





Abstract
Recent studies have demonstrated that blockade of P2X3 ATP receptors can profoundly inhibit chronic cough. We have considered whether inhaled ATP produces a tussive response and whether chronic cough patients are hypersensitive to inhaled ATP compared to healthy volunteers.
A standardised inhalational cough challenge was performed with ATP and AMP. We randomised 20 healthy volunteers and 20 chronic cough patients as to the order of challenges. The concentration of challenge solution causing at least five coughs (C5) was compared for ATP and AMP.
The study population consisted of six male and 14 female volunteers in each group. Two out of 19 healthy volunteers coughed with AMP (one volunteer could not take part in this challenge) and none reached C5. Eight out of 20 chronic cough patients coughed with AMP and two reached C5. Of the 20 healthy volunteers, 18 coughed with ATP, with 15 reaching C5. All 19 chronic cough patients completing the ATP challenge coughed with ATP and 18 reached C5. The chronic cough patients had a greater cough response at lower concentrations of ATP.
The greater potency of ATP versus AMP in the inhalational challenge suggests that tussive responses are mediated through members of the P2X purinergic receptor family. This acute effect was, however, not sufficient to explain cough hypersensitivity syndrome.
Abstract
Chronic coughers have a heightened response to ATP but not sufficient to implicate ATP in cough hypersensitivity http://ow.ly/h15730699GA
Introduction
Chronic cough (arbitrarily defined as a cough lasting more than 8 weeks) is a common presentation to general practitioners and respiratory outpatient clinics. A recent systematic review of 90 studies found the overall global prevalence of chronic cough to be 9.6% in the general population [1].
It is now widely accepted that, with rare exceptions, in chronic cough there is hypersensitivity of the vagal afferent nerves or an alteration of the central processing of their input, regardless of the underlying aetiology of the cough. In hypersensitivity, even trivial stimulation of these sensory nerves leads to the urge to cough. The cause of this hypersensitivity is not fully understood but the concept of cough hypersensitivity syndrome (CHS) is widely agreed upon in the respiratory community [2–4].
The nerves of the vagal afferent limb of the cough reflex are myelinated a-delta fibres and un-myelinated C-fibres [5]. The involvement of the terminals of these nerves in generating cough is better evidenced in animals than in humans, although recent studies suggest that similar structures can be visualised in humans [6].
The sensory receptors involved in activating these nerve endings are of great interest as potential therapeutic targets in chronic cough. Objective demonstration of hypersensitivity could lead to the development of diagnostic tests for CHS. Chronic cough patients have been found to be hypersensitive to established cough challenges such as capsaicin [7, 8] and citric acid [9]. However, the wide normal range of cough sensitivity to these agents makes them unsuitable as a diagnostic tool. The recent demonstration that the blockade of ATP that prefer purinergic receptors leads to a markedly reduced cough frequency in chronic cough [10] suggests that ATP could be a key mediator of cough hypersensitivity; thus, ATP challenge could differentiate between a normal cough reflex and cough hypersensitivity. Two classes of purinergic receptors have been characterised: P1 and P2. The P1 receptors are activated by adenosine and AMP whereas P2 receptors respond to ATP.
To explore the hypothesis that P2 receptor activation underlies cough hypersensitivity, we have compared cough challenge in two groups: healthy volunteers and patients with CHS. We also quantified the cough response to AMP (P1) and ATP (P2).
Methods
This was a randomised, controlled crossover trial of cough challenge with ATP and AMP. Twenty patients with CHS were recruited from the Hull Cough Clinic and the Hull Respiratory Clinical Trials Unit (CTU) database of chronic cough patients. Twenty gender-matched healthy volunteers were recruited from departmental staff and the CTU database of volunteers. We recruited the first participant in January 2015 and the last cough challenge was completed in May 2015.
Healthy volunteers had no evidence of cough hypersensitivity, as demonstrated by a Hull Airways Reflex Questionnaire (HARQ) score of less than 13. Chronic cough patients had cough hypersensitivity, as demonstrated by a HARQ score of 20 and above.
All participants were current non-smokers who had been stable on medication for at least a month. Excluded were volunteers who had a recent upper respiratory tract infection or cough/asthma exacerbation within the last 3 weeks.
