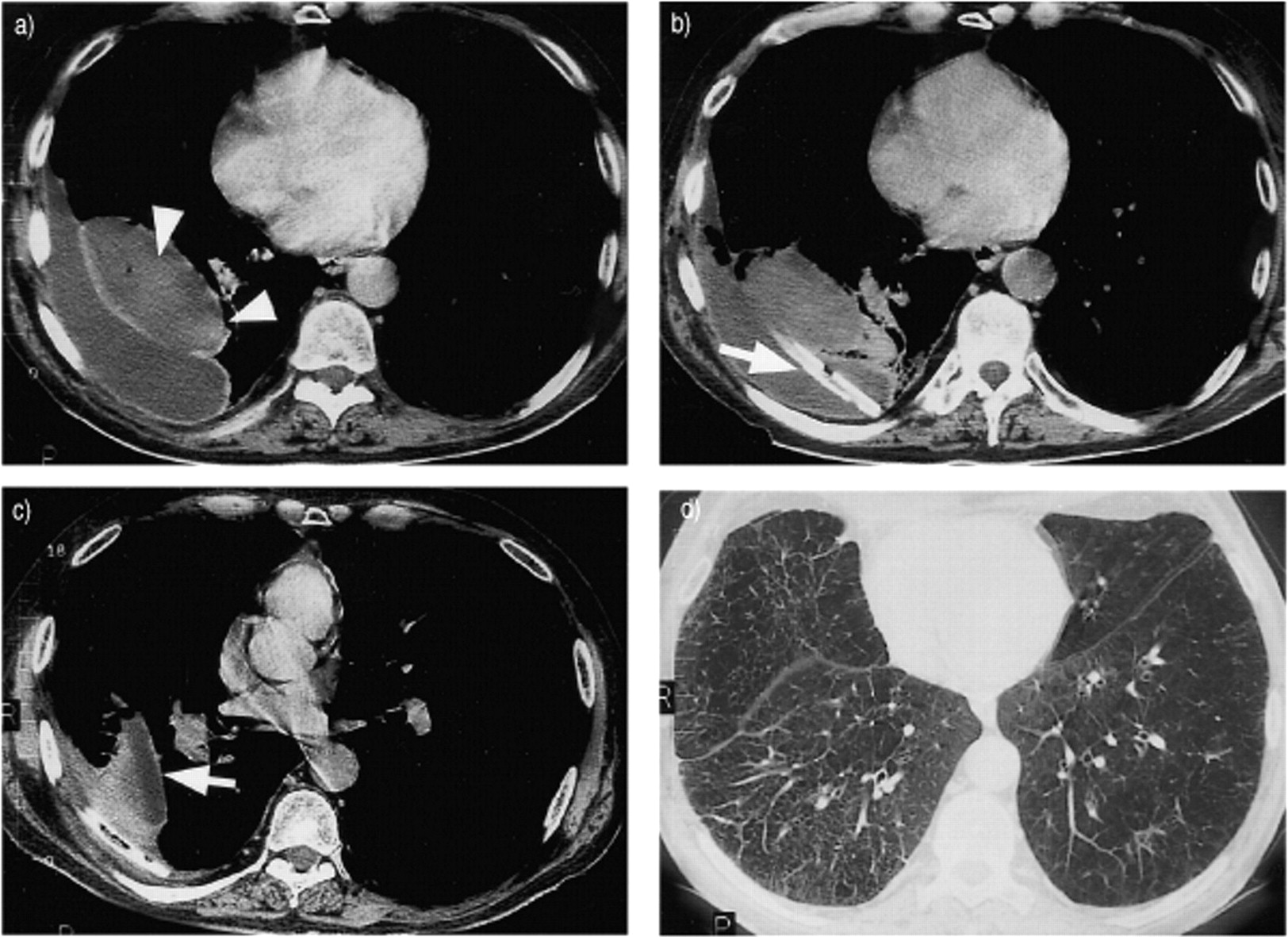
Percutaneous drainage of pleural collection. A 64-yr-old male with chronic obstructive pulmonary disease (COPD) presented with right multiloculated pleural collection, following surgical drainage of pneumothorax complicated by superinfected hemothorax. a) Contrast-enhanced spiral computed tomography (CT) section demonstrates a large multiloculated pleural collection. Areas of high densities (arrowheads) suggest presence of fresh clot. b) Aspiration with a Teflon-sheathed catheter confirms the presence of blood; a 24F chest tube (arrow) was inserted in the dependant part of the collection. Cultures were positive for Escherichia coli. 200,000 IU of urokinase were injected per day for 5 days. c) Spiral CT control demonstrates regression of the collection and persistence of an intrafissural collection (arrow). Urokinase injection was continued for 3 more days before chest tube removal and discharge of the patient. Total drainage volume was 1200 mL. Note on figures b) and c) 4 to 5 mm pleural thickening at the time of drainage. d) High-resolution computed tomography (HRCT) at 1 yr demonstrates complete regression of pleural thickening, with subnormal expansion of the right lower lobe.
Basic principles of image guided drainage (modified from Moulton) 87.
Malignant pleural effusion
Recurrent malignant pleural effusion, that is not controlled by systemic treatment, is usually drained with a soft and small catheter (8F) followed by pleural sclerosis by intrapleural injection of talcum, doxycyclin, bleomycin or other drugs. Advantages of small catheters compared to classic large-bore thoracostomy tubes are the possibility of treatment on an outpatient basis and increased patient comfort. Advantages of imaging guidance is the proper insertion of the catheter inside the pleural cavity, thus avoiding injury of a pleural mass, which may bleed during catheter insertion, nonrecognition of persistent undrained loculations and uncomplete lung re-expansion before pleural sclerosis. Complete regression of a malignant pleural effusion is obtained in 53–81% and partial resolution in up to 95%, which is a similar response rate than obtained with large thoracostomy tubes 24, 43, 105–107.
Haemothorax
Post-traumatic haemothorax is usually drained by large-bore surgical chest tubes. In selected cases with persistent intercostal or phrenic artery bleeding, angiography and transcatheter embolization is indicated before drainage. Long-lasting multiloculated haemothorax is an indication for image-guided catheter drainage. Fibrinolytic agents can be safely injected in a pleural haematoma at 1 week following trauma 97, 98 (fig. 4⇑). Uncontrolled intrapleural bleeding is an absolute contra-indication of intrapleural fibrinolysis.
Pneumothorax
Postbiopsy or spontaneous pneumothorax can be drained percutaneously with a small calibre catheter (fig. 5⇓). Success rate of drainage of iatrogenic pneumothorax is 75–97%, the vast majority resolving within 24–72 h 18, 19, 25, 86, 107, 108. Catheters can be connected to a one-way Heimlich valve. Recurrent pneumothorax can be treated with chemical pleurodesis if surgical therapy is not an option.
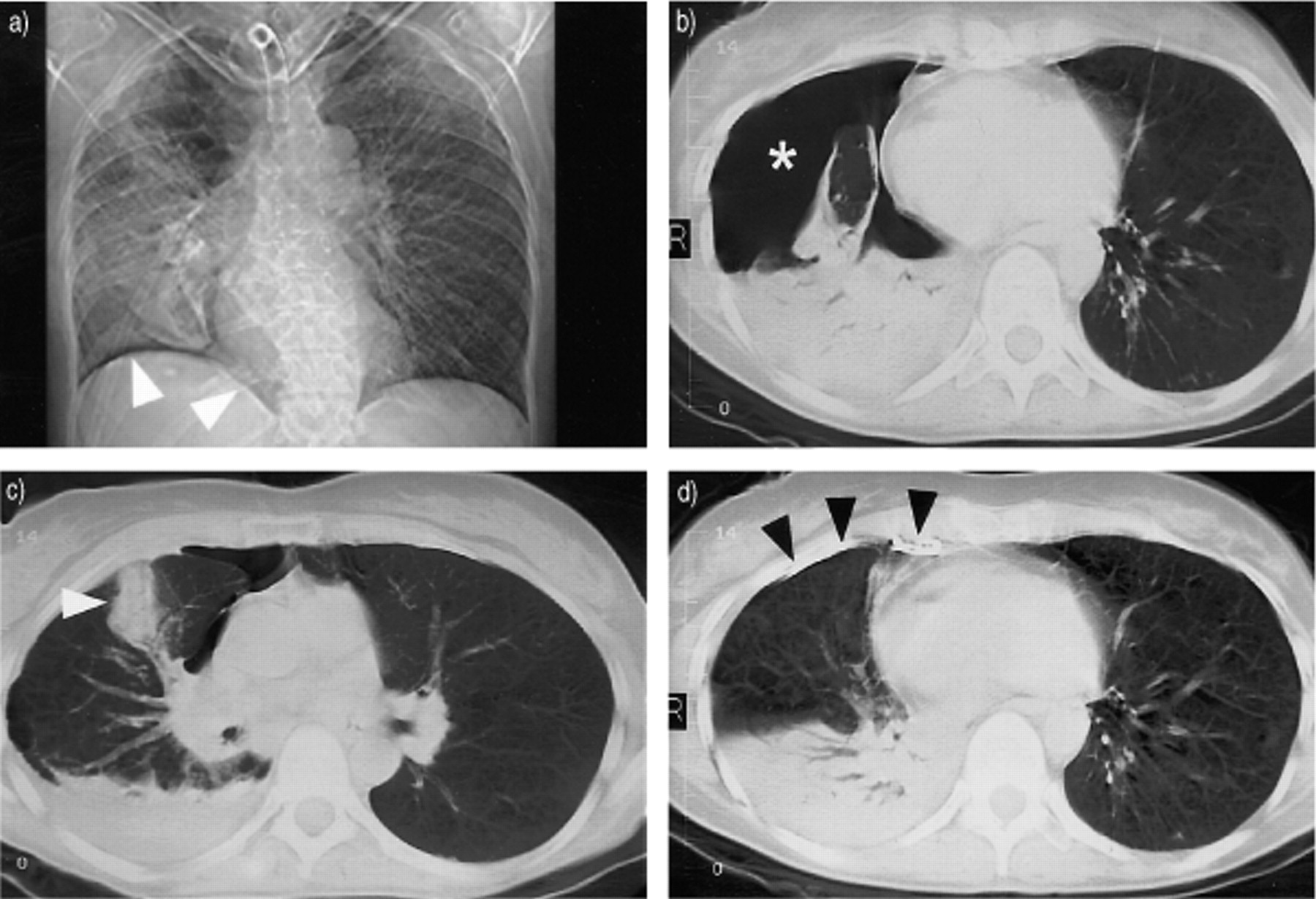
Percutaneous drainage of loculated pneumothorax. A 37-yr-old female with a past history of multiple sclerosis presented with severe dyspnoea and temperature. Chest radiography showed a right pneumothorax, pulmonary infection and large bullae in the right apex. a) Insertion of 3 large-bore chest tubes failed to resolve a pneumothorax located in an antero-inferior position (arrowheads). b) and c) Spiral computed tomography (CT) confirmed basal pneumothorax (star) and right lower lobe atelectasis with pleural effusion of limited volume. A previously blindly placed chest tube is located inside the lung parenchyma, and surrounded by areas of pulmonary hemorrhage (arrowhead). Laterally, adhesions have formed between the parietal and visceral pleura. d) A 9 F pigtail catheter (arrowheads) was inserted under CT guidance in the anterior costo-diaphragmatic sulcus and drained air and 200 mL of sterile fluid. Subsequent chemical pleurodesis was performed through the pleural catheter.
Pulmonary collections
Abscess
Pyogenic pulmonary abscesses rarely occur today, owing to progress in antibiotic treatment and a more efficient eradication of the cause. When resistant to medical treatment, postural and bronchoscopic drainage, lung abscess is amenable to percutaneous catheter drainage before considering surgery 14. Abscesses frequently present with a large pleural contact, which allows percutaneous insertion of a 7F–14F catheter without transgression of normal lung parenchyma (fig. 6⇓). Resolution of the abscess is obtained in 73–100% following 10–15 days of drainage 7, 30, 31, 33, 40, 109–113. Pulmonary abscesses may have a thick wall and complete collapse of the cavity may take 4–5 weeks. Decompression should be performed slowly to avoid rupture of a vessel or a Rasmussen pseudoaneurysm incorporated in the abscess wall. Surgery remains necessary when extensive necrotizing pneumonia or life-threatening haemorrhage has occurred 14.
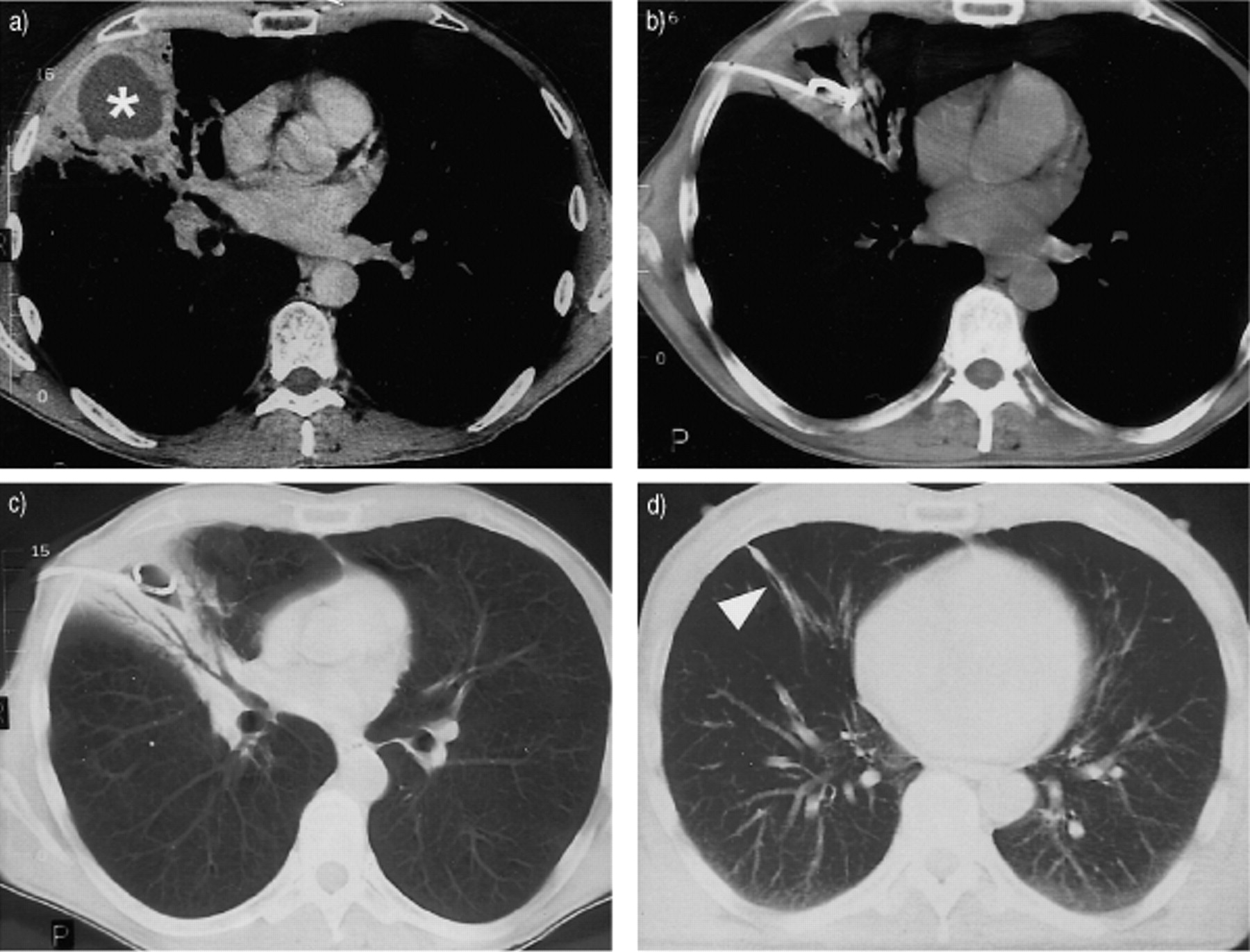
Percutaneous drainage of pulmonary abscess. A 55-yr-old male with a past history of hemilaryngectomy for squamous cell carcinoma and recurrent episodes of aspiration presented with elevated temperature and altered general condition. a) Contrast-enhanced computed tomography (CT) demonstrates a 5-cm pulmonary abscess (star) located in the right middle lobe. b) An 8F pigtail catheter was inserted in the abscess under CT guidance through the large thoracic wall contact of the abscess. Forty mL of pus were aspirated. Thirty mL were drained during the next 3 days. Cultures were negative. c) CT control on the third day showed partial collapse of the cavity, filled by air and surrounded by parenchymal consolidation. The catheter was removed. d) CT control obtained 3 months later showed complete disappearance of the lesions and a plate-like atelectasis (arrowhead).