Participants received two cumulative cough challenges in the CTU, one with ATP and one with AMP (Sigma-Aldrich Company Ltd, Dorset, UK). We used 0.9% saline as the solvent for the ATP and AMP. We chose to use AMP because of the insolubility of adenosine in saline. ATP was readily soluble in saline at a maximum concentration of just over 0.3 M. As a result, this concentration was chosen as the maximum concentration for both challenge solutions.
The stability of ATP and AMP in solution was confirmed using high-performance liquid chromatography analysis at the Department of Chemistry, University of Hull. Both challenge solutions were found to be stable in solution for at least 72 h. They were made up by a laboratory technician in single aliquots and when not used on the same day were stored in a refrigerator at 4°C.
The two challenges were administered on different days, at least 48 h apart. The order in which the challenges were administered was randomised using a computer-generated randomisation system (Sealed Envelope; Sealed Envelope Ltd, London, UK). The order of administration was double-blind and the two challenge substances looked identical once made up.
The cough challenge was adapted from European Respiratory Society standardised cough challenge methodology [11]. A single inhalation of each dose of challenge solution was delivered using a Ko-Ko digidoser (Sigma-Aldrich) with flow limiter, after maximal exhalation. All challenges started with a saline inhalation. ATP or AMP was then delivered in increasing concentrations on a half-log scale from 0.1 to 300 mM. Coughs were counted by the cough challenge administrator in the first 15 s after each inhalation. There was at least 1 min between each inhalation. Participants were asked to avoid caffeine and menthol for 1 h prior to each cough challenge.
The challenge was terminated once the participant coughed at least five times following an inhalation or reached the maximal concentration available. Comments about sensation evoked during the challenge were not actively sought, but were noted if the participants volunteered them.
Participants received their second challenge at a similar time of day. If the patient experienced changes in health between the challenges these were noted, and if this was an upper respiratory tract infection, the second challenge was delayed.
Because the effects of these challenge solutions were previously unknown it was impossible to create an accurate power calculation. However, multiple previous studies done in the Hull CTU in both normal volunteers and chronic cough patients have demonstrated a significant change in the concentration of substance which elicited at least two coughs (C2) and five coughs (5C) using 20 subjects.
The primary outcome measures were the difference in C2 and C5 between ATP and AMP, and between healthy volunteers and chronic cough patients. Statistical analysis was performed using SPSS (SPSS Inc., Chicago, IL, USA). Differences in the number of patients reaching C2 and C5 in the ATP and AMP challenges within each group were assessed using McNemar's test for related data. For purposes of statistical analysis during a comparison between the two groups of participants, if C2 or C5 was not reached the maximum concentration was set at 1000 mM. Comparisons of C2 and C5 between the healthy volunteers and the chronic cough patients were made using a t-test.
Ethical approval to complete this study was obtained from the National Research Ethics Committee (REC reference: 14/SS/1071). The study is registered on ClinicalTrials.Gov (NCT02039999).
Results
Demographics
The healthy volunteer group and chronic cough patient groups were matched for gender with 14 women in each. The majority of the participants were Caucasian, with two non-Caucasians in the healthy group and one in the patient group. The chronic cough patients were older, at 27–83 years versus 23–74 years. The forced expiratory volume in 1 s (FEV1) as a percentage of predicted was also lower in the chronic cough group, with a median of 88% versus 101%.
All patients in the healthy volunteer group had a HARQ score of between 0 and 8. The chronic cough patient group's HARQ scores varied between 21 and 52. Full details are shown in table 1.
Demographics
Comorbidities
Nine of the healthy volunteers self-reported comorbidities. All the chronic cough patients had comorbidities. Gastrointestinal disturbances (both upper and lower), inflammatory disorders such as arthritis and vasculitis, hypertension, and other respiratory conditions were more common in the patient group.
Medications
The patient group were taking more medications. One participant in each group was taking angiotensin-converting enzyme (ACE) inhibitors. One healthy volunteer was taking anti-reflux medication, compared to 11 in the cough group.
Healthy volunteers cough challenge
Two out of 19 healthy volunteers coughed with AMP (one healthy volunteer was not challenged with AMP owing to an adverse event with the previous challenge). One of these reached C2, and none reached C5. In total there were only four coughs throughout the AMP challenges.
Two healthy volunteers did not cough at all in response to the ATP challenge. The remaining 18 all reached C2, with 15 reaching C5. The differences in the number of patients reaching C2 or C5 between the ATP and AMP challenges was statistically significant (p<0.01 for both). The results of the individual healthy volunteers cough challenges to ATP are shown in supplementary figure S1.