Aspergilloma
Life-threatening haemoptysis due to intracavitary aspergilloma may be recurrent, despite an initially successful bronchial embolization, and eventually require surgical resection 114–120. Open thoracotomy however, can be contraindicated in some patients who present with a severe underlying pulmonary condition 118, 120. Transthoracic instillation of amphothericin B has been described with a success rate of 50% for resolution of the aspergilloma and 75–100% for acute control of haemoptysis 117–121.
Pneumatocele and bulla
Percutaneous drainage of infected or tension pulmonary pneumatocele has been described 14, 122. A percutaneous diagnostic aspiration with an 18-Gauge needle can precede catheter insertion in doubtful cases, as bullae may frequently contain an air fluid level, without infection.
Mediastinal collections
Abscess
Mediastinal abscesses are challenging to treat by a closed percutaneous approach, as overall prognosis of the patient is usually poor. Mediastinal collections can be drained under CT guidance using a parasternal catheter approach for collections located in the anterior mediastinum (fig. 7⇓) and a posterior paraspinal approach for safe access to the posterior and middle mediastinal compartments 14, 27.
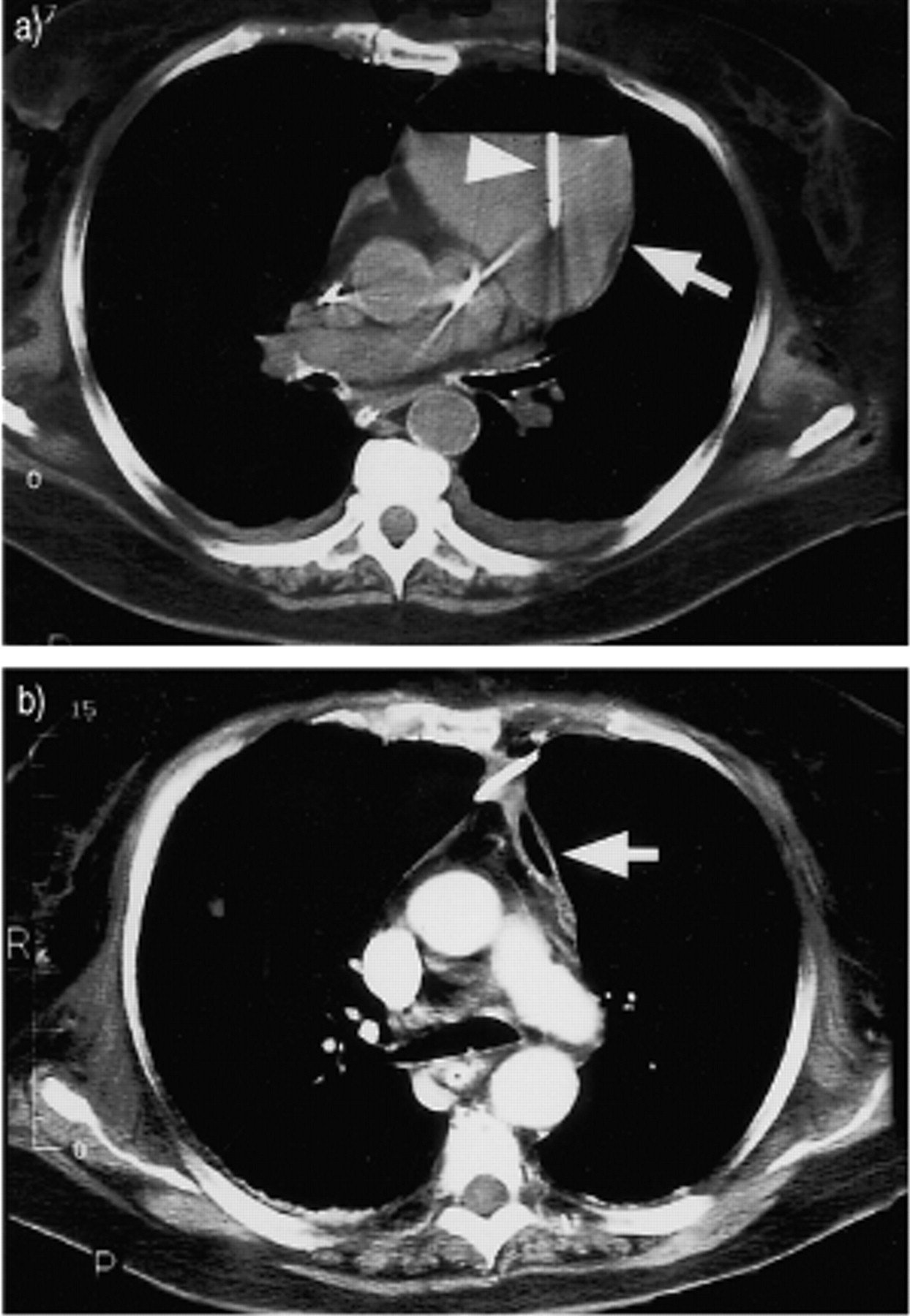
Percutaneous drainage of mediastinal collection. A 68-yr-old female presented with epilepsy related to a frontal cerebral haematoma. Latrogenic bilateral pneumothorax and pneumomediastinum followed difficult intubation with laceration of the tracheal wall. Pneumothoraces were drained by surgical chest tubes; 2 days later, chest radiography showed a large mediastinal widening. a) Computed tomography (CT) demonstrates an extensive hydro-haemomediastinum located in the anterior mediastinum (arrow). A 9F pigtail catheter (arrowhead) was inserted under CT guidance, and drained 450 mL of bloody fluid in 48 h. b) CT control at 48 h showed complete regression of the collection (arrow).
When a mediastinal abscess is associated with oesophageal perforation, an oesophageal catheter can be inserted in the mediastinum over a guide wire through the oesophageal tear 123. The few reported series indicate a success rate of 83–100%, but 30 days mortality is high, owing to the underlying disease 31, 123–125.
Pericardial effusion
Most pericardial effusions are drained under US control using a subcostal or a subxyphoid approach 126. When US fails, fluid can be drained under CT guidance, by an atypical left anterolateral approach 127 (fig. 8⇓).

Percutaneous pericardial drainage. A 38-yr-old female presented with sudden dyspnoea following left pneumonectomy for tuberculosis complicated by aspergilloma, unresponsive to medical treatment. a) Echocardiography demonstrated cardiac tamponade, confirmed by computed tomography (CT) Percutaneous insertion of a 5F catheter in the posterolateral part of the pericardial sac under CT guidance allowed aspiration of 410 mL of a sterile bloody effusion. b) Immediate CT control following catheter placement and aspiration showed almost complete regression of effusion and increase of volume of the heart chambers. The 5F catheter was exchanged for an 8F pigtail catheter to avoid clogging. The catheter was left in place for 72 h and drained 50 mL of blood. No recurrence.
Tension pneumomediastinum
Tension pneumomediastinum usually results from barotrauma in mechanically ventilated patients. A tension mediastinal emphysema may compress the large mediastinal veins and the heart, leading to pseudotamponade which urges for rapid decompression. The usual treatment is mediastinostomy. Percutaneous insertion of a 12F or 14F catheter with sideholes into a retrosternal mediastinal gas collection under CT guidance is an alternative emergency treatment 128.
Others
Ectopic pancreatic pseudocysts, pleuropericardial, parathyroid or bronchogenic cysts, necrotic tumours, lymphoceles and haematomas can be drained or aspirated percutaneously using imaging guidance 14.
Vascular interventions
Vascular interventions that are in clinical use are listed in table 5⇓.
Vascular interventions in the thorax
This section focuses on the treatment of haemoptysis, pulmonary arteriovenous malformation and pseudoaneurysm, superior vena cava obstruction and percutaneous retrieval of vascular foreign bodies.
Bronchial artery embolization
Indications
Haemoptysis can be classified as massive (>300 mL in 24–48 h), moderate (≥3 episodes of >100 mL within a week) and chronic (quantitatively small episodes of haemoptysis repeated over the course of weeks or months). Massive haemoptysis carries a high mortality rate in patients treated conservatively, and many patients are unfit for lung resection. When surgery is performed in an acute situation, morbidity is high and a mortality rate of 35% has been reported 129–133. Most frequent causes of bleeding include tuberculosis, chronic infection, bronchiectasis, aspergilloma, pneumoconiosis, bronchogenic carcinoma, pulmonary metastasis and pulmonary infarction 132, 134–136. Chest radiography and bronchoscopy should be obtained immediately to localize the site of bleeding. CT may be considered in noncritical patients to search for the underlying cause or determine the exact bleeding site whenever chest radiographs are inconclusive. In cases of massive haemoptysis requiring an urgent embolization, angiography is recommended as the initial intervention. Following embolization, surgery can be carried out in a second intent for localized disease 133. In moderate or chronic haemoptysis, bronchial embolization is the only treatment, when unresponsive to medical treatment in the following situation: recurrent haemoptysis following surgery, postradiation lung, unresectable carcinoma, bilateral pulmonary disease, inadequate lung function to tolerate resection, failure to localize a bleeding source roentgenographically and/or bronchoscopically, and large transpleural connections between bronchial and nonbronchial systemic arterial supply.
Technique
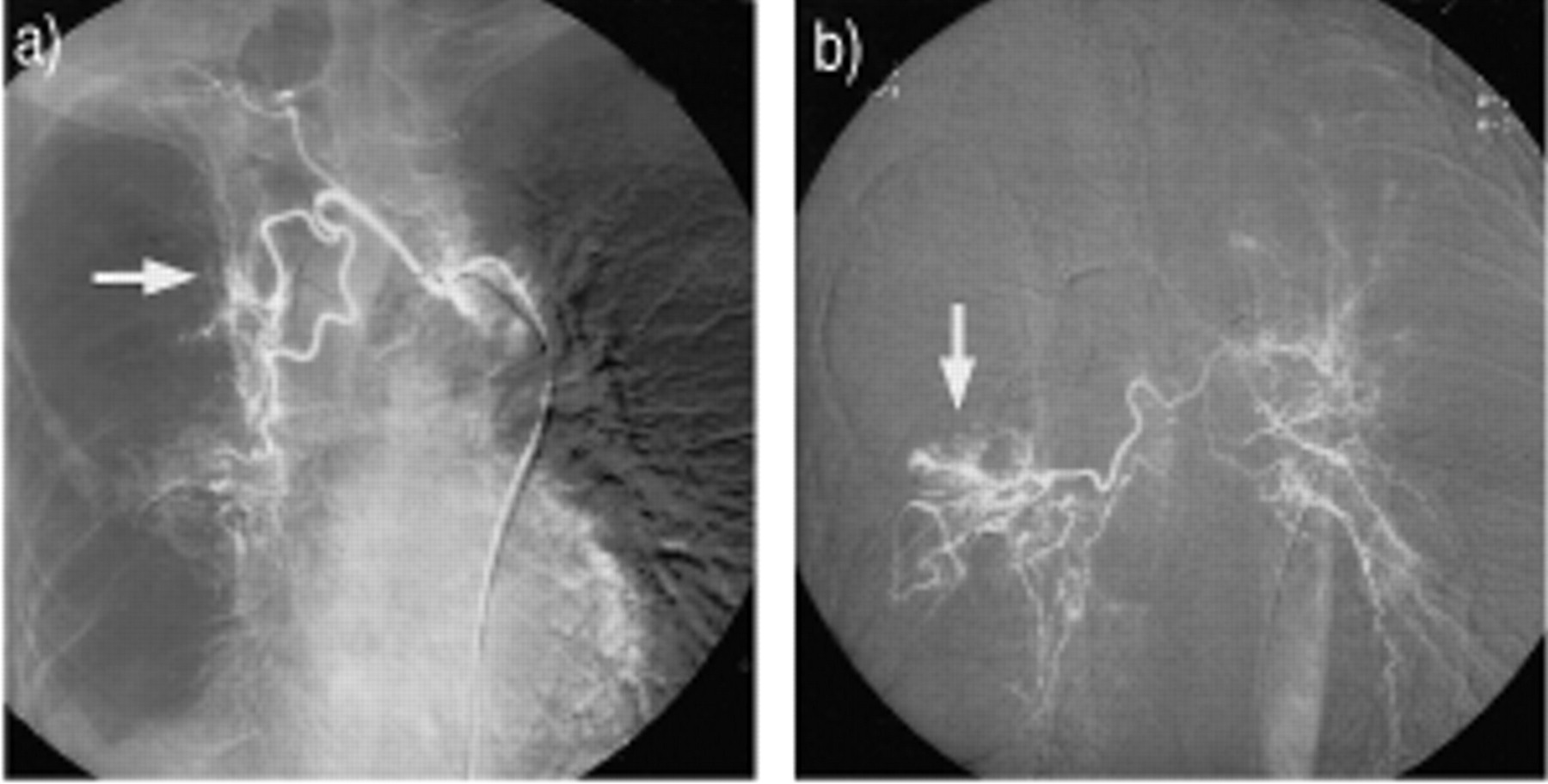
A thoracic aortogram is always obtained to map all bronchial arteries and systemic nonbronchial feeders of the bleeding site. Selective opacification of all bronchial arteries is then performed beginning with the vessels directed to the suspected bleeding area. Arteries with an increased calibre, and a tortuous course and parenchymal hypervascularity are found (fig. 9⇓). Contrast extravasation in the lung parenchyma or in the bronchial lumen is not required to decide on embolization. Vaso-occlusion is best performed through a microcatheter that is inserted coaxially through a diagnostic catheter, the tip of which is placed in the proximal portion of the vessel or at its ostium. Microcatheters, which can be placed selectively distal to the origin of a spinal artery are not occlusive and allow for optimal catheter stability and safety during embolization avoiding reflux of embolization material 136–138. Polyvinyl alcohol particles, gelfoam and dextran microspheres are among the agents that are in frequent clinical use. Additional bronchial and nonbronchial collaterals (internal and external thoracic arteries, periscapular arteries, cervical arteries, intercostal arteries and inferior phrenic artery) are catheterized and may be treated, when their contribution to the hypervascular area is shown on angiography 132, 139, 140 (fig. 10⇓). Nonbronchial systemic collaterals may resume the distal bronchial circulation after a previous bronchial embolization and be responsible for bleeding recurrence 141.

Embolization of bronchial arteries. A 71-yr-old male with a past history of pleuroparenchymal tuberculosis presented with chronic episodes of haemoptysis of small amount for 5 months. The patient underwent previous bronchial embolization for haemoptysis 11 yrs before. a) Arteriography of the right intercostobronchial trunk demonstrates an increased calibre and a tortuous course of the bronchial artery and areas of parenchymal hypervascularity (arrow). Embolization with polyvinyl alcohol particles was performed. b) Arteriography of a common right and a left bronchial arterial trunk showed other areas of abnormal hypervascularity fed by a dilated and tortuous right bronchial artery (arrow). Embolization with particles.