Chronic cough patients
Ten of the chronic cough patients coughed at least once in response to AMP. Of these, eight reached C2 and two reached C5. Within-individual cough responses were erratic. Having coughed at least twice, patients often did not cough at higher concentrations. These findings are shown in supplementary figure S2.
In total, 19 patients completed the ATP challenge; one patient withdrew prior to administration. All of these patients coughed in response to ATP and all reached C2. One patient did not reach C5, coughing four times at the two highest concentrations (supplementary figure S3). All patients who reached C5 did so by a concentration of 100 mM. The C5 in chronic cough patients was mainly distributed between 1 mM and 100 mM.
Two patients who reached C5 for both the AMP and ATP challenges achieved C5 for ATP at half a log below the C5 concentration of AMP.
The difference between C2 and C5 for ATP and AMP was statistically significant (p<0.01 for both).
Whereas none of the healthy volunteers coughed in response to the initial inhalation of saline, six of the chronic cough patients did. They all only coughed in response to saline prior to one of their challenges. This was not consistently on their first exposure to a cough challenge.
Comparing healthy volunteers and chronic cough patients
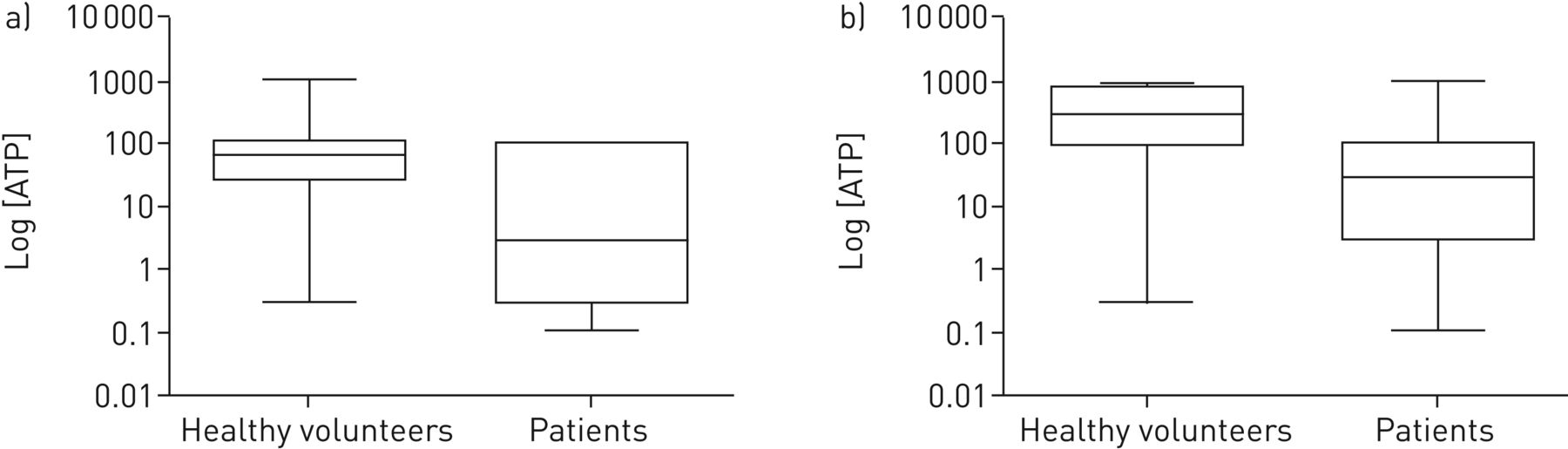
The distribution of the C2 and C5 for ATP in healthy volunteers and chronic cough patients is outlined in figure 1. The C2 for ATP was statistically significantly different between the healthy volunteers and the patients (p=0.047). This was also the case for C5 (p<0.01). The average number of coughs at each concentration of ATP for healthy volunteers and chronic cough patients is compared in figure 2.

Box and whisker plots showing distribution of a) C2 and b) C5 during adenosine triphosphate (ATP) challenge in healthy volunteers compared to chronic cough patients. C2: the concentration of ATP causing at least two coughs; C5: the concentration of ATP causing at least five coughs.

{kind=link}
{kind=link}
Comparison of mean coughs to each concentration of adenosine triphosphate (ATP) in healthy volunteers and chronic cough patients.