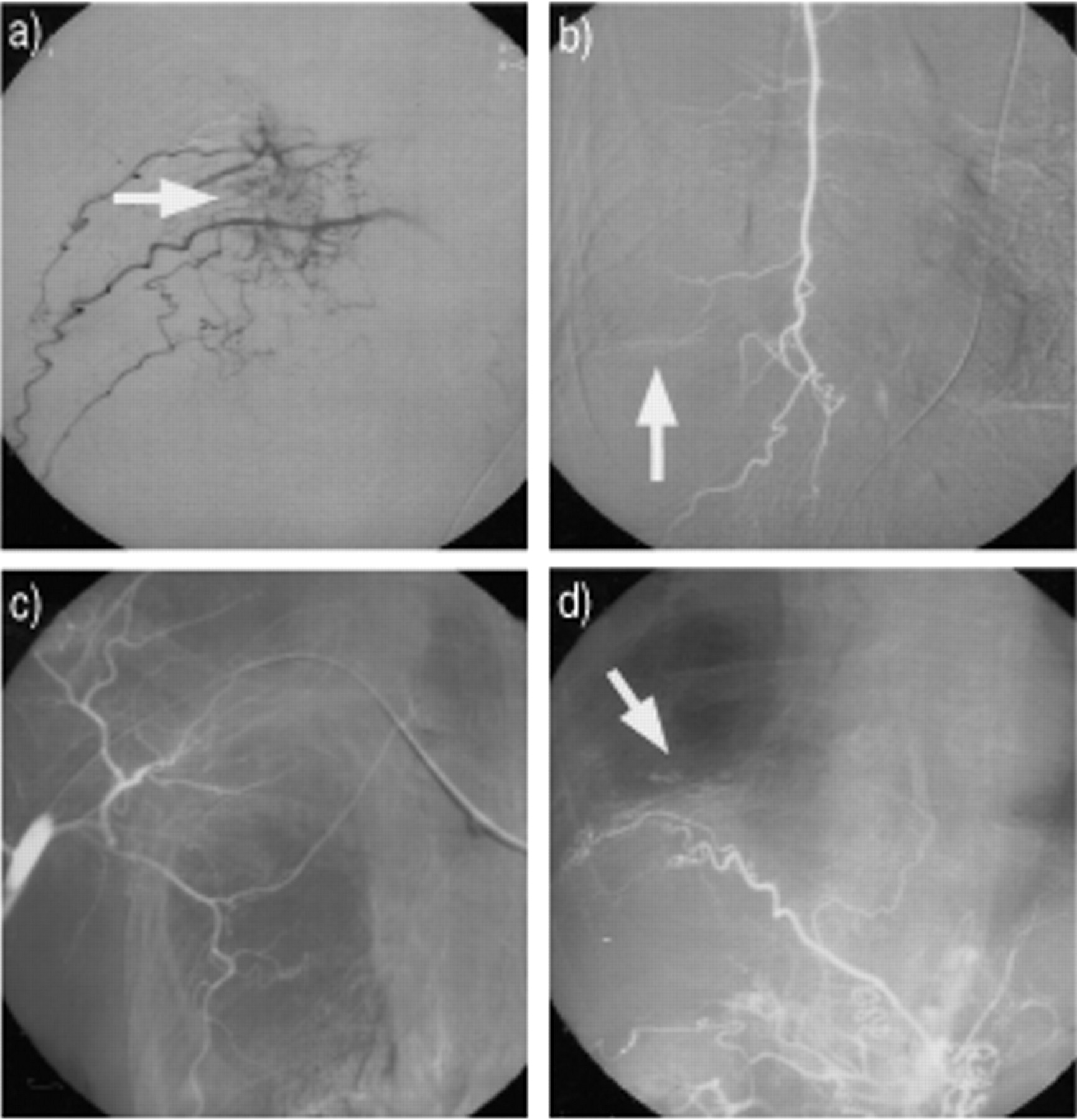
Embolization of systemic nonbronchial collaterals (same patient and same procedure as in fig. 9⇑). a) Opacifica-tion of a dilated fourth right intercostal artery and adjacent metameric arteries, shows extensive pleural and parenchymal hypervascularization (arrow). Embolization with particles. b) Opacification of the right internal thoracic artery shows a small parenchymal blush in the lower part of the right hemithorax. No embolization is required. c) Opacification of periscapular and external thoracic arteries. Normal aspect. d) Opacification of the right inferior phrenic artery, showing limited basal pleuroparenchymal hypervascularization (arrow). No embolization.
Results
In a review of the recent literature, bleeding (predominantly massive) was controlled in an acute setting in 75–90% of the patients 142. Bleeding recurrence rate was 16–48%. In one study with long-term outcome, the Kaplan-Meier curves showed 18% of recurrences within 7 days, 24% within 1 month, 33% within 6 months and 38% within 1 yr. No further recurrences occurred 1–2 yrs after embolization 142. Recurrence can be caused by incomplete bronchial embolization, recanalization of an embolized artery, development of extrapulmonary systemic collaterals (short-term recurrence), or by progression of the underlying disease (long-term recurrence) 136, 142. Usually, recurrent haemoptysis responds to a second embolization procedure. Bleeding from a pulmonary artery should be suspected if the bronchial arteries are angiographically normal or if embolization of the bronchial and nonbronchial arteries fails to stop the bleeding.
Complications
Complications are encountered in 1% ofthe patients. A postembolization syndrome may beobserved (pleuritic pain, fever, dysphagia, leukocytosis); it will last for 5–7 days and responds to symptomatic treatment 143. Bronchial wall or oesophageal wall necrosis, inadvertent facial or abdominal visceral embolization, myocardial infarction and spinal cord infarction are rare complications that can be avoided by proper technique.
Pulmonary artery embolization
Arteriovenous malformation
Indications
Pulmonary arteriovenous malformations (PAVMs) are arteriovenous shunts which represent a potential source of paradoxical emboli through a right to left shunt, without altering pulmonary artery pressure or cardiac output. Other potential complications include systemic oxygen desaturation resulting in polycythaemia, and haemoptysis or haemothorax caused by rupture of the aneurysmal sac. Most PAVMs are congenital and multiple, being part of the hereditary haemorrhagic telangiectasia (Rendu-Weber-Osler) syndrome, while a minority are acquired, mainly secondary to vascular damage 136, 144–147. They can be classified as simple (one segmental feeding artery: one draining vein) or complex (several segmental feeding arteries: one or several draining veins) 148, 149. Before 1980, surgical lobectomy or pulmonary wedge resection was the only valid therapy. Selective embolization is at present considered the treatment of choice for PAVMs which show a feeding artery superior to 3 mm in diameter. In fact, large shunts are associated with an increased incidence of paradoxical emboli potentially causing severe neurological complications 146–153. Multiple microscopic shunts are usually present in addition to the visible fistulae and small AVMs may increase in size during lifetime. Endoluminal embolization offers the advantage of a maximal preservation of normal lung parenchyma around the malformation, particularly in patients with multiple and bilateral PAVMs.
Technique
Pre-embolization thin section helical CT with 3D reconstruction of the PAVM is an important step in identifying all small feeding arteries, which may be responsible, when not recognized, of persistent shunting following embolization of the main feeder only 149. Selective transcatheter embolization of all feeding arteries is performed with steel coils with attached cotton strands (fig. 11⇓). All catheter and guidewire exchanges and coil introduction into the catheter are performed “under water” to avoid air embolism to the brain. Compact placement of endoluminal coils and choice of large “tornado” shaped coils or use of a controlled coil detachment technique are important keypoints for successful treatment to avoid transfistulous coil migration. The site of groin access should be alternated in multiple interventions to avoid femoral vein thrombosis.