Adverse events
One healthy volunteer had an episode of urticaria in the 24 h following inhalation of the ATP challenge and was withdrawn from the study. There was one episode of wheeze following AMP in a chronic cough patient, which resolved following administration of inhaled salbutamol. One patient withdrew after their first challenge because they felt that their cough had increased in the days after the challenge.
Participants in both groups informally reported that they had throat irritation which lasted for up to several hours after the ATP challenge.
Discussion
When comparing healthy volunteers with chronic cough patients, the patient group coughed significantly more, and at lower concentrations of ATP. However, the degree of hypersensitivity demonstrated by our patient group to ATP does not appear to be any more than previously seen in other cough inhalational challenges [9, 11, 12]. This suggests that chronic cough patients do not have an intrinsically heightened sensitivity to ATP and, thus, it is not the acute, peripheral response to ATP that underlies cough hypersensitivity in these patients.
The use of citric acid as a tussive challenge in humans was first described by Bickerman and Barach in 1954 [13]. Since then, the technique has been used in a number of different settings with different tussive agents. The most commonly used are citric acid, capsaicin and fog challenge. These challenges stimulate cough by acting on different peripheral nerve receptors in the airways. Capsaicin is known to stimulate TRPV1 receptors on sensory afferent C-fibres [14]; citric acid shows some cross-reactivity with a number of receptors on C-fibres and also a-delta fibres [15]; whereas the specific receptors stimulated by the low chlorine solution of a fog challenge are poorly defined [16]. Other receptors implicated in the cough response are more difficult to stimulate with an inhalational challenge given the nature of the ligands involved; however, cinnamaldehyde has been shown to cause cough in humans and supports the involvement of the TRPA1 receptor in the cough reflex [17].
One hypothesis for the cause of hypersensitivity in chronic cough patients is that there is an up-regulation in one or more of the peripheral receptors of the afferent limb of the cough reflex [18]. The blockade of receptors stimulated by cough challenges are therefore of interest as therapeutic targets. In animal studies, there has been some success in reducing cough by antagonising these receptors [19, 20]. However, this success has not been replicated in human trials of TRPA1 (personal communication) and TRPV1 receptors [21], suggesting that these afferent sensory receptors, which are undoubtedly important in the sensation of irritation stimulating cough, are not the root cause of cough hypersensitivity.
A number of different lines of evidence now point to the purinergic system as being the most likely mechanism for inducing afferent hypersensitivity. ATP, acting through a class of purinergic receptors, was first postulated as an extracellular signalling molecule by Burnstock in 1972 [22]. It took a number of years for this mechanism to become established, and the role of ATP as an extracellular signal was not widely accepted until the 1990s when the first purinergic receptors were cloned [23, 24].
A number of findings support the presence of ATP-responsive P2 receptors within mammalian lungs. P2X3 receptors are thought to be mainly responsible for the effects of ATP in the lung, which have been demonstrated using immunohistochemistry on sensory nerve endings [25]. These receptors are found as either homotrimeric P2X3 receptors or heterotrimeric P2X2/3 receptors [26]. Vagal C-fibres can be stimulated by ATP via heteromeric P2X2/3 receptors [27].
The responses of peripheral neurons to ATP vary within the same ganglia, between different types of ganglia and within species. The response appears to be consistently due to the effect of ATP on P2X2 and P2X3, but there is probably a difference in the proportion of homo/hetero types of receptor expressed [26]. Of relevance to cough hypersensitivity is the observation that activation of P2X2/3 heterodimers produces a prolonged current, whereas stimulation of P2X3 receptors produces a rapidly inactivating current [28]. A recent study has, however, suggested that prolonged activation of the P2X3 receptor can be achieved by TRPV4 activation of pannexin, causing the continuous stimulation of P2X3 and thus leading to prolonged hypersensitivity [29].
Animal studies considering the role of ATP and P2X receptors in cough have been limited to guinea pigs, in which inhaled ATP accentuated the subsequent citric acid challenge response. ATP alone failed to stimulate cough and antagonist studies implicated the P2X4 receptor in this species [30].
In humans, intravenous ATP administered to palliative care patients caused breathlessness as its most common side effect [31]. Inhaling ATP has previously been noted to cause cough, although this response has not been systematically characterised. Prolonged inhalation of ATP causes bronchoconstriction in both healthy and asthmatic volunteers, with a greater response in the asthmatic individuals [32, 33]. Inhalation challenges using ATP and AMP in patients with chronic obstructive pulmonary disease, in smokers and in healthy volunteers found that ATP appeared to cause increased breathlessness and cough compared to AMP [34].