Embolization of pulmonary artery vascular malformation (PAVM). A 49-yr-old male presented with polycytaemia in the department of Haematology. Investigations were noncontributive except chest radiography, which depicted a pulmonary mass in the left lower lobe behind the haemidiaphragm. a) Contrast enhanced spiral computed tomography (CT) shows a solitary 3 cm PAVM (arrow) in the left lower lobe. b) 3D-CT reformatting demonstrates a simple angioarchitecture of the malformation with one feeding artery (A) and one draining vein (V). Note the division of the feeder in small afferent branches (arrowheads) before entering the aneurysmal sac. c) Selective angiographic opacification shows the same findings than in figure (b) (arrowheads). d) Angiography control following embolization with steel coils of the feeding artery close to the aneurysmal sac in order to preserve surrounding parenchymal vascularization. Polycytaemia improved in the following weeks.
Results
Closure rate of PAVMs is 98% and results in palliation of the right to left shunt and probable prevention of haemorrhagic and thromboembolic complications caused by major PAVMs 136. There is no evidence based benefit on patient's survival. Multiple treatment sessions are needed in 20–40% of cases. Embolization can fail in case of a unrecognized persistent feeding artery, recruitment of feeders, including bronchial arteries in 4% of the cases, recanalization of occluded feeders or growth of other PAVMs.
Complications
Potential complications are encountered in <10% of the patients and include pulmonary infarction distal to the occlusion, pleurisy, sepsis and retrograde pulmonary embolism in patients with polycythaemia.
Pseudoaneurysm
Destructive processes of any origin, including trauma (particularly iatrogenic, i.e. Swan-Ganz catheter), infection, tumour, and inflammatory disease, can erode the wall of a pulmonary or bronchial vessel, and lead to the formation of a pseudoaneurysm 154. Prompt therapy is required, as false aneurysms are at risk of enlargement and rupture, which can lead to lethal haemoptysis in >50% of the patients 155. Multiple therapeutic procedures have been used to control pulmonary artery bleeding. Palliative measures include Swan-Ganz balloon tamponade of the affected vessel and endobronchial tube placement with positive end-expiratory pressure. Surgical management generally comprises resection of the involved lobe, or in selected cases, aneurysmectomy 155. Endoluminal catheter embolization of the parent artery with steel coils has emerged as an alternative noninvasive technique, particularly in emergency cases 154, 156. Intrasaccular embolization with steel coils has the advantage of preserving the distal pulmonary artery and sparing of pulmonary function distal to the pseudoaneurysm 154 (fig. 12⇓).

Endoluminal intrasaccular embolization of pulmonary artery pseudoaneurysm. An 85-yr-old female presented with haemoptysis 8 days following insertion of a Swan-Ganz catheter. a) Contrast-enhanced spiral computed tomography (CT) demonstrates a 3 cm pseudoaneurysm located in the internal segment of the middle lobe (arrow). b) Angiographic selective catheterization of the internal segmental artery of the middle lobe confirmed the pseudoaneurysm. Intrasaccular embolization of the pseudoaneurysm was performed by filling with ten 15 cm-long, 2 cm-diameter steel coils. c) Angiographic control showed complete occlusion of the pseudoaneurysm and normal perfusion of the middle and lower lobe branches. d) Contrast-enhanced spiral CT scan confirmed complete thrombosis of the pseudoaneurysm.
Percutaneous recanalization and stenting of the superior vena cava and innominate veins
Rationale
The potential of the venous system to collateralize and the usually nonacutely lethal nature of SVC obstruction are the main reasons why medical management and radiotherapy are preferred to other invasive therapeutic procedures for correction. Percutaneous transluminal angioplasty (PTA) is rarely successful in large vein obstruction, due to elastic recoil of the venous wall and/or persistent perivascular compression. The rationale for using expandable metal stents in benign and malignant SVC obstruction is the immediate and permanent achievement of venous patency.
Indications
Potential indications for percutaneous stenting of the SVC and innominate veins are mainly primary or secondary malignant tumours with mediastinal location, such as bronchogenic carcinoma, lymphoma, or metastatic adenopathy and benign stenoses related to central venous lines, haemodialysis shunts, and rarely postoperative anastomotic stenoses, or fibrosing mediastinitis 13, 157–161.
The advantage of endoluminal desobstruction over radiation therapy or chemotherapy is the immediate correction of disabling symptoms and the still possible application in patients who have already received the maximum radiation dose. Patients with imminent SVC obstruction should be treated before they become fully symptomatic, when encasement of the innominate vein, SVC bifurcation is suspected, as a Y‐shaped stricture is technically more difficult to treat than a straight vein segment. Multiple and bilateral stents might be required to treat the bifurcation and regional thrombolysis, preceding stent placement might be necessary to clear the lumen from thrombosis before stenting. Patients in whom nephrotoxic chemotherapy or other nephrotoxic drugs are given and patients in whom extensive tumourlysis with hyperuricaemia, hypercalcaemiaand emesis-related dehydration is expected may also benefit from SVC desobstruction to increase tolerance of high volume hydration, even if clinical symptoms of venous stasis are not prominent.
Relative contra-indications include preterminal patients with malignant disease, extensive chronic venous thrombosis, endoluminal tumour growth, and upper limb paralysis. Occlusion of the ostium of the azygos vein is not a contraindication. Mechanical thrombectomy using rotational catheters or other devices should not be used in the SVC system, because of the risk of pulmonary embolism by a jugular vein thrombosis, that may become mobilized after successful clearance of the downstream veins. Patients with simultaneous tracheobronchial and mediastinal vein obstruction should undergo stenting of the airways first.
Technique
Although SVC stenting is a straight forward procedure in simple cases, it can become extremely complex in cases with extensive obstruction. Phlebographic demonstration by a bilateral arm injection of contrast medium is mandatory before treatment, to locate the obstruction, appreciate its haemodynamic significance, extent of collateral venous drainage and any congenital variants and to allow planning of the stenting procedure (fig. 13⇓). In patients with severe oedema of the upper limbs, puncture of the axillary vein may be targeted by a peripheral hand vein injection of carbon dioxide. In case of acute or subacute venous thrombosis, local catheter directed thrombolysis may be indicated, using an infusion of 70,000–100,000 IU of urokinase per hour or another plasminogen activator. Chronic occlusion is recanalized with catheter-guidewire techniques by a unilateral or bilateral axillary vein or a femoral vein approach, or a combination of both. Self-expandable and flexible metal stents are placed, when necessary, multiple and bilateral and in an overlapping position. Stent placement in the subclavian vein should be prohibited because of the risk of subclavian vein thrombosis or stent fragmentation by external clavicular compression. Stents in large veins should be oversized by 25–50% compared to the diameter of a fully dilated normal vein. PTA is not indicated prior to stenting in malignant disease, but should be performed after stenting to establish optimal venous return immediately. In stenosis of benign origin, PTA is indicated prior to stenting to probe the degree of stenosis and for precise localization of maximum of resistance within the stenosed venous segment. Perprocedure heparinization is advised in all cases 162, 163.

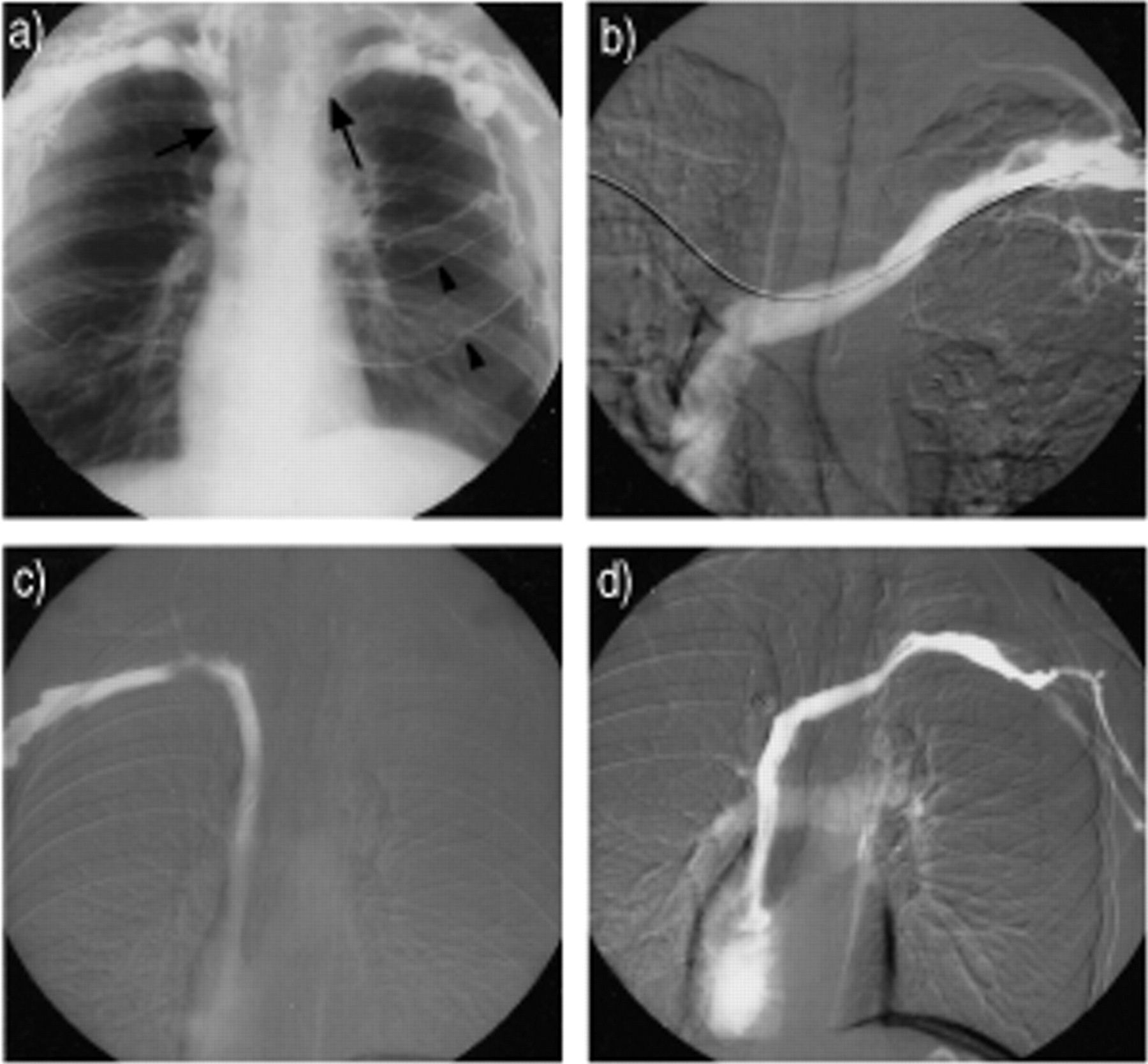
A 36-yr-old female with mediastinal non-Hodgkin lymphoma, treated by chemotherapy. Prominent symptoms of superior vena cava obstruction. a) Bilateral arm phlebography shows obstruction of right and left innominate veins (arrows) and lateral thoracic collateral circulation (arrowheads). b) Venous recanalization was performed by a bilateral axillary vein approach. Note recanalized and stented left innominate vein. c) and d) Phlebography shows normal flow in both innominate veins after bilateral stenting with 10 mm Wallstents.
Results
Following successful restoration of flow in the SVC and innominate veins, complete or significant relief from symptoms is obtained in 68–100% of patients with malignant disease 158–164. Delayed reintervention during the patient's survival is only rarely required for a follow-up of 16 months. The type of bare metal stent is irrelevant to clinical results. Covered stents are generally not indicated, as endoluminal tumour extent is an exceptional observation. The most prominent clinical symptoms are corrected within a few hours, face and neck oedema resolves in 1–2 days, and upper limb oedema in 2–4 days. Benign SVC obstruction is observed with increasing frequency in recent years. Generally patients with a benign stenosis present at the moment of treatment with extensive thrombosis due to delayed patient referral. Overall, similar results may be obtained in stenosis of malignant and benign origin, although a longer observation time in the benign group allows for more delayed complications to occur. Haemodialysis related central venous stenoses are particularly prone to formation of exuberant intimal hyperplasia within the stent or formation of stenosis in the adjacent venous segment. Repeated PTA or placement of an additional stent may be required during the first years of follow-up. Stents should not be placed in arm veins, as secondary obstruction is the rule 162, 165–168.
Complications
Complications of venous desobstruction are few. Local thrombolysis may lead to haemorrhagic complications. Stent related complications include misplacement or migration, uncomplete stent opening, formation of de novo thrombosis, and pulmonary embolism. Vein perforation, significant infection, phrenic nerve deficit by stent compression or puncture site complications are rare.
Percutaneous vascular foreign body retrieval
Indications
Since its introduction, percutaneous catheter mediated vascular foreign body retrieval has emerged as the treatment of choice, avoiding thoracotomy and open heart surgery 12. The growing clinical application of intravascular devices in interventional radiological practice has increased the risk for central venous embolization of many types of foreign materials besides the classical lost central venous lines, Swan-Ganz catheters, ventriculo-atrial shunts, port‐a‐caths, cardiac stimulator lines and pacemaker electrodes. All intravascular embolized foreign bodies should be retrieved, as they are potentially associated with serious complications according to their type and location. A 21–71% long-term serious morbidity and a 25% death rate was reported 169–173. Expected complications from a foreign body that is partially or entirely blocked in the right heart are ventricular arrythmia, myocardial infarction, myocarditis, recurrent pericardial effusion, tamponade and sepsis. Foreign bodies blocked in the pulmonary circulation may be responsible for thromboembolism and sepsis. Relative contra-indications of catheter retrieval are free floating thrombus attached to the foreign body and chronic incorporation of the foreign body in a thrombus or vessel wall.
Technique
Vascular foreign bodies are located with fluoroscopy and, when necessary, phlebographic demonstration. Extraction devices are relatively inexpensive and based on the loop-snare technique, helical basket entrapment or the grasping forceps technique or a combination of the above and other catheter-guide wire dislodgement techniques (fig. 14⇓). The procedure is carried out under fluoroscopic control and with local anaesthesia. Large and uncompressible foreign bodies may require a femoral venotomy for extraction. Large stents retrieved from a pulmonary artery or from the heart can be abandoned in an iliac vein.