The lack of a significant cough response to inhaled AMP in our healthy participants seems to be in contrast with previous studies. This could be due to methodological differences given the brief exposure of our participants, a consequence of the use of the single-breath inhalation method. While the majority of our healthy volunteers coughed with ATP, two did not. This is in keeping with experiences with other cough challenges, such as citric acid and capsaicin, in which a proportion of healthy volunteers do not cough within the range of the challenge. ATP challenge does not appear, therefore, to be exceptional in its sensitivity or persistence. Thus, while our findings support the importance of purinergic receptors in the normal cough reflex pathway, it is not possible to differentiate between P2X3 and P2X2/3 receptors as the main modulators of this tussive response to ATP.
AF-219 (a P2X3 receptor antagonist) (Afferent Pharmaceuticals, San Mateo, CA, USA) has been trialled in a phase 2 study and has been found to dramatically reduce 24 h cough counts after 2 weeks of administration in patients with chronic cough [10]. Our data would tend to support the hypothesis that, while P2X3 receptor activation could be the final common pathway producing hypersensitivity, acute activation of the receptor does not infer this state on afferent nerves, and that other mechanisms such as activation of TRPV4/pannexin are required.
Our study has several limitations. Our two study populations were gender matched because of the known influence of gender on cough reflex sensitivity. They were, however, not age matched and our patient group was older than our healthy volunteer group. Although chronic cough is more prevalent in older patients [35], this does not seem to influence the cough reflex but rather the increased prevalence of the underlying cough-provoking conditions in older patients. Previous studies have shown no influence of age on the cough reflex, as opposed to a comorbidity such as dementia [36].
Comorbidities were also more prevalent in the patient group. The majority of these were conditions that are often associated with cough, such as gastro-oesophageal reflux disease, asthma and post-nasal drip as well as irritable bowel syndrome and lymphoedema. These comorbidities were self-reported by patients. One participant in each group was taking ACE inhibitors, and while this could have influenced the cough threshold, these individuals did not appear as outliers.
Within the population of 40 participants, we only had one adverse effect to ATP. This urticarial rash appears to have been a hypersensitivity reaction.
Given that some of our participants commented on ongoing throat irritation after the challenge was completed, ATP could potentially be involved in cough hypersensitivity via mechanisms other than a direct pro-tussive effect.
Conclusion
We believe that this is the first study to compare an objective cough response to inhaled ATP and AMP in healthy volunteers and chronic cough patients. The response to ATP in chronic cough appears to be heightened, but not to such a degree as to implicate an acute response to inhalation of ATP in the pathophysiology of cough hypersensitivity syndrome.
Supplementary material
Supplementary Material
Please note: supplementary material is not edited by the Editorial Office, and is uploaded as it has been supplied by the author.
Figure S1. Number of coughs at each concentration of adenosine triphosphate in 20 individual healthy volunteers. N/S: normal saline; ATP: adenosine triphosphate. ERJ-01452-2016_Supplementary_Fig_S1
Figure S2. Number of coughs at each concentration of adenosine monophosphate in 20 chronic cough patients. N/S: normal saline; AMP: adenosine monophosphate. ERJ-01452-2016_Supplementary_Fig_S2
Figure S3. Number of coughs at each concentration of adenosine triphosphate in 19 chronic cough patients. N/S: normal saline; ATP: adenosine triphosphate. ERJ-01452-2016_Supplementary_Fig_S3
Disclosures
Acknowledgements
Authors are indebted to all volunteers and patients who participated in the study. Special thanks to all staff in the Respiratory Clinical Trials Unit, Castle Hill Hospital, particularly Joseph Howard, Zainab Rai, Chris Crow and Juozas Domarkas, for assistance with cough challenge administration and laboratory support.
Footnotes
This article has supplementary material available from erj.ersjournals.com
Clinical trial: This study is registered at ClinicalTrials.gov with identifier number NCT02039999.
Conflict of interest: Disclosures can be found alongside this article at erj.ersjournals.com
- Received July 21, 2016.
- Accepted November 2, 2016.
- Copyright ©ERS 2017
References