{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
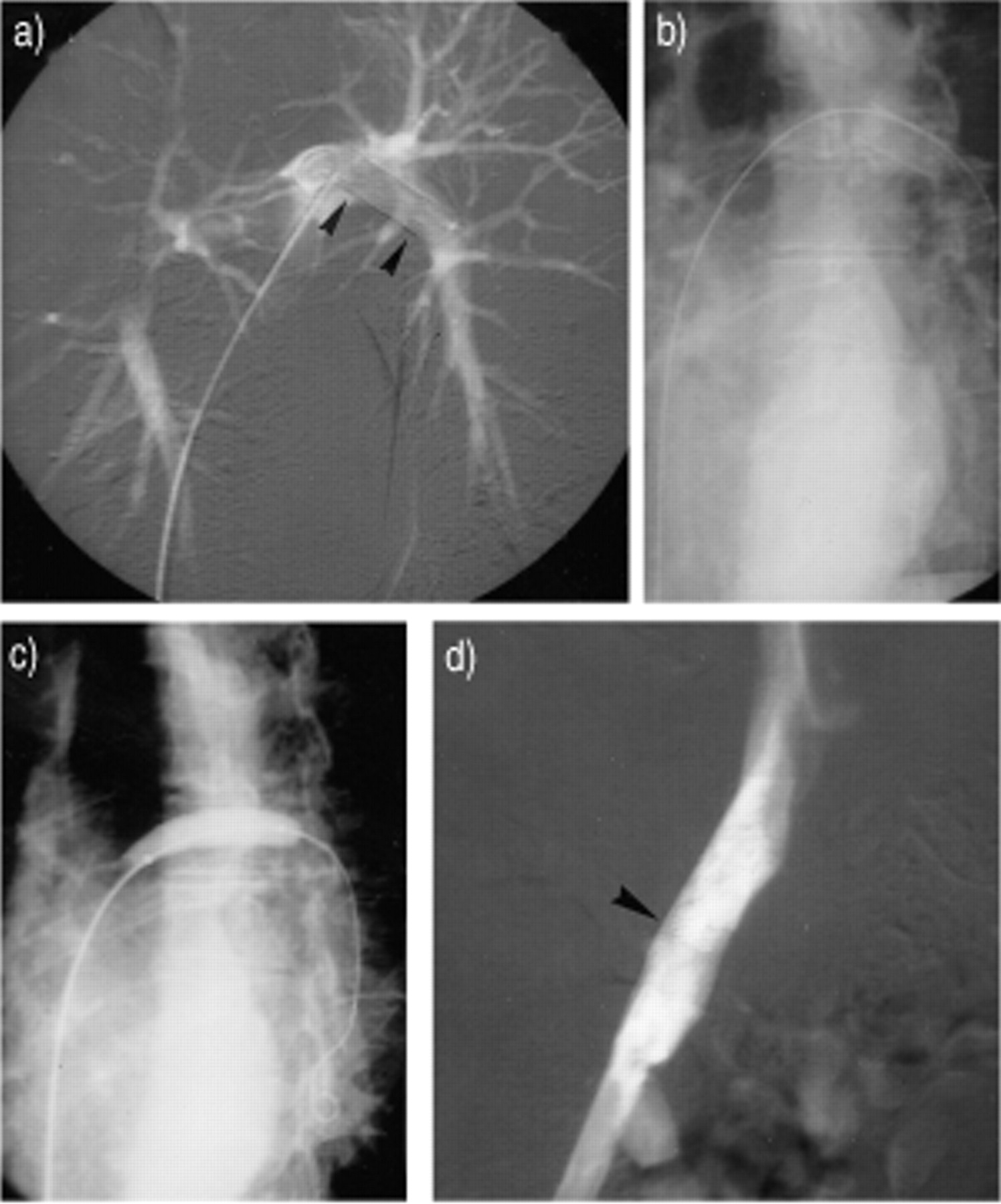
Percutaneous vascular foreign body retrieval. A 48-yr-old female. Stent placement in the right subclavian vein was attempted in another hospital. The metal stent had migrated to the left pulmonary artery. a) Pulmonary angiography shows a 4 cm fully expanded metal stent (arrowheads), blocked in the left inferior pulmonary artery. b) Foreign body retrieval was planned with a coaxial balloon extraction technique. The stent lumen was catheterized with a guidewire allowing insertion of a percutaneous transluminal angioplasty (PTA) catheter. c) Full inflation of a PTA balloon inside the stent, allowed atraumatic stent retraction in the iliac vein. d) The stent was abandoned in the right iliac vein, after balloon deflation, avoiding right femoral venotomy for extraction. Control phlebography shows optimal stent placement in the right iliac vein.
Results
The literature reports a success rate of >90% by a closed percutaneous retrieval 173. The procedure may fail, when no free ends of an endovascular line are available for snaring, when small catheter fragments are lodged too far in a small pulmonary artery branch or when small objects are incorporated in the wall of cardiac chambers, or lodged in a thrombosed vein or have perforated outside the venous wall. Failure of percutaneous extraction is obviated by early treatment, without waiting for clinical symptoms to occur. Complications from percutaneous retrieval are rare including transient arrythmia, further distal pulmonary embolization of a friable foreign body and thrombosis at the puncture site.
Endoluminal tracheobronchial stenting
Indications
Tracheobronchial airway obstruction is a relatively common condition. Various therapeutic options are available and depend on the cause (benign versus malignant), location (central versus peripheral) and origin (intrinsic versus extrinsic) of the stenosis. Patient's condition and the prognosis of disease are also considered. Whenever possible, in malignant obstruction or in benign stenosis, surgery is the first choice 174. With progress in technique, local treatment by bronchoscopy (laser, cryotherapy, electrocautery, photodynamic therapy, brachytherapy) has been used with increasing frequency 175–179. Balloon dilatation leads to a rapid improvement of the respiratory function after treatment of malignant and benign bronchial stenosis, but relief of symptoms is often short-lasting 180, 181. Therefore, indication of stents placement in the tracheobronchial tree has increased in frequency and can be placed under radiological or bronchoscopic control, or a combination of both modalities 181, 182. Compared to surgery, stent insertion is a simple palliative method, resulting in immediate improvement in acute respiratory distress from airway obstruction 181. In nonsurgical patients with malignant disease, indications of tracheobronchial stenting are: extrinsic compression or submucosal disease; tracheo-oesophageal fistula; and obstructive endobronchial tumour unresponsive to endobronchial treatment by debulging or resection, respectively 181–190. In benign stenosis, surgery may not be indicated in patients with a short life expectancy or extensive airway stenoses. Stent insertion for benign stenosis has been reported in the following conditions: iatrogenic (postintubation or postanastomotic stricture); tracheobronchial malacia in children; extrinsic compression from vascular structures or fibrosing mediastinitis; tracheobronchial infection (tuberculosis); and systemic disease (Wegener's granulomatosis, relapsing polychondritis and amyloidosis) 181, 182, 184, 190–196.
Technique
Precise measurements of the diameter of the tracheal and bronchial lumen and location of the stenosis compared to anatomical landmarks are performed with spiral CT before the procedure. Stents are inserted under sedation or anaesthesia, following previous dilatation or laser ablation of the stenosis under fluoroscopic and endoscopic control. Two types of endobronchial stents are currently available in the tracheobronchial tree: silicone stents (Dumon, Dynamic, Reynders, and others) 181–183, 186, 188, 190 and metallic stents, the latter including either balloon expandable stents (Palmaz and Strecker) or selfexpanding stents (Gianturco, Wallstent, Ultraflex) 181, 182, 187, 190, 192, 193, 197, 198. Most metallic stents are available in covered and noncovered versions. No ideal stent is currently available. The type of stent to be used is a matter of debate and is often dictated by availability and individual preference. Most metallic stents can be inserted on an outpatient basis.
Results
Placement of stents leads to an immediate and significant decrease in symptoms and an improvement in respiratory function in 80–95% of the patients. Most of the patients with severe respiratory impairment are able to be discharged following treatment. As results depend on optimal positioning of the prosthesis and some of the stents show a poor visualization under fluoroscopy, new advances in CT fluoroscopy are promising guiding techniques allowing precise and real time control of stent insertion in selected cases.
Complications
Complications are related to the type of stent, and include early or late stent migration (1–19%), infection (3–22%), deformation or breakage (1–36%) and stent obstruction by secretions, granulation formation or tumour overgrowth (6–21%). Other complications, such as major haemorrhage and tracheobronchial fistula are rare. New developments in stent configuration and composition seem to be associated with aneasier introduction and a lower rate of complications.
Conclusion
A close collaboration between interventional radiologists and pathologists, primary care physicians, pulmonologists, medical and radiation oncologists as well as thoracic surgeons is a prerequisite for optimal patient management, offering full therapeutic options. Future developments in imaging based patient management mainly concern oncological applications. Following preliminary studies on percutaneous treatment of inoperable or early non-small cell lung cancer, such as electrochemical polarization of cancer 199, new modalities are emerging including percutaneous brachytherapy 200 and radiofrequency tumour ablation 201. Interventional radiology will also be used for catheter or needle mediated immunomodulatory or gene therapy delivery to the target organs. Concerning stenting procedures, future types of stents include hybrid stents with metallic components and a smooth synthetic covering of silicone or polyurethane, biodegradable stents, chemically and radioactively coated stents 182, 202.
- Received October 10, 2000.
- Accepted December 27, 2000.
- © ERS Journals Ltd
References










Jump To
- Article
- Abstract
- Percutaneous nonvascular interventions
- Imaging guidance modalities
- Transthoracic needle biopsy
- Percutaneous drainage of thoracic fluid collections
- Vascular interventions
- Bronchial artery embolization
- Pulmonary artery embolization
- Percutaneous recanalization and stenting of the superior vena cava and innominate veins
- Percutaneous vascular foreign body retrieval
- Endoluminal tracheobronchial stenting
- Conclusion
- References
- Figures & Data
- Info & Metrics